
Oral cavity & oropharynx
Potentially malignant & dysplasia
Actinic cheilitis
Editorial Board Member: Molly Housley Smith, D.M.D.
Deputy Editor-in-Chief: Kelly Magliocca, D.D.S., M.P.H.


Last author update: 12 April 2024
Last staff update: 12 April 2024
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Actinic cheilitis
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Goldfaden JS, Bilodeau EA. Actinic cheilitis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/oralcavityactiniccheilitis.html. Accessed April 23rd, 2024.
Definition / general
- Common premalignant alteration, usually of the lower lip vermilion, that results from chronic ultraviolet light exposure
Essential features
- Clinically, this manifests as blurring of the demarcation between the vermilion and lip mucosa (Head Neck Pathol 2020;14:899)
- Actinic cheilitis has a strong predilection for fair skinned (> 87%) men (> 70%) over the age of 55; colloquially known as farmer's lip or sailor's lip due to its association with such outdoor occupations (Head Neck Pathol 2020;14:899, AOCD: Actinic Cheilitis [Accessed 4 March 2024])
- Surface epithelium is variably dysplastic and is low risk for malignant transformation (J Investig Clin Dent 2018;9:e12343, StatPearls: Actinic Cheilitis [Accessed 4 April 2024], J Dent Res Dent Clin Dent Prospects 2021;15:285)
- Hyperkeratosis, acanthosis and atrophy of the epithelium may also be present
- Underlying connective tissue exhibits solar elastosis, which appears as a band of amorphous, acellular, basophilic change due to ultraviolet light induced degeneration of collagen and elastin fibers (Head Neck Pathol 2021;15:566)
Terminology
- First described as "scurfy, scaly lip of the outdoor worker" by Montgomery and Culver in 1920, who attributed this to effects of wind and weather; Ayres coined the term chronic actinic cheilitis in 1923 to describe a chronic inflammatory disorder of the lips as a result of actinic or chemically active rays of sunlight (JAMA 1923;81:1183)
- In 1997, Manganaro, Will and Poulos designated actinic cheilitis as a premalignant, irreversible pathosis that most often affects the lower lip vermilion (Gen Dent 1997;45:492)
ICD coding
Epidemiology
- Actinic cheilitis has a strong predilection for fair skinned (> 87%) men (> 70%) over the age of 55 (Head Neck Pathol 2020;14:899)
Sites
- Actinic cheilitis affects the vermilion of the lower lips in 95% of cases (Head Neck Pathol 2020;14:899)
Pathophysiology
- Ultraviolet B (UVB) rays (290 - 320 nm) are the primary cause of actinic damage as 70% is absorbed by the skin (J Oral Med Oral Surg 2023;29:30)
- This form of radiation drives thymine and uracil dimer formation in DNA and RNA, respectively; additionally, UVB rays create 6 - 4 pyrimidine photoproducts and substitutions of cytosine thymine in DNA, which particularly results in mutations to the p53 protein (Photochem Photobiol 2008;84:422)
Etiology
- Ultraviolet radiation from long term sun exposure
Clinical features
- Actinic cheilitis manifests as a blurred demarcation between the vermilion and the mucosal lip, erythema and edema with subsequent dry scaling / a persistent, nonmigrating crust and in some cases, leukoplakia (BDJ Open 2017;3:17016, J Drugs Dermatol 2011;10:1240)
- Patients typically have a chief concern of persistent chapped lips or lip tightness (AOCD: Actinic Cheilitis [Accessed 4 March 2024])
Diagnosis
- May be detected clinically as blurring between the vermilion and lip mucosa as an incidental finding
- Lip may also be erythematous, swollen or present with white patching
- Biopsy is indicated
Prognostic factors
- Chronic sun exposure without protective measures increases risk for malignant transformation
- Weighted remission rate following surgical treatment (92.8%) is greater than nonsurgical treatment (65.9%)
- Additionally, the recurrence following surgery (8.4%) is lower in comparison to nonsurgical treatment (19.2%) (Oral Dis 2019;25:972)
Case reports
- 51 year old man with a chief concern of a lip lesion that was diagnosed by his dentist (Oral Surg Oral Med Oral Pathol Oral Radiol 2020;130:e203)
- 64 year old, fair skinned man with multiple crusted areas of the lower lip vermilion (Oral Surg Oral Med Oral Pathol Oral Radiol 1980;50:21)
- 67 year old woman with a 2 year history of dryness, thickening and scaling of the entire lower lip that was treated with photodynamic therapy (Phtodermatol Photoimmunol Photomed 2007;23:209)
- 76 year old man presented with a white, hyperkeratotic lesion of the lower lip (Dermatology 2016;232:1)
Treatment
- Surgical treatments, particularly carbon dioxide laser ablation and vermilionectomy, are associated with the most favorable outcomes and the fewest recurrences (J Eur Acad Dermatol Venereol 2021;35:815)
- Nonsurgical treatments for actinic cheilitis consist of a variety of topical therapies, including
- 5-fluorouracil
- Imiquimod
- Trichloroacetic acid
- Ingenol mebutate
- Diclofenac
- Reference: Photodermatol Photoimmunol Photomed 2019;35:11
Clinical images
Contributed by James Guggenheimer, D.D.S.

