Mandible & maxilla
Cysts of the jaw
Dentigerous cyst
Author: Kelly Magliocca, D.D.S., M.P.H.
Editorial Board Members: Ruta Gupta, M.D., Bin Xu, M.D., Ph.D.

Last author update: 9 August 2023
Last staff update: 27 March 2024
Copyright: 2004-2025, PathologyOutlines.com, Inc.
PubMed Search: Dentigerous cyst
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Frozen section description | Frozen section images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Positive stains | Negative stains | Sample pathology report | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Magliocca K. Dentigerous cyst. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/mandiblemaxilladentigerous.html. Accessed September 6th, 2025.
Definition / general
- Dentigerous cyst is a developmental odontogenic cyst that originates from the separation of the dental follicle from around the crown of an unerupted tooth, thus showing an epithelial lining attached to the cementoenamel junction
Essential features
- Intraosseous location, maxilla or mandible
- Cystic strips of nonneoplastic, nondysplastic epithelium with a fibrous or fibromyxoid cyst wall
- Epithelial lining is composed of stratified squamous epithelium
- Radiographic findings show cyst associated with crown of unerupted tooth
- Treatment is surgical, unlikely to recur once excised
- Diagnosis requires correlation with radiographs or knowledge of radiographic findings
Terminology
- Follicular cyst is synonymous
- Extraosseous counterpart: eruption cyst, involves an erupting tooth, usually a deciduous first molar tooth (Med Oral Patol Oral Cir Bucal 2017;22:e228)
- Ameloblasts: specialized epithelial cells that form tooth enamel
- Reduced enamel epithelium
- Enamel is normally composed of 2 cell layers: inner layer of reduced or atrophied ameloblasts and external layer, probably stratum intermedium cells
- Reduced enamel epithelium is normally found overlying an unerupted, otherwise developed tooth
- Deciduous tooth (also called baby tooth or primary tooth): exfoliated during childhood
- Succedaneous tooth (also called adult tooth): permanent tooth; replaces deciduous teeth
ICD coding
- ICD-11: DA05.0 - developmental odontogenic cysts
Epidemiology
- Second most common odontogenic cyst (Braz Oral Res 2021;35:e129)
