Mandible & maxilla
Benign odontogenic tumors
Adenomatoid odontogenic tumor
Editorial Board Member: Marc Pusztaszeri, M.D.
Deputy Editor-in-Chief: Kelly Magliocca, D.D.S., M.P.H.


Last author update: 11 December 2023
Last staff update: 26 March 2024
Copyright: 2004-2025, PathologyOutlines.com, Inc.
PubMed Search: Adenomatoid odontogenic tumor
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1Cite this page: Goldfaden JS, Bilodeau EA. Adenomatoid odontogenic tumor. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/mandiblemaxillaadenomatoid.html. Accessed September 2nd, 2025.
Definition / general
- Benign, rare tumor of odontogenic origin
- Encapsulated, characterized by spindled or cuboidal epithelium forming a nodular pattern, with duct-like structures resulting in cribriform areas; eosinophilic amyloid and calcifications may be seen (Head Neck Pathol 2021;15:71)
Essential features
- Adenomatoid odontogenic tumors (AOTs) are most common in the anterior region of the jaws in young female patients associated with impacted teeth (J Nat Sci Biol Med 2013;4:457)
- Microscopically, AOTs contain spindled, cuboidal, polygonal epithelium, forming duct-like structures, whorls and cribriform architecture surrounded by a thick capsule