Blurring of lip vermilion
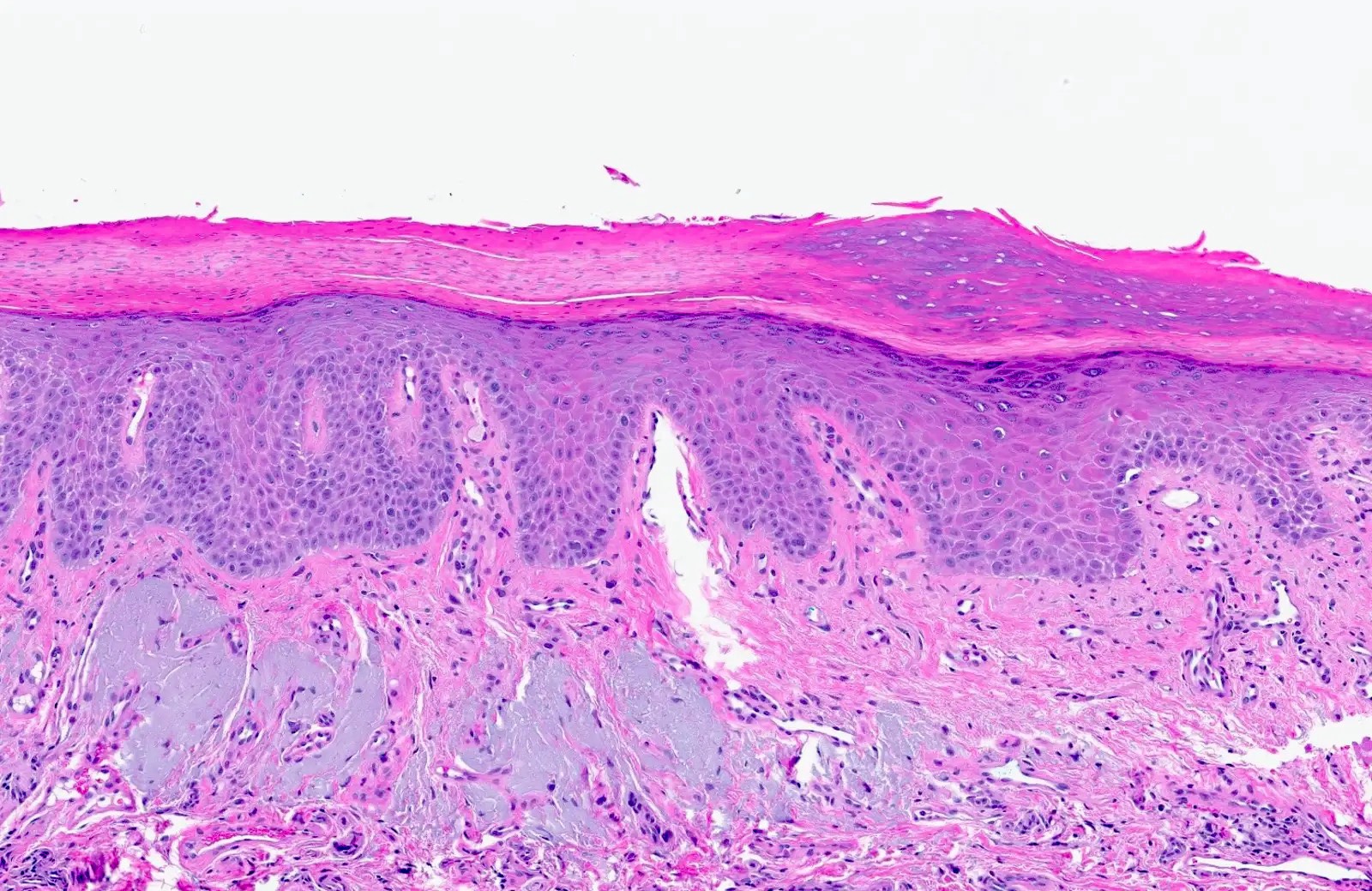
Microscopic (histologic) description
- Surface epithelium is variably dysplastic
- Hyperkeratosis, acanthosis and epithelial atrophy may be noted
- Underlying connective tissue exhibits solar elastosis, which appears as a band of amorphous, acellular, basophilic change due to ultraviolet light induced degeneration of collagen and elastin fibers (Head Neck Pathol 2021;15:566)
- Chronic inflammatory cell infiltrate and dilated blood vessels are often present
Microscopic (histologic) images
Contributed by Joshua Seth Goldfaden, D.D.S.