- Most common developmental odontogenic cyst (Braz Oral Res 2021;35:e129)
- Multiple simultaneous dentigerous cysts are uncommon
- Broad age range (5 - 83 years), with peak incidence in second to third decade and a slight male predilection (J Oral Pathol Med 2013;42:462, Surg Pathol Clin 2017;10:177, J Oral Pathol Med 2019;48:74, Oral Maxillofac Surg 2020;24:73)
Sites
- By definition, a dentigerous cyst occurs in association with an unerupted tooth
- Most common around permanent mandibular third molars (wisdom teeth)
- Somewhat less common around permanent maxillary third molars, maxillary cuspids and mandibular second premolars but any tooth may be involved (J Oral Pathol Med 2013;42:462)
- Rarely involves supernumerary teeth and odontomas
- Distinctly rare to occur around unerupted primary teeth
Pathophysiology
- Vast majority are developmental odontogenic cysts with unknown pathogenesis; subset may have inflammatory pathogenesis
- Inflammation progressing from root apex of carious or necrotic deciduous tooth brings about development of dentigerous cyst around underlying, unerupted permanent tooth (J Korean Assoc Oral Maxillofac Surg 2022;48:342, Exp Ther Med 2021;22:750)
- Difficult to histologically distinguish inflamed developmental odontogenic dentigerous cyst from those induced by inflammation
Etiology
- In normal tooth development, tooth enamel is produced by the enamel organ, an ectodermally derived specialized epithelium
- After enamel formation is complete, the enamel organ epithelium atrophies
- This reduced enamel epithelium eventually merges with the overlying mucosal epithelium to form the initial gingival crevicular epithelium of the newly erupted tooth
- Develops from accumulation of fluid (including glycosaminoglycans) between reduced enamel epithelium of dental follicle and crown of unerupted tooth (Mod Pathol 2017;30:S96, Surg Pathol Clin 2017;10:177, J Oral Pathol Med 2019;48:74)
Clinical features
- May be small / asymptomatic; then may be incidentally detected on radiographs taken for unrelated reasons or for imaging to investigate delayed tooth eruption (Oral Maxillofac Surg 2020;24:73)
- Large lesions may produce a painless bony expansion; can displace the involved tooth or cause resorption of adjacent teeth
- If secondarily infected, may be associated with pain