- Eosinophilic matrix may be seen, which can calcify (Oral Surg Oral Med Oral Pathol Oral Radiol 2022;133:675)
- Also called the tumor of two - thirds as two - thirds of cases occur in female patients in the maxilla, surrounding an impacted tooth (Oral Oncol 1999;35:125, Surg Pathol Clin 2017;10:177)
Terminology
- Historic terminology (no longer appropriate) includes adenoameloblastoma, adenoameloblastic odontoma, adenomatoid ameloblastoma, pseudoadenomatous ameloblastoma (J Oral Pathol Med 1991;20:149)
- In 1971, the World Health Organization (WHO) adopted terminology proposed by Philipsen and Birn: adenomatoid odontogenic tumor (Acta Pathol Microbiol Scand 1969;75:375)
ICD coding
Epidemiology
- 2.2 - 7.1% of all odontogenic tumors (J Oral Med Oral Surg 2021;27:19, J Oral Pathol Med 2007;36:383)
- 87.2% occur in the second or third decade of life but may occur across wide age range
- ~2:1 female predilection
- 3 variants of AOT are follicular (pericoronal), extrafollicular and peripheral (J Oral Pathol Med 2007;36:383)
- Follicular variant accounts for ~71% of all cases
- Extrafollicular (extracoronal) variant accounts for ~27% of cases
- Peripheral (extraosseous) variant accounts for 2% of all cases
Sites
- Anterior maxilla is the most affected (66.6%) (Head Neck Pathol 2012;6:430)
- ~42% of cases are associated with impacted maxillary canines (J Oral Pathol Med 1991;20:149)
- There is a significant predilection for the anterior region (93.3%), with only 6.7% of cases affecting the posterior area, exclusively in the mandible (Head Neck Pathol 2012;6:430)
Pathophysiology
- KRAS mutations and MAPK pathway activation are commonly implicated in the pathogenesis in AOT
- In one series, 71% (27/38) of AOT cases expressed KRAS codon 12 mutations (Mod Pathol 2019;32:799)
Clinical features
- Usually an asymptomatic swelling (unless secondarily infected)
- Tooth displacement may be present
Diagnosis
- May be detected radiographically as an incidental finding or present as clinical swelling
Radiology description
- Most commonly (~75%) appear as well defined, unilocular radiolucencies (J Oral Pathol Med 2007;36:383)
- May also appear as mixed density or opaque lesions
- Encompass impacted teeth and extend beyond the cementoenamel junction and sometimes continue to the apex (Quintessence Int 2022;53:260)