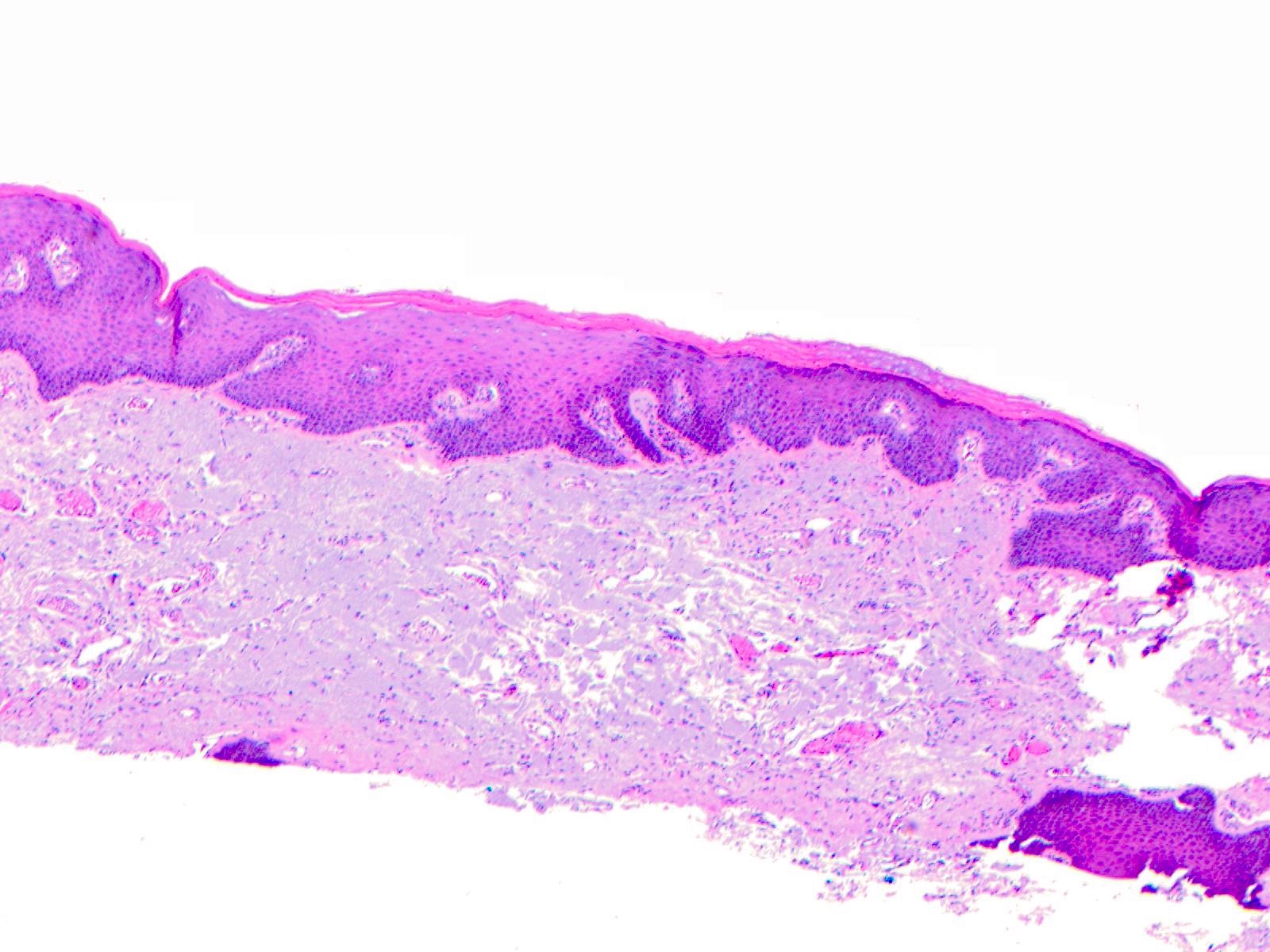
Hyperkeratotic, dysplastic epithelium