Diagnosis
- Diagnosis incorporates elements such as clinical examination, patient history, symptoms, clinical examination, imaging and supportive histopathology
- Patient symptoms (see Clinical features)
- Clinical examination findings: dentigerous cyst is not clinically visible on examination of oral cavity
- Surgical findings during operative exploration
- Cyst fluid may be released during extirpation
- Cyst cavity may be appreciated during extirpation
- Lesion classically surrounds crown of unerupted tooth
- Lesion is intraosseous and will require surgical exposure through mucosa and bone
- Imaging findings of lesion relative to unerupted tooth (Diagnostics (Basel) 2022;12:2006)
- Histopathology additionally supports the diagnosis
Radiology description
- Radiology is essential to identify landmarks and the extent of disease in the preoperative and follow up setting
- Panoramic radiograph (panorex), intraoral film or cross sectional imaging can detect most cases of dentigerous cyst
- Most commonly a well defined, unilocular radiolucency on Xray
- Often has sclerotic border
- Can cause resorption of adjacent teeth
- 3 different radiographic relationships between unerupted tooth and cyst are described (Imaging Sci Dent 2021;51:291)
- Central
- Most common radiographic relationship
- Cyst develops around and surrounds the entire crown of tooth; thus, the tooth appears to be erupting into the cyst (see Clinical images)
- Lateral
- Cyst develops at lateral tooth root and only partially surrounds the crown (see Clinical images)
- Circumferential
- Cyst develops around the crown and extends down the root(s); thus, roots also appear within the cyst
- Central
- Radiographic differential diagnosis of dentigerous cyst: odontogenic keratocyst, orthokeratinized odontogenic cyst and ameloblastoma among other odontogenic tumors
- Detection of bilateral dentigerous cysts is uncommon
- Radiographic distinction between an enlarged dental follicle and a small dentigerous cyst can be arbitrary
- Generally, a pericoronal radiolucency that is > 3 - 4 mm in diameter is considered suggestive of cyst formation
Radiology images
Contributed by Kelly Magliocca, D.D.S., M.P.H.
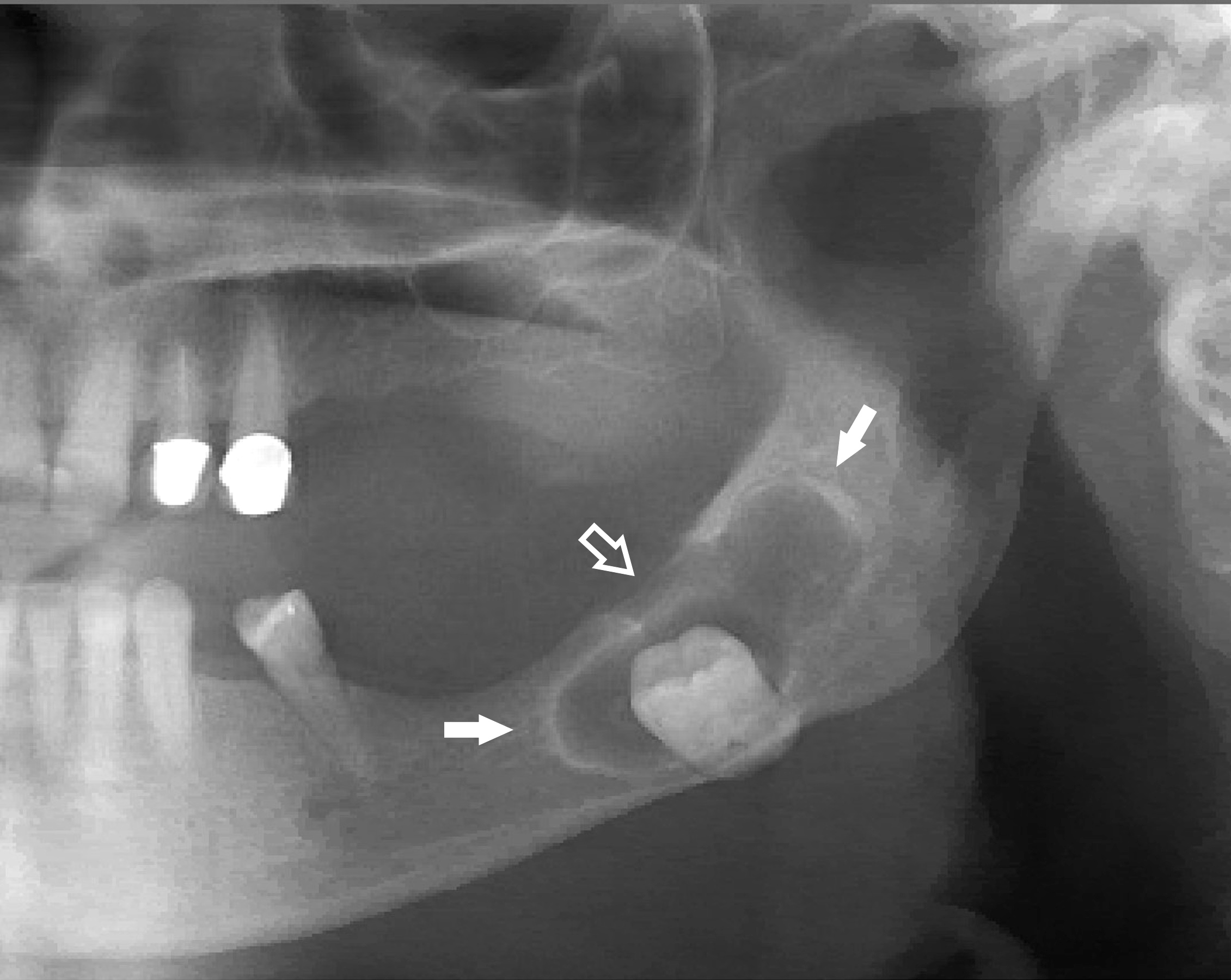
Cropped panorex
Images hosted on other servers:

