Mandible & maxilla
Cysts of the jaw
Calcifying odontogenic cyst
Resident / Fellow Advisory Board: Kyle Devins, M.D.
Deputy Editor-in-Chief: Kelly Magliocca, D.D.S., M.P.H.

Last author update: 13 August 2021
Last staff update: 20 July 2023
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Calcifying odontogenic cyst
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2 | Practice question #3 | Practice answer #3Cite this page: Bilodeau EA, Hunter KD. Calcifying odontogenic cyst. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/mandiblemaxillacalcifyingodontogenic.html. Accessed September 14th, 2025.
Definition / general
- Benign cyst of odontogenic origin, characterized by an ameloblastoma-like epithelial lining containing ghost cells that may calcify
- Originally described by Gorlin and colleagues in 1962 as a possible oral analogue to pilomatrixoma of skin, owing to the presence of ghost cell keratinization in both lesions
Essential features
- Calcifying odontogenic cysts are located most commonly in the anterior regions of jaws
- Microscopically calcifying odontogenic cysts contain an ameloblastoma-like epithelial lining containing ghost cells that may calcify
- Calcifying odontogenic cysts are associated with β catenin (CTNNB1) mutations
Terminology
- Calcifying odontogenic cyst (COC) is the preferred terminology in the 2017 WHO classification
- Nomenclature has been continuously changing, due to debate as to whether COC is a neoplasm or a developmental cyst
- In 1992, WHO classified this lesion as an odontogenic tumor but continued to use the term calcifying odontogenic cyst
- In 2005, WHO redesignated the lesion as calcifying cystic odontogenic tumor (CCOT)
- In 2017, the term calcifying odontogenic cyst was reapplied to this lesion and it was reclassified as a benign odontogenic cyst
- Other archaic names include Gorlin cyst and keratinizing and calcifying odontogenic cyst
- Given the diversity of the histopathologic features seen in COC and its tendency to coexist with other odontogenic lesions, complex classification systems have been proposed (Am J Surg Pathol 2003;27:372, J Oral Pathol Med 2008;37:302, Reichart: Odontogenic Tumors and Allied Lesions, Illustrated Edition, 2004)
- COC belongs to odontogenic ghost cell family of lesions (J Oral Pathol Med 2008;37:302)
- From a practical standpoint, a spectrum of histopathologic patterns exists, ranging from a benign lesion that is primarily cystic, a benign lesion with a solid pattern of growth to a rare tumor with features of carcinoma
- Solid lesions are designated dentinogenic ghost cell tumors in the 2017 WHO classification
- Malignant counterpart is ghost cell odontogenic carcinoma
- From a practical standpoint, a spectrum of histopathologic patterns exists, ranging from a benign lesion that is primarily cystic, a benign lesion with a solid pattern of growth to a rare tumor with features of carcinoma
ICD coding
Epidemiology
- 0.3% of odontogenic cysts (J Oral Pathol Med 2006;35:500)
- Mean age: 31 years (standard deviation: 21 years) range 5 - 92 years; however, this varies geographically (J Oral Pathol Med 2018;47:721)
- No consistent gender predominance
- Around 33% of cases are associated with odontogenic lesions, most commonly odontoma; odontoma associated COC occurs in younger patients on average (20.4 years) (J Oral Pathol Med 2018;47:721)
Sites
- Vast majority of lesions are central COC (within bone of jaw, intraosseous) (Reichart: Odontogenic Tumors and Allied Lesions, Illustrated Edition, 2004)
- Less commonly, peripheral lesions may be seen (located on gingival tissues, extraosseous) most of which can be classified as dentinogenic ghost cell tumors
- Usually anterior regions of jaws, incisor / cuspid region
- Lesions associated with odontoma are most commonly found in the anterior maxilla (J Oral Pathol Med 2008;37:302)
Pathophysiology
- Cystic neoplasms with β catenin (CTNNB1) mutations in the Wnt signaling pathway
- In one series, 91% (10/11) cases of CCOT / COC demonstrated CTNNB1 point mutations COC (PLoS One 2017;12:e0180224)
- Immunohistochemistry for LEF1 (a transcription factor of the Wnt pathway) is reported to be positive in 64% (7/11) of CCOT (Hum Pathol 2015;46:255)
Clinical features
- Either asymptomatic (incidental radiographic finding) or a painless swelling
- Extraosseous lesions present as a gingival swelling, which may be painful
- May be associated with other odontogenic pathology, most commonly odontoma (J Oral Pathol Med 2018;47:721)
Diagnosis
- Diagnosis can be made on an incisional biopsy or enucleation specimen
Radiology description
- Usually unilocular, well defined radiolucency with focal opacification but may rarely be multilocular (Br J Radiol 2012;85:548)
- Scattered radiopacities in 33 - 50%
- 33% associated with impacted tooth
- Usually 2 - 4 cm
- Adjacent tooth root displacement, resorption or root divergence may occur (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;101:356)
Radiology images
Contributed by Elizabeth Ann Bilodeau, D.M.D., M.D., M.S.Ed.