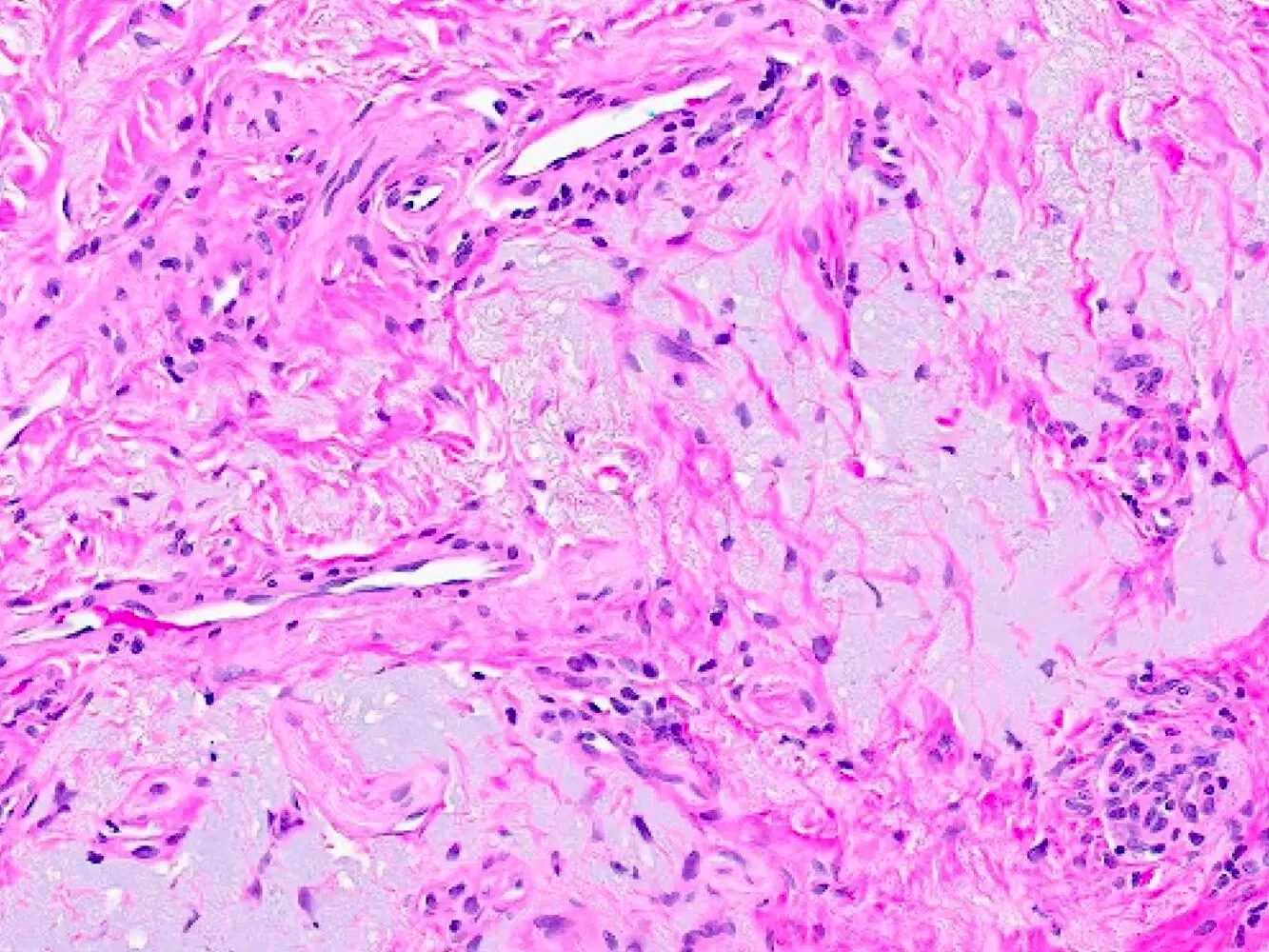
Prominent solar elastosis and telangiectasia