Central variety

Lateral variety

Multiple radiopaque masses with thin radiolucent rim

Expansion and thinning of the bony sinus wall
Prognostic factors
- Excellent prognosis
- Almost never recurs with complete enucleation
- Recurrence may indicate incomplete excision or possibly incorrect original diagnosis (Head Neck Pathol 2021;15:107)
Case reports
- 12 year old boy with bilateral inflammatory dentigerous cysts (Int J Clin Pediatr Dent 2020;13:429)
- 20 year old woman with florid cemento-osseous dysplasia in association with dentigerous cyst (J Oral Maxillofac Pathol 2010;14:63)
- 44 year old man with bilateral dentigerous cysts (Am J Case Rep 2019;20:1148)
- 65 year old woman with dentigerous cyst in association with odontoma (Case Rep Dent 2022;2022:6210289)
Treatment
- Varies based on age, maturity, anatomic position and relative importance of tooth involved, size of cyst, presence of additional neoplasms; also patient preference, including cosmetic and functional considerations
- Enucleation of entire cyst with extraction of the associated tooth is the most common approach
- Marsupialization
- Removal of the cyst sparing the permanent tooth (J Appl Oral Sci 2012;20:282)
- Requires close follow up to monitor for recurrence
Clinical images




Gross description
- Relationship of tooth and cyst is usually disrupted during surgery; however, examination of associated tooth may reveal tags of adherent tissue at cementoenamel junction (Surg Pathol Clin 2017;10:177)
- Surgical specimens usually consist of multiple, irregular fragments
- Possible minute bone fragments
- All mucosal, soft tissue and bone fragments should be submitted for histologic examination to definitively confirm the diagnosis
- Tooth received as specimen can be photographed and grossly described unless cyst develops in association with odontoma
- Odontoma requires microscopic examination, further underscoring the importance of radiographic correlation
Gross images
Images hosted on other servers:

Hard and soft tissues with impacted lateral incisor

Enucleated specimen with embedded canine

Cystic lesion

Tan colored thickenings in wall of cystic lesion

Maxillary right quadrant


Mandibular left quadrant

Extracted tooth and pathologic lining
Frozen section description
- Variability depending on the degree and extent of inflammation
- Inflamed cysts may show multilayered stratified squamous epithelium making it difficult to distinguish from unicystic ameloblastoma, luminal subtype or inflamed odontogenic keratocyst
- Uninflamed cysts may show low cuboidal or bilaminar epithelial lining
- Frozen section limitations include sampling bias, frozen section artifact and inability to perform immunohistochemistry, such as BRAF (J Oral Maxillofac Surg 2014;72:914)
Frozen section images
Contributed by Kelly Magliocca, D.D.S., M.P.H.

Cystic strips of inflamed tissue

Cyst epithelium

Squamous epithelium
Microscopic (histologic) description
- Microscopic features are influenced by presence of inflammation
- Inflamed dentigerous cyst
- Fibrous connective tissue
- Hyperplastic nonkeratinized epithelium, sometimes elongated interconnecting rete ridges
- Acute and chronic inflammatory cells
- Cholesterol clefts, possibly formation of cholesterol granuloma
- Rushton bodies
- Scattered mucous, ciliated or sebaceous cells are uncommon but possible (J Oral Sci 2005;47:77)
- Occasional dystrophic calcifications
- Odontogenic epithelial rests, small, inactive appearing within fibrous wall
- Noninflamed dentigerous cyst (J Oral Pathol Med 2013;42:462)
- Fibrous to fibromyxoid connective tissue
- No rete ridges, flat interface
- Lining epithelium, 2 - 4 layers of cuboidal epithelium, devoid of superficial keratinization
- Occasional mucous cells; rare ciliated cells
- Occasional dystrophic calcifications
- Odontogenic epithelial rests, small, inactive appearing within fibrous wall
- Some lesions submitted as dentigerous cysts are partially lined with a thin, fragmented layer of eosinophilic columnar cells / low cuboidal epithelium representing the postfunctional ameloblastic layer of the reduced enamel epithelium
- Classification of these lesions as cysts versus dental follicles shows interobserver variability
Microscopic (histologic) images
Contributed by Kelly Magliocca, D.D.S., M.P.H.