Radiology images
Images hosted on other servers:

Radiolucency, engulfing tooth, extending beyond crown
Prognostic factors
- Prognosis excellent, few recurrences (< 5% documented)
Case reports
- 17 year old girl with a 2 cm maxillary lesion surrounding an impacted canine tooth (Case #490)
- 18 year old woman with nonpainful lesion of right anterior maxilla (Anticancer Res 2013;33:2673)
- 28 year old man with impacted tooth (Arch Pathol Lab Med 2003;127:e173)
- 31 year old man with cystic radiolucent lesion of the right mandible (J Oral Med Oral Surg 2021;27:19)
Treatment
- Generally treated by surgical enucleation
- Cases of large lesions that have caused significant bone loss and thinning are often managed by insertion of a drain or via marsupialization (Maxillofac Plast Reconstr Surg 2014;36:173)
- Both surgical and orthodontic modalities can be used to preserve the associated impacted tooth (Maxillofac Plast Reconstr Surg 2014;36:173)
Gross description
- 1 - 3 cm in size, unicystic with a thick capsule and soft tissue filling most of the cystic space
Microscopic (histologic) description
- Epithelium may appear nodular, trabecular, cribriform and form duct-like structures
- Cells may be spindly, cuboidal or columnar with the nuclei palisading away from the lumen
- Lesion is enclosed in a thick capsule
- Amyloid deposits may be present (Quintessence Int 2022;53:260)
- Calcifications may be seen
- Calcifying epithelial odontogenic tumor (CEOT)-like areas may be seen
- AOT - CEOT hybrid lesions have been described as distinct entities; these are customarily considered to be an AOT variant, with the clinical behavior of AOT
- References: Head Neck Pathol 2017;11:519, Oral Oncol 2005;41:835
Microscopic (histologic) images
Contributed by Elizabeth Ann Bilodeau, D.M.D., M.D., M.S.Ed. and Kelly Magliocca, D.D.S., M.P.H. (Case #490)
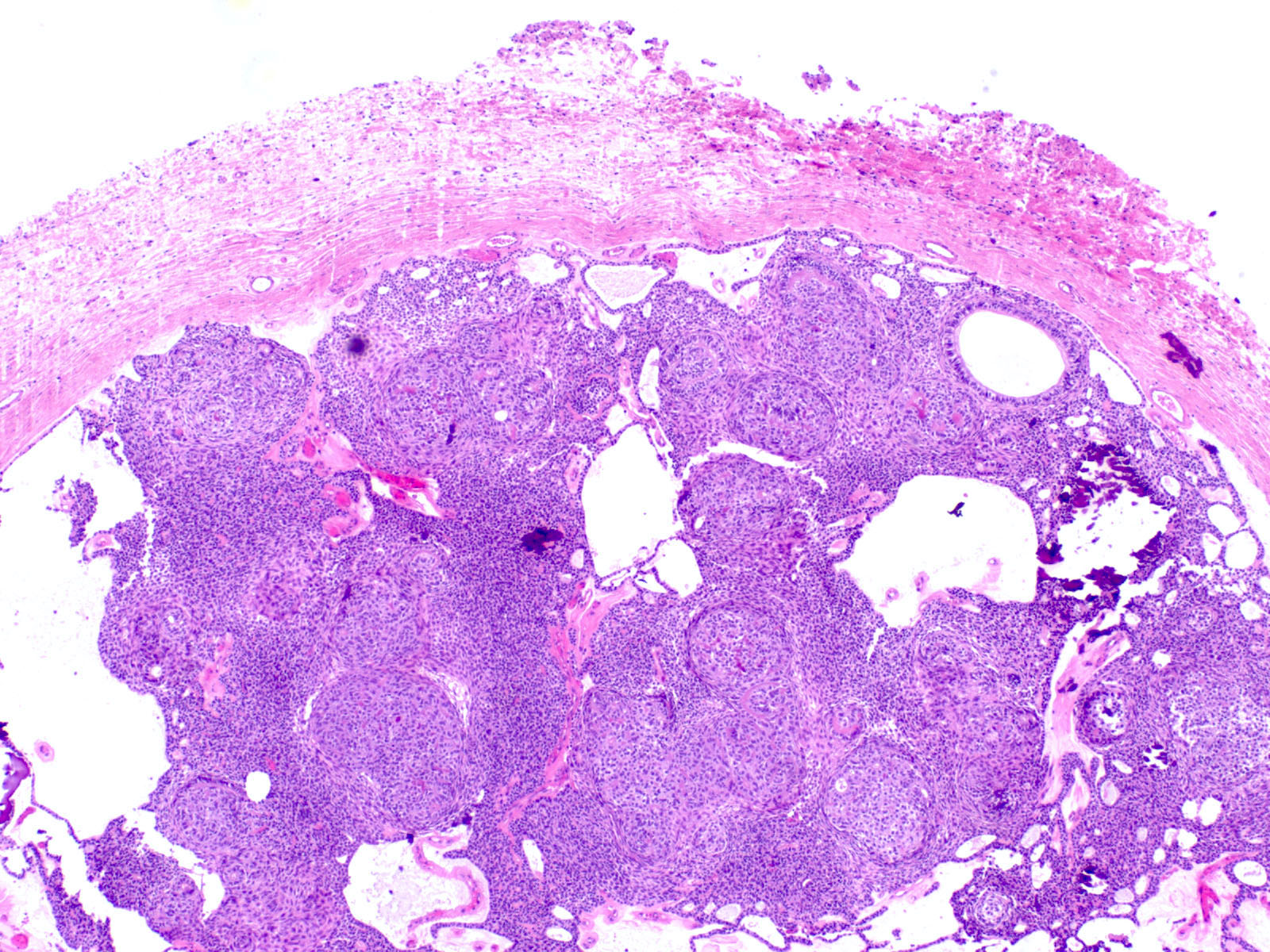
Thick fibrous capsule
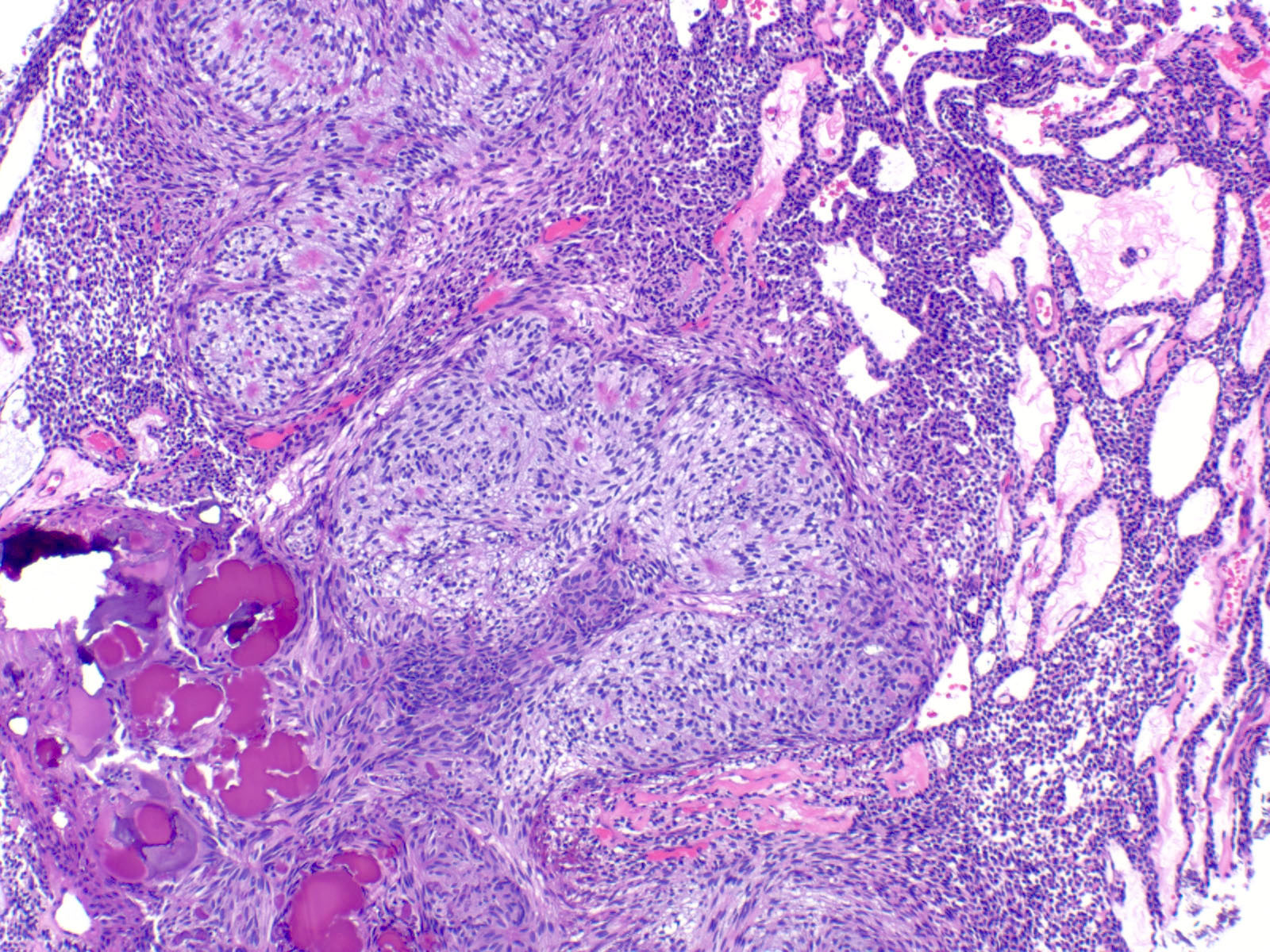
Cribriform areas
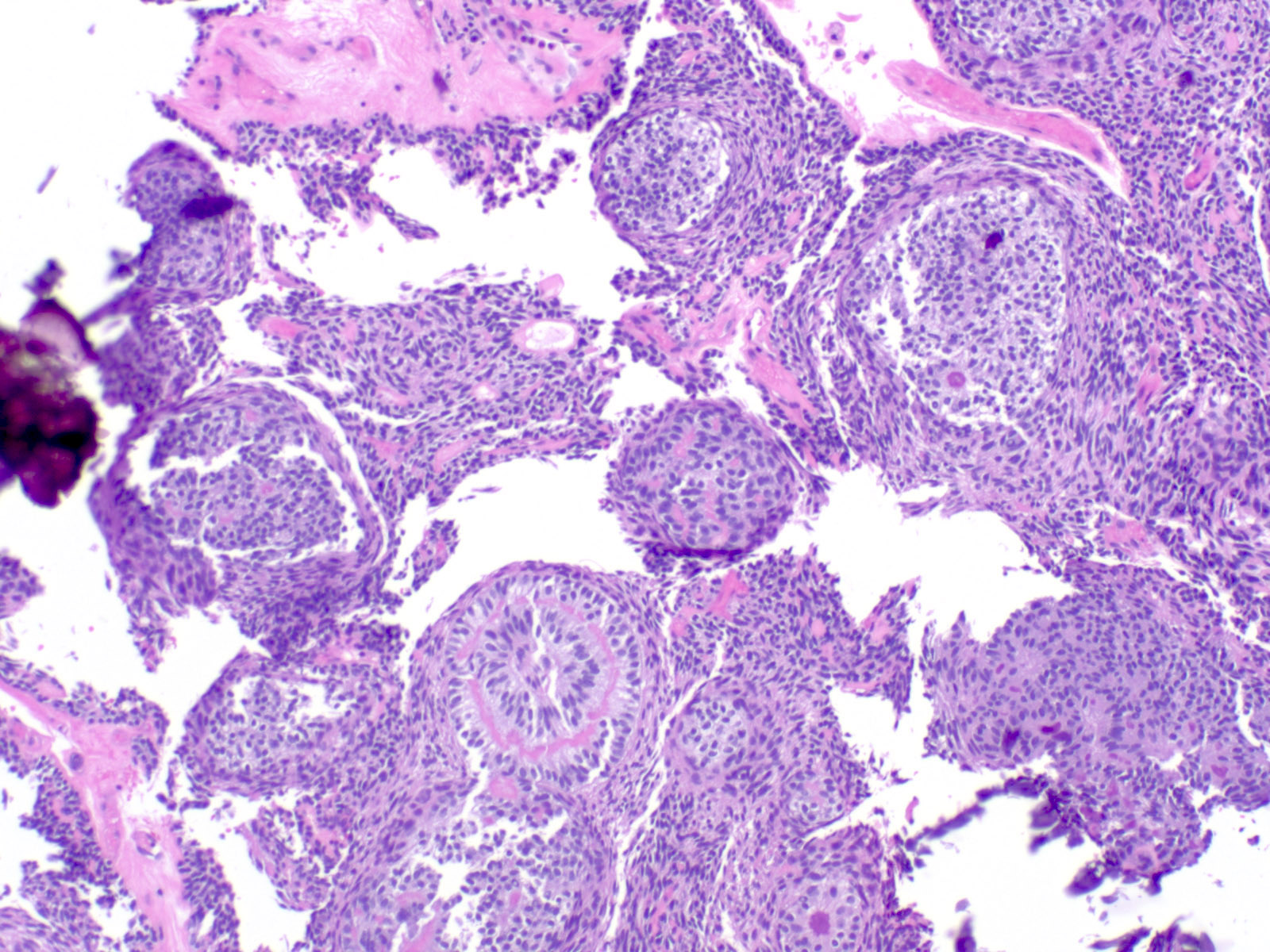
Rosette-like structure
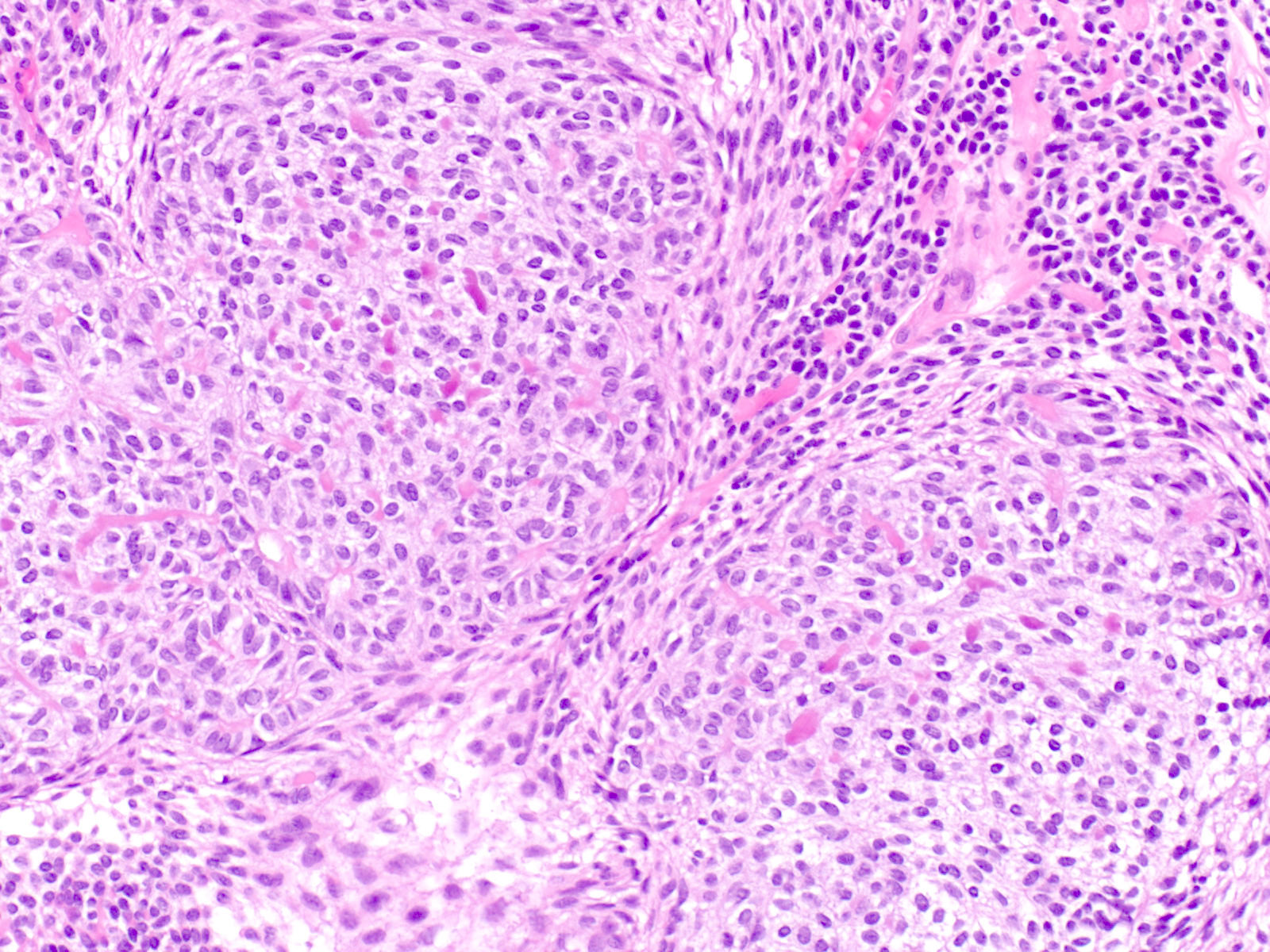
Cellular area with focal matrix deposition
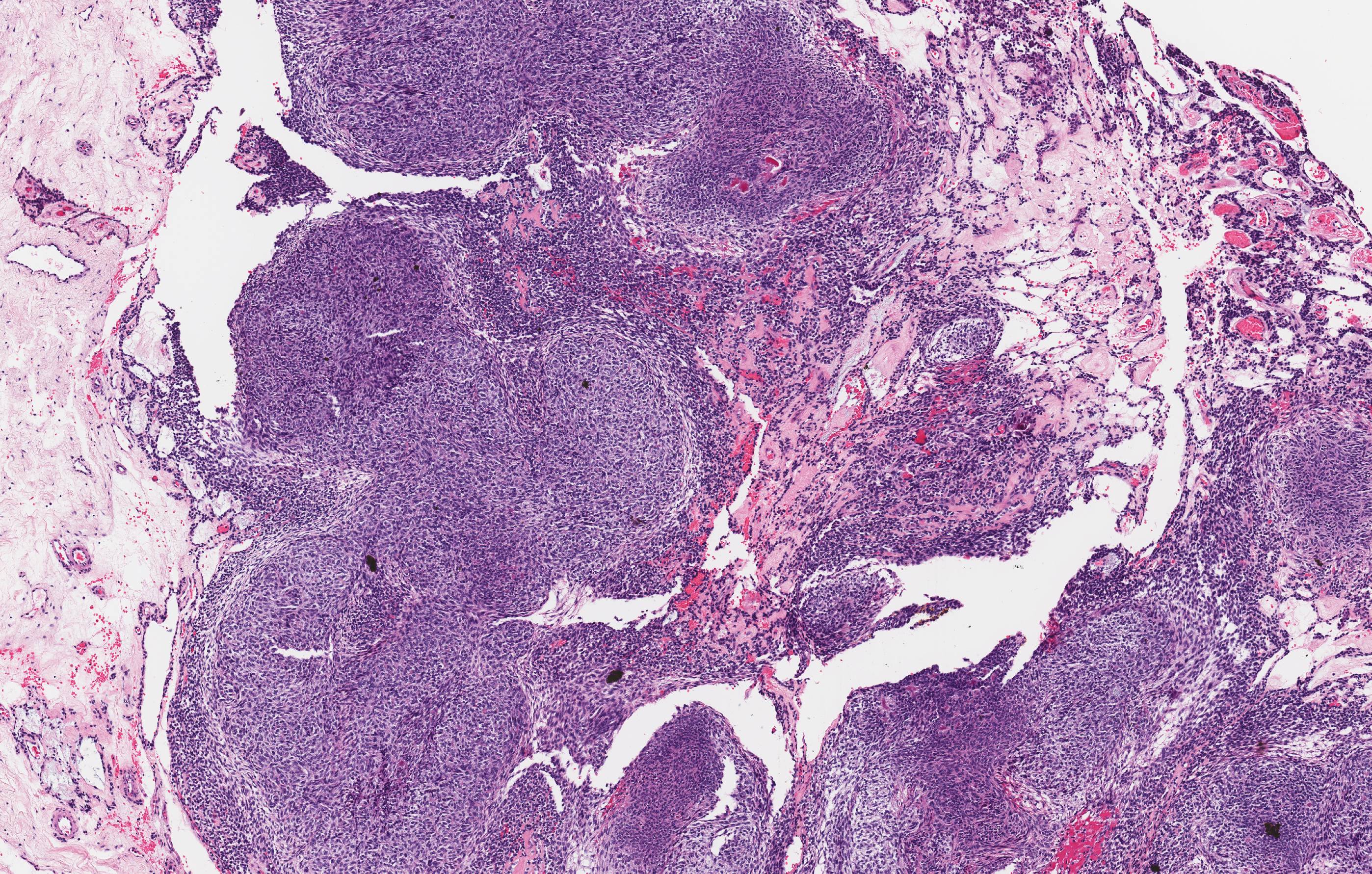
Nodular appearance

Thick capsule
Positive stains
- AE1 / AE3 (Oral Surg Oral Med Oral Pathol Oral Radiol 2022;133:675)