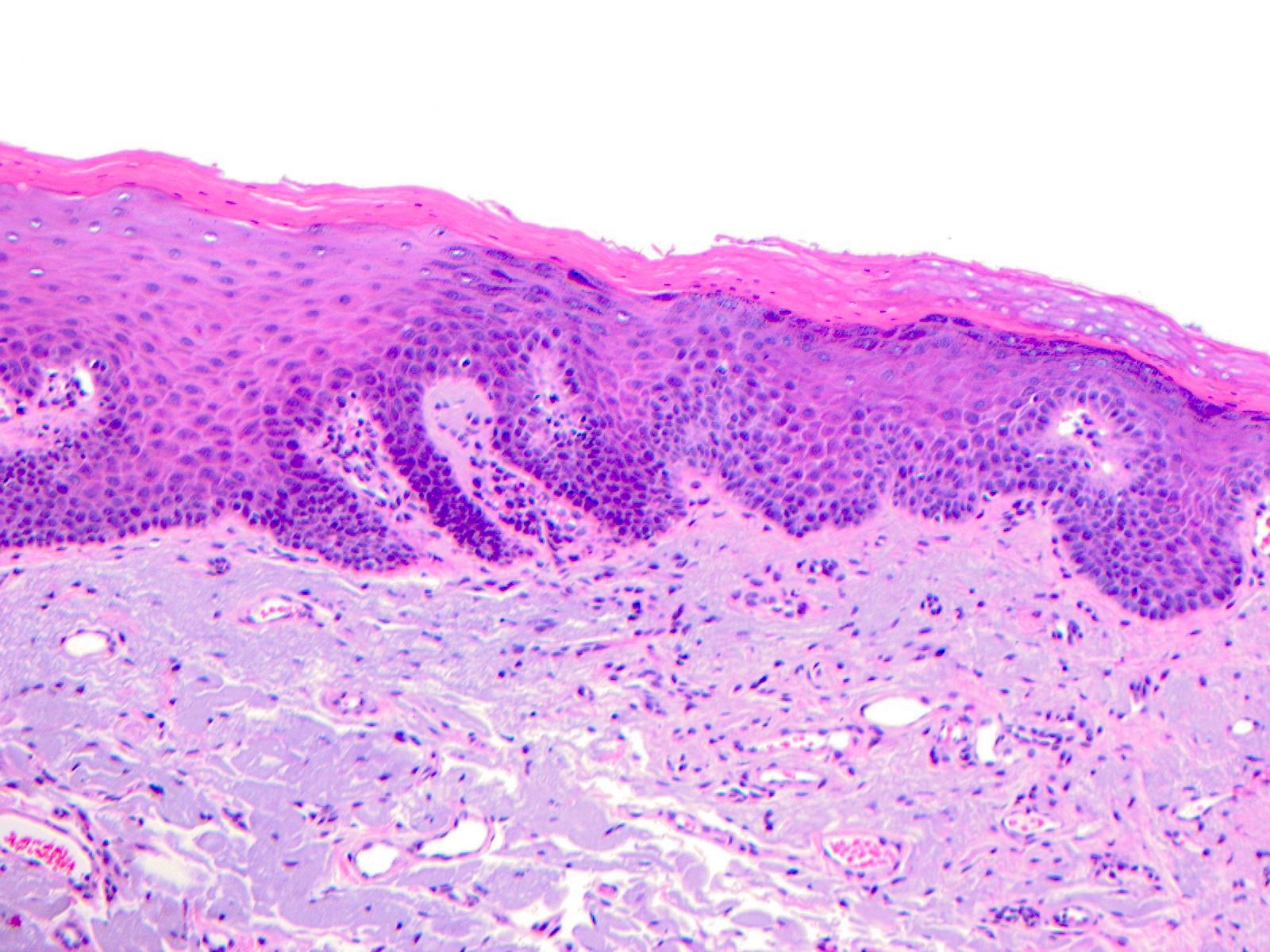
Epithelium with dysplastic changes