Cyst and cholesterol granuloma

Stratified squamous epithelium
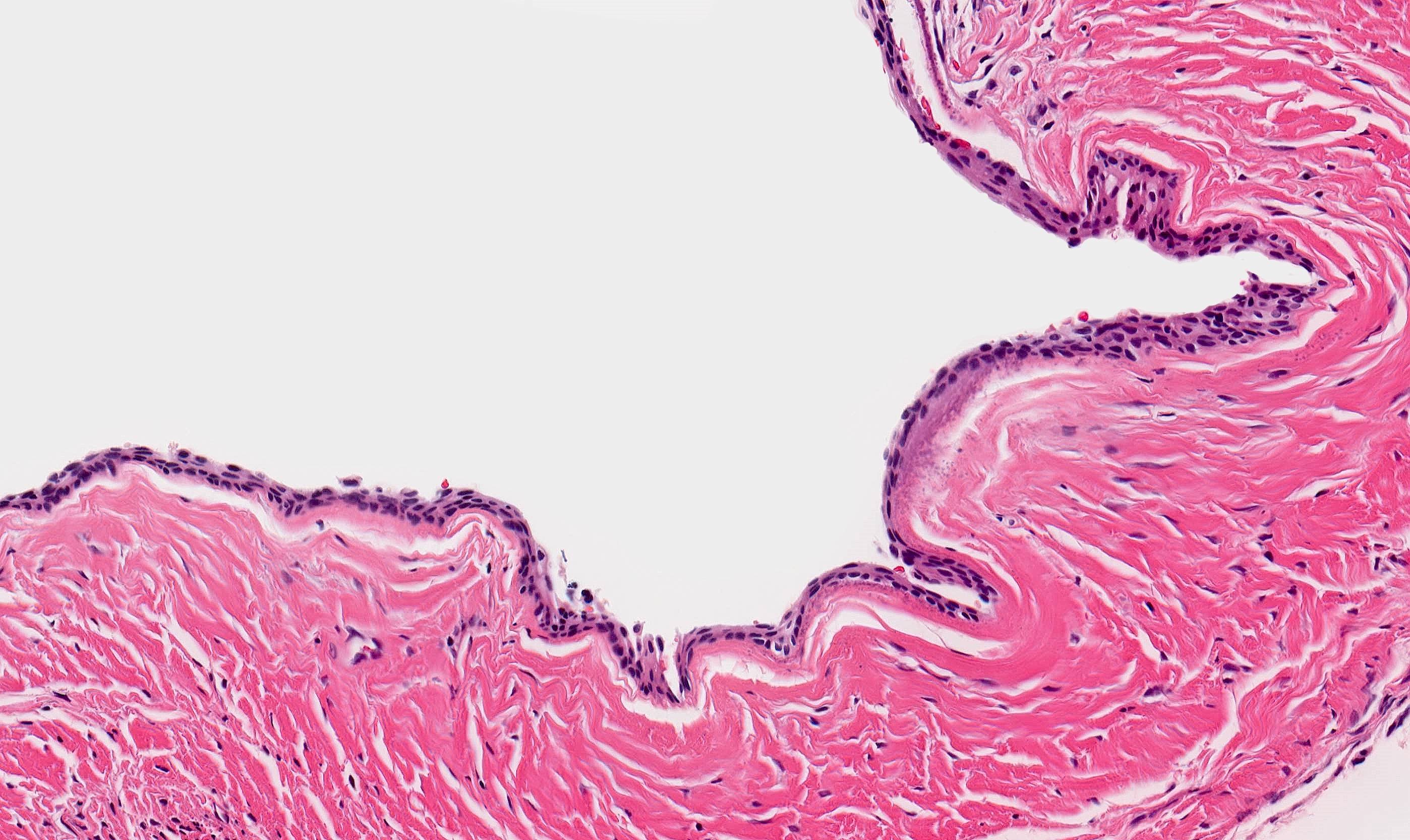