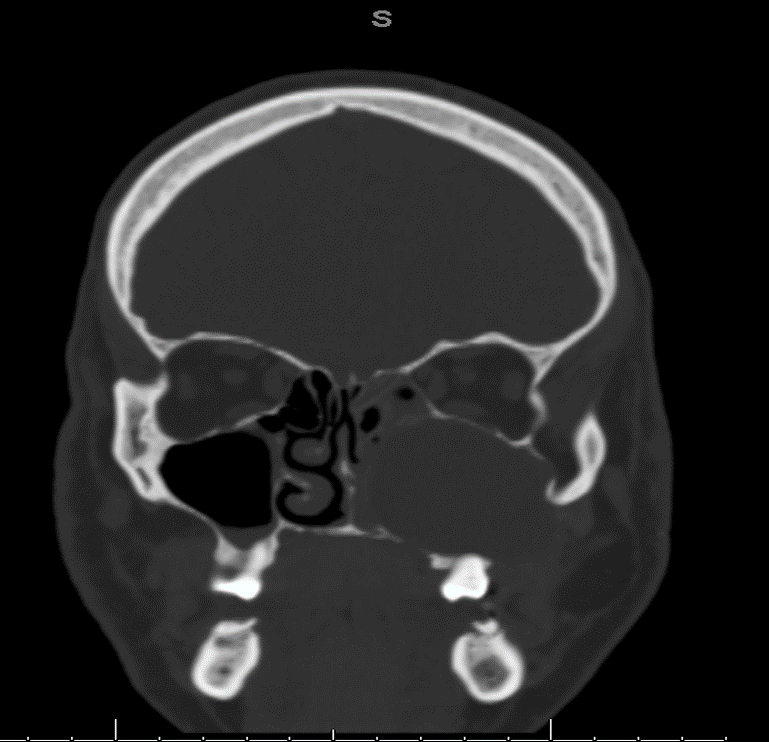
Coronal CT
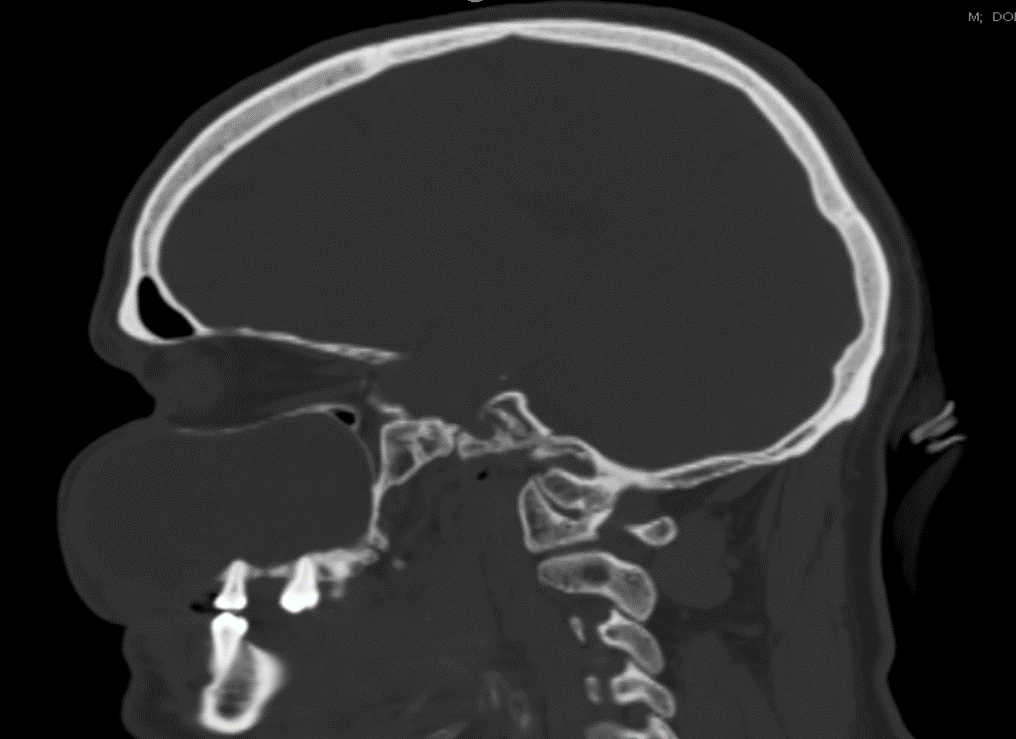
Sagittal CT
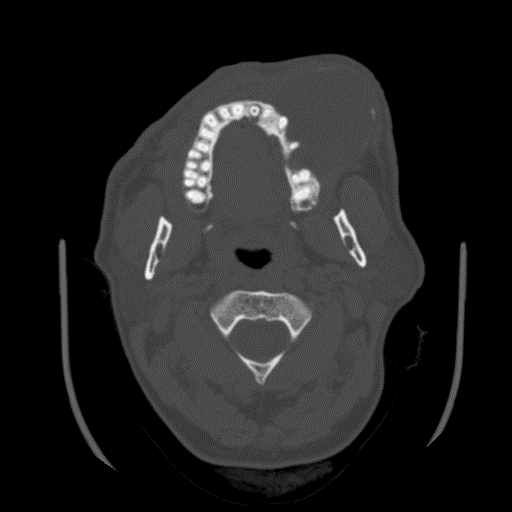
Axial CT
Prognostic factors
- Prognosis excellent, few recurrences (< 5% documented)
- Rarely, malignant transformation has been reported (Case Rep Pathol 2013;2013:853095, Korean J Pathol 2012;46:478, Ann Diagn Pathol 2009;13:394)
Case reports
- 15 year old Japanese boy with pigmented calcifying cystic odontogenic tumor associated with compound odontoma (Head Face Med 2007;3:35)
- 23 year old man with ameloblastic fibro-odontoma arising from a calcifying odontogenic cyst (Bull Tokyo Dent Coll 2001;42:51)
- 24 year old woman with calcifying odontogenic cyst associated with an orthokeratinized odontogenic cyst (Head Neck Pathol 2008;2:324)
- 36 year old man with a 5.9 cm calcifying odontogenic cyst treated with 2 stage decompression (J Oral Maxillofac Surg 2017;75:1915)
- Hybrid odontogenic tumor with features of ameloblastic fibro-odontoma, calcifying odontogenic cyst and adenomatoid odontogenic tumor (J Oral Maxillofac Surg 2010;68:470)
Treatment
- Treated by enucleation and curettage
- For combined lesions, treat according to characteristics of more aggressive lesion
- Large cysts may be decompressed prior to surgical management in a 2 stage approach (J Oral Maxillofac Surg 2017;75:1915)
Gross description
- Unicystic, often 2 cm or less; no solid areas
- Grossly cystic with focal luminal thickenings
Gross images
Contributed by Elizabeth Ann Bilodeau, D.M.D., M.D., M.S.Ed.