- CK5, CK17 and CK19 (J Oral Pathol Med 2003;32:55)
- Congo red may highlight focal amyloid deposits, especially in CEOT-like areas (Oral Oncol 2005;41:835)
Molecular / cytogenetics description
- KRAS mutations and MAPK pathway activation are commonly implicated in the pathogenesis of AOT (Mod Pathol 2019;32:799)
Sample pathology report
- Anterior maxilla, left, excisional biopsy:
- Adenomatoid odontogenic tumor, 1.8 cm
Differential diagnosis
- Adenoid ameloblastoma:
- May have extensive dentinoid clear cells and occasional ghost cells
- Morules / whorls, duct-like structures may be seen
- Lacks thick capsule, radiographically often not well defined
- Calcifying cystic odontogenic tumor:
- Ameloblastic epithelium and ghost cells
- Lacks whorls, duct-like structures and cribriform architecture
- Calcifying epithelial odontogenic tumor:
- Sheets of polygonal cells with pleomorphism and prominent intercellular bridging
- Lacks architectural pleomorphism (whorls, cribriform, duct-like pattern)
Additional references
Practice question #1
A 16 year old girl presents with a lesion associated with an impacted maxillary canine. Based on the photomicrograph, what is the lesion?
- Adenomatoid odontogenic tumor
- Ameloblastoma
- Calcifying cystic odontogenic tumor / calcifying odontogenic cyst
- Calcifying epithelial odontogenic tumor
Practice answer #1
A. Adenomatoid odontogenic tumor. The photomicrograph depicts nodular islands and duct-like structures with interspersed calcifications surrounded by a thick fibrous capsule. Answer B is incorrect because ameloblastomas are characterized by ameloblastic epithelium with reverse polarity away from the basement membrane but nodular architecture, encapsulation, calcifications and duct formation are not seen. Answer C is incorrect because calcifying cystic odontogenic tumors / calcifying odontogenic cysts have ameloblastic epithelium, varying numbers of ghost cells and calcifications, lacking the nodular architecture seen. Answer D is incorrect because calcifying epithelial odontogenic tumors lack encapsulation and have sheets, nest and cords of polygonal, pleomorphic cells that exhibit prominent intercellular bridging and amyloid with concentric calcifications.
Comment Here
Reference: Adenomatoid odontogenic tumor
Comment Here
Reference: Adenomatoid odontogenic tumor