Cyst epithelium
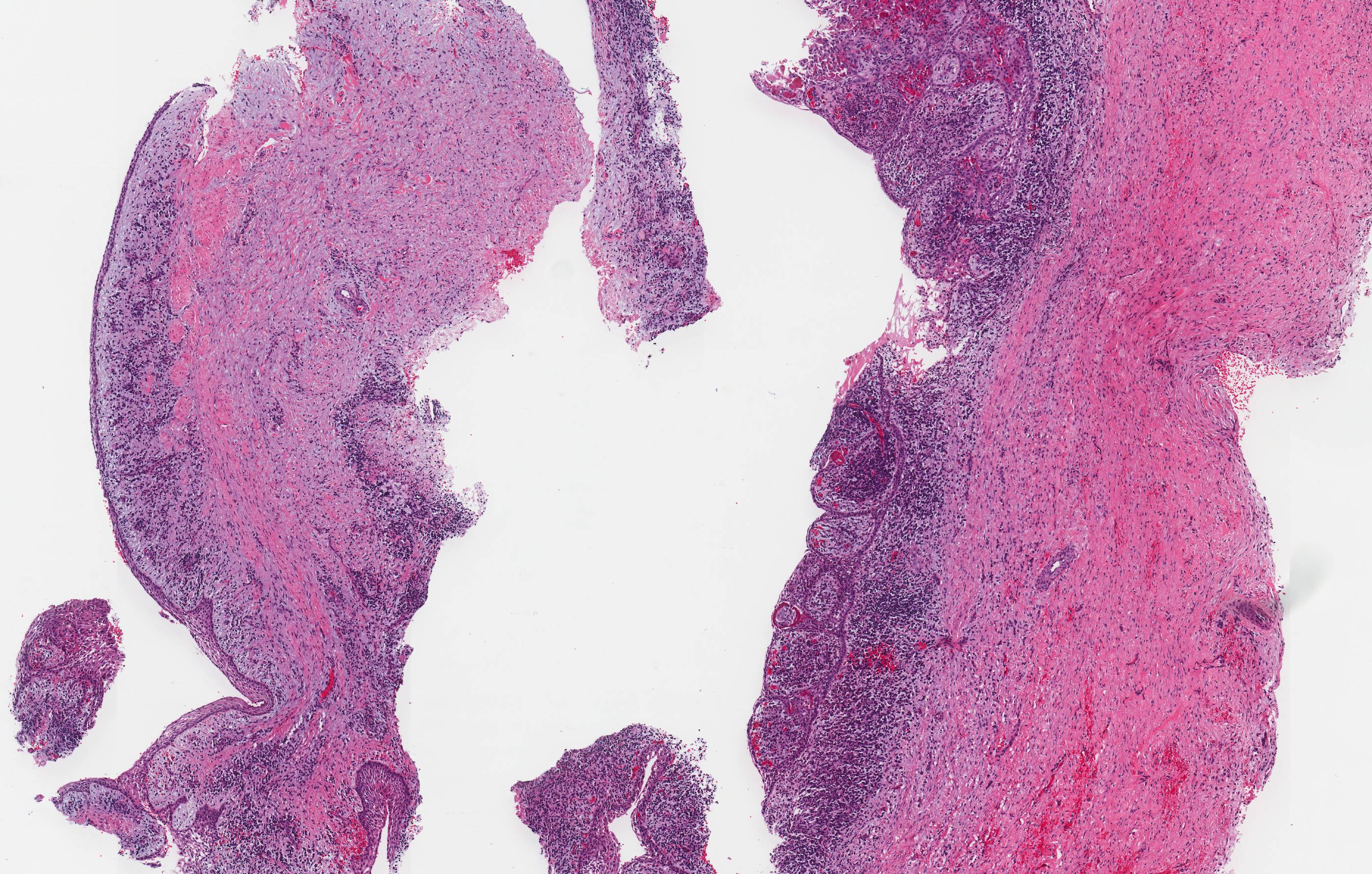
Inflamed cyst