Opened and sectioned cyst
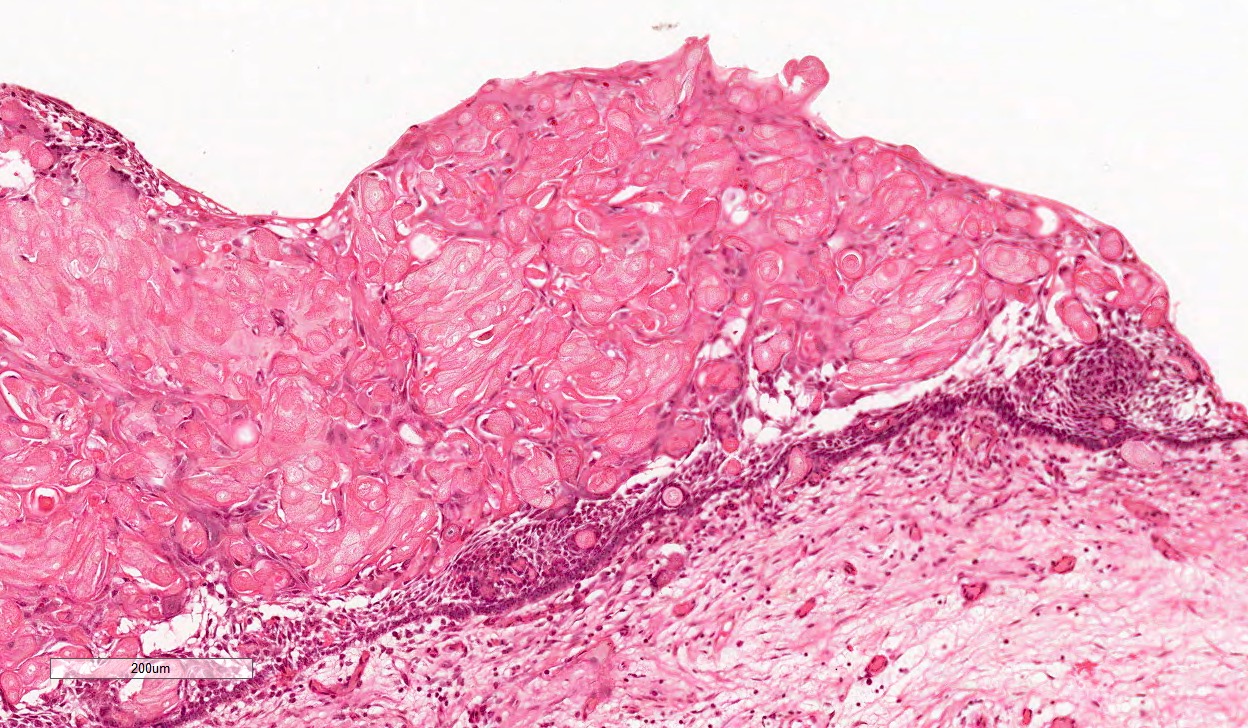
Microscopic (histologic) description
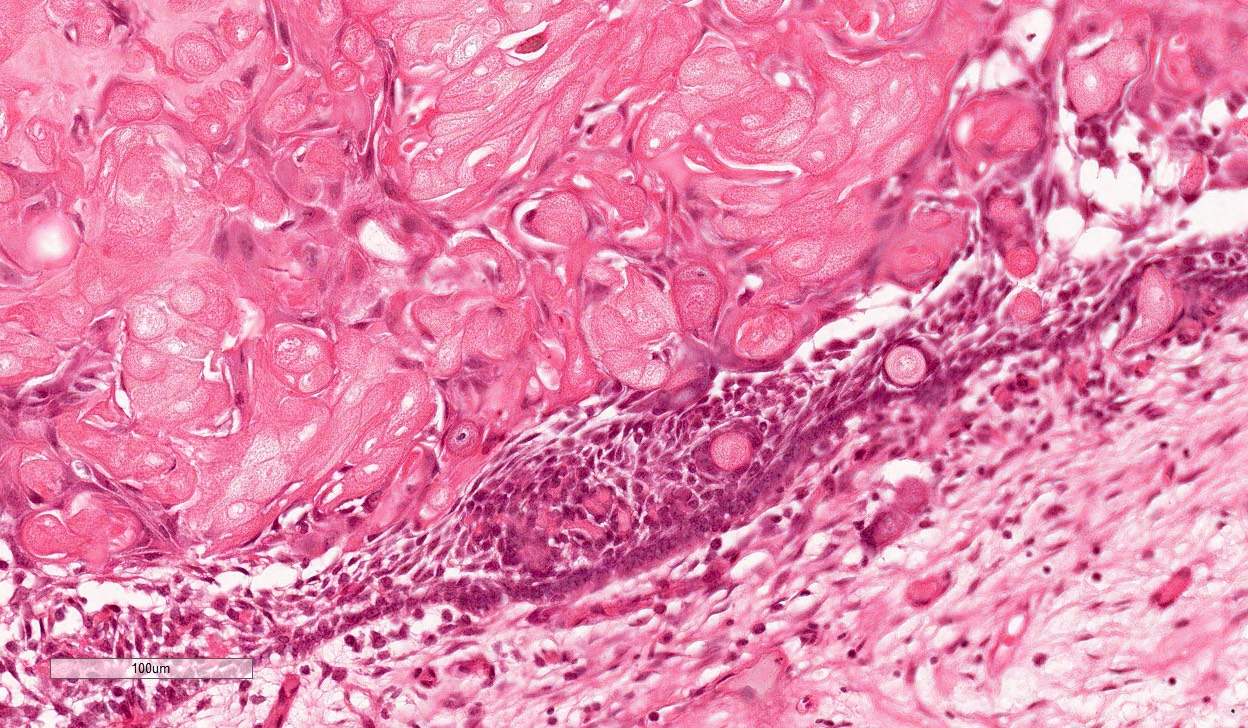
- Cyst lining is of odontogenic epithelium with a well defined layer of palisading basal cells, loosely arranged suprabasal epithelial cells resembling stellate reticulum, similar to ameloblastoma (microscopic image #1)
- Unlike ameloblastoma, variable numbers of cells undergo ghost cell change in suprabasilar epithelium (microscopic image #1)
- Pale, eosinophilic ghost cells are altered epithelial cells with preservation of basic cell outline and eosinophilic cytoplasm but loss of the nucleus; ghost cell change may be due to coagulative necrosis, accumulation of enamel protein, aberrant keratinization of odontogenic epithelium and these cells may calcify (microscopic images #2 - 3)
- Other variable findings may include:
- Foreign body giant cell reaction
- Proliferation of odontogenic epithelium into the cyst wall which can resemble strands of dental lamina (microscopic image #4)
- Dystrophic calcifications
- Dentinoid may be laid down next to basal cells:
- Paucicellular, eosinophilic calcified material considered to represent dysplastic dentin (microscopic image #4)
- May be present adjacent to epithelial component
- Most likely formed due to an inductive effect of odontogenic epithelium on adjacent mesenchymal tissue
- Cyst wall consists of mature fibrous connective tissue containing scattered inflammatory cells (unless secondarily infected)
