
Molecular markers
Tumor mutation burden
Author: Megan Parilla, M.D.
Editorial Board Member: Ruta Gupta, M.D.
Deputy Editor-in-Chief: Patricia Tsang, M.D., M.B.A.

Last author update: 31 May 2022
Last staff update: 31 May 2022
Copyright: 2022, PathologyOutlines.com, Inc.
PubMed Search: Tumor mutation burden

Table of Contents
Definition / general | Essential features | Terminology | Pathophysiology | Diagrams / tables | Clinical features | Uses by pathologists | Prognostic factors | Molecular / cytogenetics description | Sample pathology report | Additional references | Board review style question #1 | Board review style answer #1Cite this page: Parilla M. Tumor mutation burden. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/moleculartumormutation.html. Accessed April 19th, 2024.
Definition / general
- An accounting of the number of somatic mutations seen in a particular tumor's genome
- Number of mutations found in the genome of a tumor correlates with tumor type, mechanism of genomic damage and the likelihood for the immune system to recognize the tumor tissue as abnormal
- One of the predictive biomarkers that indicates the likelihood of response to immune checkpoint inhibition therapies, such as PDL1 blockade
Essential features
- Tumor mutation burden (TMB) is one of the biomarkers that suggests whether immune checkpoint inhibition therapy will be efficacious
- Whole genome or exome sequencing is the gold standard for determining tumor mutation burden but larger targeted panel gene sequencing can provide a good estimation of TMB
- Tumor mutation burden varies by tumor type; for example, cutaneous melanomas have more mutations (on average) than prostate adenocarcinoma
Terminology
- Tumor mutation burden (TMB)
- Tumors that are genetically tested and found to have a large number of mutations are called high TMB or TMB H tumors
Pathophysiology
- TMB varies between tumor types (see Diagrams / tables) and often correlates with exposure to environmental mutagens or defective intracellular DNA repair (Nature 2013;500:415)
- Tumors with inherited or acquired defects in DNA mismatch repair result an inability to replicated microsatellites with fidelity (termed microsatellite instability / MSI H) and correspondingly demonstrate high TMB and a hyper mutated phenotype (Nature 2012;487:330)
- Mutation in the proofreading domain of the gene encoding DNA polymerase Epsilon, POLE, results in extremely high numbers of single nucleotide missense mutations and an ultra mutated phenotype (Curr Opin Genet Dev 2014;24:107, Nature 2012;487:330)
- TMB H tumors, with more mutations in genes, have more abnormal protein production
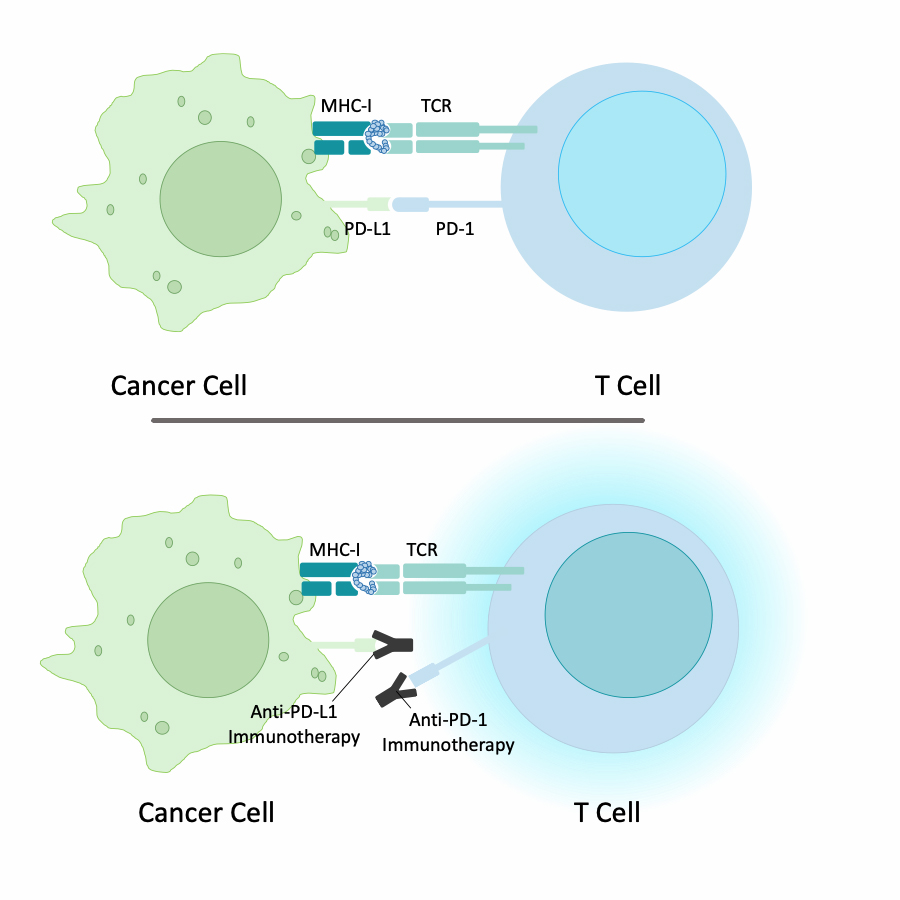
- Portions of abnormal proteins are presented by major histocompatibility complex (MHC) class I molecules as foreign cancer antigens to T cells for destruction
- PDL1 is a protein that is expressed on normal, healthy tissues to aid in T cell recognition of self when MHC class I molecules display self peptides
- When MHC I molecules display foreign peptides, the self destruction signals from abnormal peptides should supersede the self preservation signals from PDL1
- One way cancer cells can evade cytotoxic T cell destruction is by increasing the expression of PDL1 to supersede the self destruction signals from MHC I neoantigens
- Immune therapies that target PDL1 interacting with PD-1 on T cells work best in cancers that have a high TMB; this is because TMB H tumors have more MHC I neoantigen presentation to T cells
- Reference: Nat Rev Cancer 2017;17:209
Diagrams / tables