Variable cyst epithelial lining

Subepithelial mineralization
Virtual slides
Images hosted on other servers:

Dentigerous cyst
Positive stains
- No specific immunohistochemistry required for dentigerous cyst
- Squamous epithelium expected to be immunoreactive for cytokeratin AE1 / AE3, p63 and p40
Negative stains
- BRAF immunostain
- Beta catenin immunostain negative for nuclear staining
Sample pathology report
- Left mandible lesion, excision:
- Stratified squamous epithelial lined cyst consistent with dentigerous cyst
Differential diagnosis
- Unicystic ameloblastoma:
- Columnar basal cells with hyperchromatic nuclei
- Usually but not always exhibit reverse polarization of nuclei (away from basement membrane)
- Dentigerous cysts do not harbor the BRAF p.V600E mutations found in ameloblastomas (J Oral Pathol Med 2016;45:780, Appl Immunohistochem Mol Morphol 2021;29:390)
- Odontogenic keratocyst:
- Uniform epithelium
- 4 - 8 cell layers in thickness
- Hyperchromatic basilar palisading of cuboidal to columnar cells
- Characteristic wavy / corrugated surface parakeratosis
- With or without keratin flakes within cyst lumen
- Radicular / periapical cyst:
- Radicular cyst (RC) is an inflammatory odontogenic cyst associated with the root of a nonvital tooth
- Surfaced by nonkeratinized stratified squamous epithelium
- Often characterized by an arcading pattern
- Cyst wall is composed of inflamed fibrous tissue; may have foamy histiocytes
- Inflammatory collateral cysts:
- Inflammatory cysts occur on the buccal or distobuccal aspect of the roots of partially or recently erupted teeth
- Microscopically can be almost indistinguishable from inflamed radicular cyst or inflamed dentigerous cyst
- Further divided into 2 subtypes
- Mandibular buccal bifurcation cyst occurs on the lateral aspect of partially or recently erupted tooth
- Paradental cyst occurs on the distobuccal aspect of partially or recently erupted tooth
Additional references
Practice question #1
Which of the following entities represents a microscopic mimic of inflamed dentigerous cyst?
- Ameloblastic fibroma
- Mandibular buccal bifurcation cyst
- Odontogenic myxoma
- Orthokeratinized odontogenic cyst
Practice answer #1
B. Mandibular buccal bifurcation cyst. Mandibular buccal bifurcation cysts are lined by an inflamed, nonkeratinizing stratified squamous epithelial lining, similar to an inflamed dentigerous cyst. Buccal bifurcation cysts occur lateral to an erupting or recently erupted mandibular tooth whereas dentigerous cyst occurs in relation to an impacted tooth.
Answer A is incorrect because ameloblastic fibroma is an odontogenic neoplasm composed of epithelial and mesenchymal components. It is not cystic. Answer C is incorrect because odontogenic myxoma is a mesenchymal neoplasm without cystic change. Answer D is incorrect because the epithelial lining of orthokeratinized odontogenic cyst is heavily keratinized.
Comment Here
Reference: Dentigerous cyst
Answer A is incorrect because ameloblastic fibroma is an odontogenic neoplasm composed of epithelial and mesenchymal components. It is not cystic. Answer C is incorrect because odontogenic myxoma is a mesenchymal neoplasm without cystic change. Answer D is incorrect because the epithelial lining of orthokeratinized odontogenic cyst is heavily keratinized.
Comment Here
Reference: Dentigerous cyst
Practice question #2
What is the most common locational relationship for a dentigerous cyst to have with a tooth?
- Surrounds the apex of erupted tooth
- Surrounds the crown of erupted tooth
- Surrounds the crown of unerupted tooth
- Surrounds the lateral aspect of erupted tooth
Practice answer #2
C. Surrounds the crown of unerupted tooth. Dentigerous cysts most commonly surround the crown of an unerupted tooth. While the circumferential and lateral radiographic appearance have been described, the classically described dentigerous cyst shows the crown of the tooth projecting into the cyst.
Answer A is incorrect because a dentigerous cyst surrounding only the apex of an unerupted tooth has not been described. Answer B is incorrect because a dentigerous cyst involves an unerupted tooth, not an erupted tooth. Answer D is incorrect because a dentigerous cyst involves an unerupted tooth, not an erupted tooth.
Comment Here
Reference: Dentigerous cyst
Answer A is incorrect because a dentigerous cyst surrounding only the apex of an unerupted tooth has not been described. Answer B is incorrect because a dentigerous cyst involves an unerupted tooth, not an erupted tooth. Answer D is incorrect because a dentigerous cyst involves an unerupted tooth, not an erupted tooth.
Comment Here
Reference: Dentigerous cyst