- Reference: Reichart: Odontogenic Tumors and Allied Lesions, Illustrated Edition, 2004
Microscopic (histologic) images



Cytology description
- Numerous polyhedral epithelial cells and occasional columnar cells with calcification and Congo red negative extracellular homogenous material in background (Acta Cytol 2009;53:460)
Positive stains
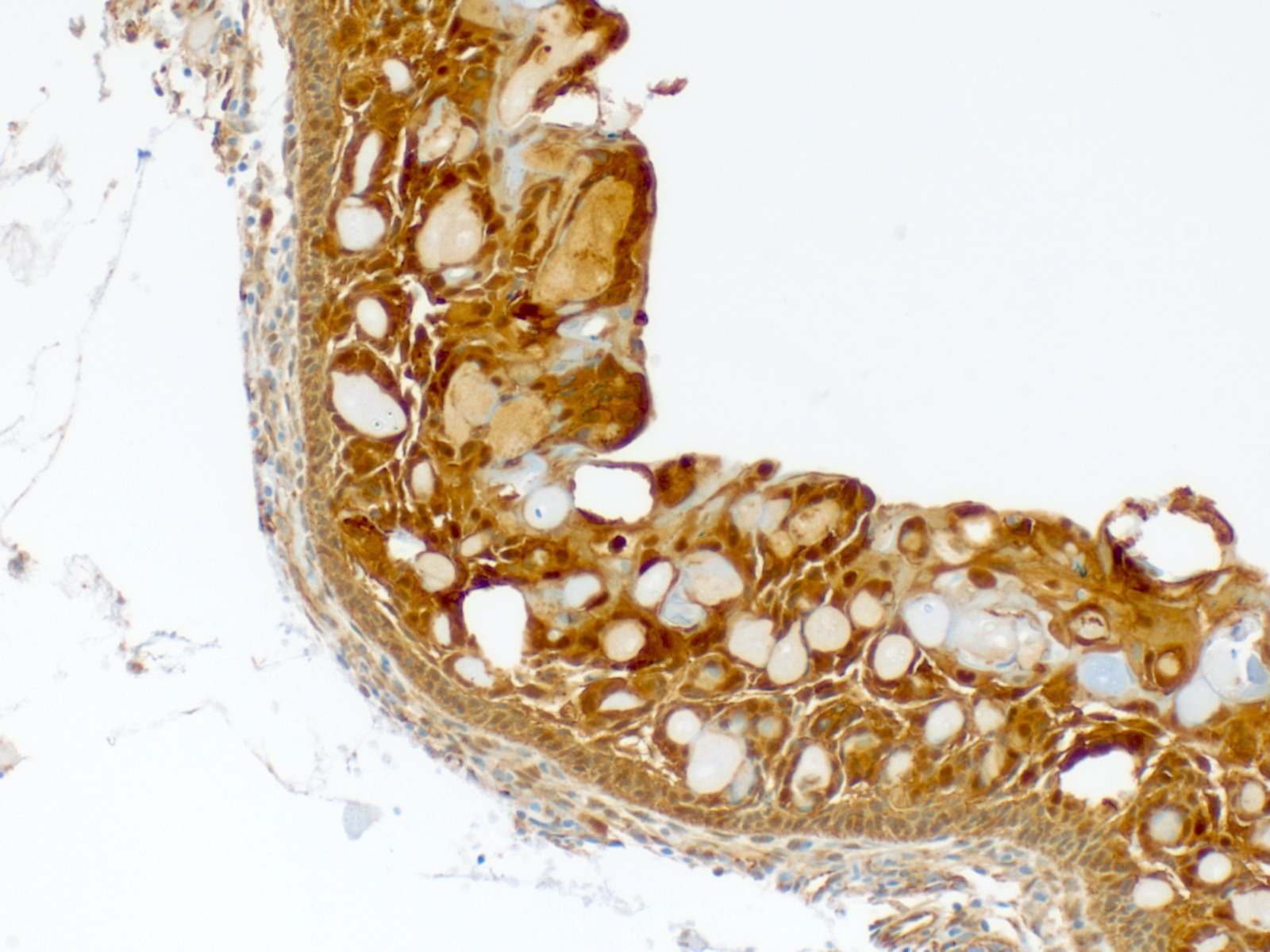
- β catenin (microscopic image #5) (Hum Pathol 2015;46:255, APMIS 2008;116:206, Pathol Int 2006;56:732, Am J Clin Pathol 2003;120:732, Am J Pathol 2003;163:1707)
- LEF1 (microscopic image #6) (Hum Pathol 2015;46:255)
- Cytokeratins 7, 8, 14 and 19 (J Oral Pathol Med 2003;32:163)
- Amelogenesis related proteins (J Oral Pathol Med 2012;41:272)
- MMPs (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011;112:609)
- Hard α keratins (Am J Clin Pathol 2005;123:376)
- Podoplanin (J Oral Sci 2012;54:165)
- Ki67 lower in COC than in other odontogenic tumors with ghost cells and solid growth pattern (Oral Oncol 2009;45:515)
Negative stains
- Nothing useful or significant
Electron microscopy description
- Basal and suprabasilar cells contain tonofilaments and organelles
- Ghost cells contain coarse bundles of tonofilaments intermingled with dilated membranous organelles (Med Electron Microsc 2002;35:109, Oral Surg Oral Med Oral Pathol 1975;39:769)
Molecular / cytogenetics description
- Aberrations of Wnt signaling pathway with β catenin overexpression (APMIS 2008;116:206)
- Mutations in CTNNB1 but not BRAF (PLoS One 2017;12:e0180224)