Clinical features
- 1 Mb is equivalent to 1 million nucleotides
- Universal TMB cutoffs for all tumor types may not be as effective as tumor specific TMB thresholds, which have yet to be determined (Clin Cancer Res 2021;27:1236)
- Prevalence of TMB H is variable; UV induced melanomas have many more mutations per megabase (Mb) when compared to breast and thyroid carcinoma (Science 2015;349:1483)
- TMB H is common with > 30% prevalence in non small cell and small cell lung cancer and in UV induced cutaneous melanoma (JAMA Netw Open 2020;3:e2025109)
- TMB H is infrequent with < 5% prevalence in biliary adenocarcinoma, prostate adenocarcinoma, sarcomas, thyroid carcinoma and mesothelioma (JAMA Netw Open 2020;3:e2025109)
Uses by pathologists
- FDA has approved pembrolizumab (a PD-1 inhibitor) for solid tumors that are unresectable or metastatic and are categorized as TMB H
- Identification of POLE mutations and an ultra mutated phenotype in uterine endometrial adenocarcinoma is associated with a good prognosis (Obstet Gynecol Clin North Am 2012;39:255)
- There is conflicting data about the utility of TMB across multiple tumor types, especially those not sampled in the KEYNOTE-158 study (Clin Cancer Res 2021;27:1236, Lancet Oncol 2020;21:1353)
Prognostic factors
- TMB has a mixed impact on prognosis when separated from immunotherapy response (Ann Transl Med 2020;8:575)
- Immune therapies work best in cancers that have a high TMB (Nat Rev Cancer 2017;17:209)
Molecular / cytogenetics description
- TMB was initially described in whole exome sequencing (WES), a form of next generation sequencing (NGS), which is the gold standard
- Smaller, targeted NGS panels are accurate in estimating TMB if they are larger than ~1.5 Mb (Int J Cancer 2019;144:848)
- Compared to WES, targeted gene panels have the advantage of faster turnaround times, lower costs and broader availability
Sample pathology report
- Endometrium, biopsy:
- Endometrial adenocarcinoma, endometrioid type (see molecular report)
- Molecular report:
- Tumor mutational burden: 125 muts/Mb
- TMB status: TMB H (≥ 10 muts/Mb)
Additional references
Board review style question #1

A patient with abnormal uterine bleeding has an endometrial biopsy sent for next generation sequencing. The next generation sequencing report is shown above. Which of the following is true about this patient's tumor?
- High TMB (125 muts/Mb) portends a favorable prognosis
- High TMB (125 muts/Mb) suggests the patient may have Lynch syndrome
- Low TMB (125 muts/Mb) portends a favorable prognosis
- Low TMB (125 muts/Mb) portends an unfavorable prognosis
Board review style answer #1
A. High TMB (125 muts/Mb) portends a favorable prognosis. The tumor has 125 mutations/Mb, which is greater than 10 mutations/Mb, qualifying this tumor as TMB H. TMB H tumors are more likely to respond to pembrolizumab (a PD-1 inhibitor) due to neoantigen presentation to the immune system. Additionally, ultra mutated endometrial adenocarcinoma (> 100 mutations/Mb) with pathogenic POLE mutations, seen in this report, have an excellent prognosis regardless of immunotherapy. Although microsatellite instable tumors may have high TMB, this tumor is microsatellite stable, so the likelihood of Lynch syndrome is low.
Comment Here
Reference: Tumor mutation burden
Comment Here
Reference: Tumor mutation burden