Sample pathology report
- Anterior maxilla, right, excisional biopsy:
- Calcifying odontogenic cyst (calcifying cystic odontogenic tumor) 1.2 cm
Differential diagnosis
- Ameloblastoma (conventional or unicystic):
- Usually lacks ghost cells and calcifications
- Dentinogenic ghost cell tumor / carcinoma
- Solid counterpart of COC
- Ghost cell odontogenic carcinoma:
- Infiltrative
- Exhibits mitotic activity, nuclear atypia or necrosis
- Odontoma:
- Lacks the ameloblastic epithelium of COC
- Ameloblastic fibro-odontoma:
- Exhibits primitive mesenchymal stroma
Additional references
Practice question #1
What is the most common mutation in calcifying odontogenic cyst?
- β catenin
- BRAF
- PPARγ
- PTCH
- RAS
Practice answer #1
Practice question #2
What odontogenic tumor most commonly is associated with a calcifying odontogenic cyst?
- Adamantinomatous craniopharyngioma
- Adenomatoid odontogenic tumor
- Ameloblastoma
- Basal cell adenocarcinoma
- Odontoma
Practice answer #2
Practice question #3
Which feature is most typical for a calcifying odontogenic cyst?
- Cyst lining contains a well defined layer of palisading basal cells and a stellate reticulum-like suprabasal layer
- Infiltrative lesion with mitotic activity
- No ameloblastic epithelium present
- Sellar or suprasellar location
Practice answer #3
A. Cyst lining contains a well defined layer of palisading basal cells and a stellate reticulum-like suprabasal layer
Comment Here
Reference: Calcifying odontogenic cyst
Comment Here
Reference: Calcifying odontogenic cyst