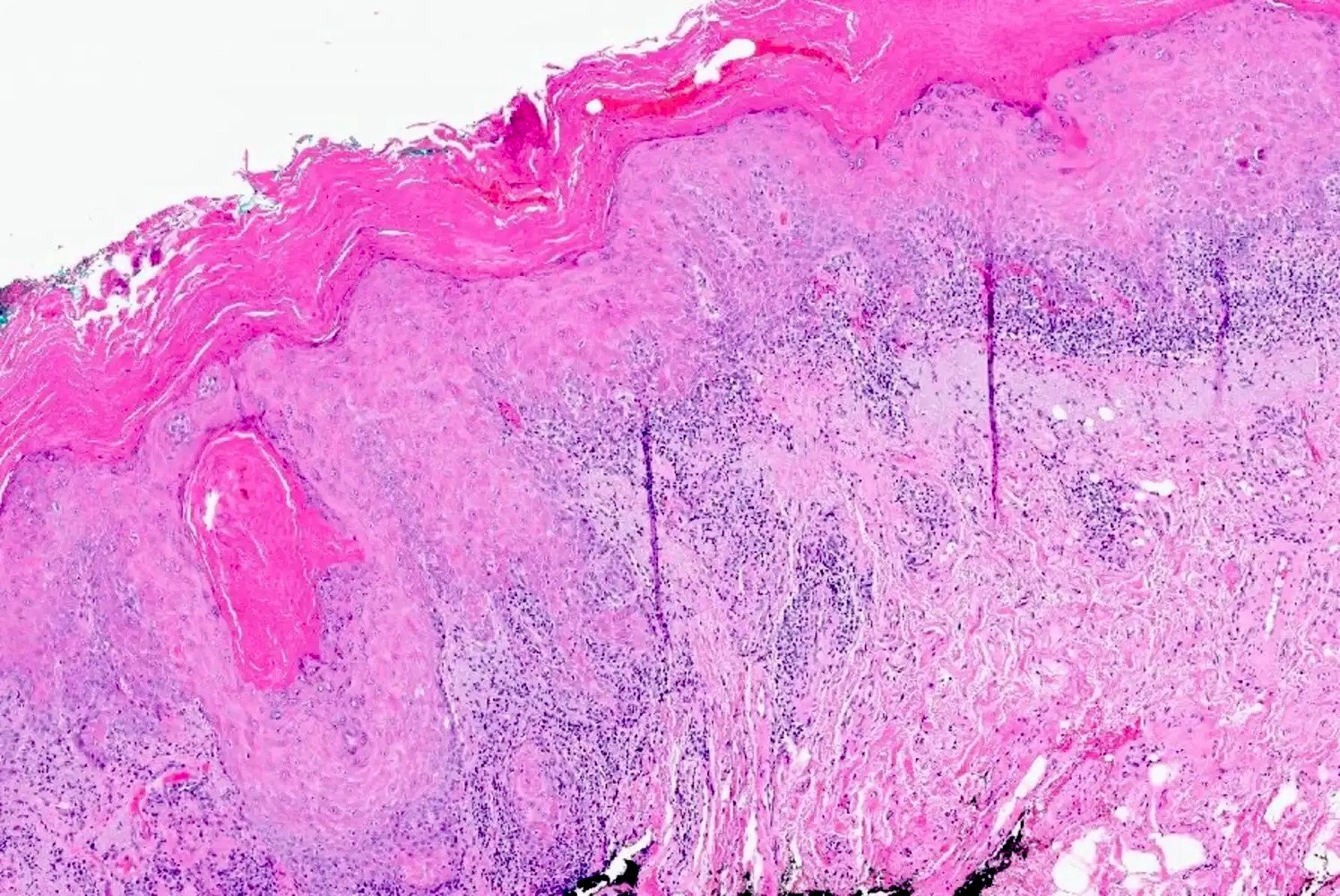
Arising squamous cell carcinoma
Keratosis and solar elastosis
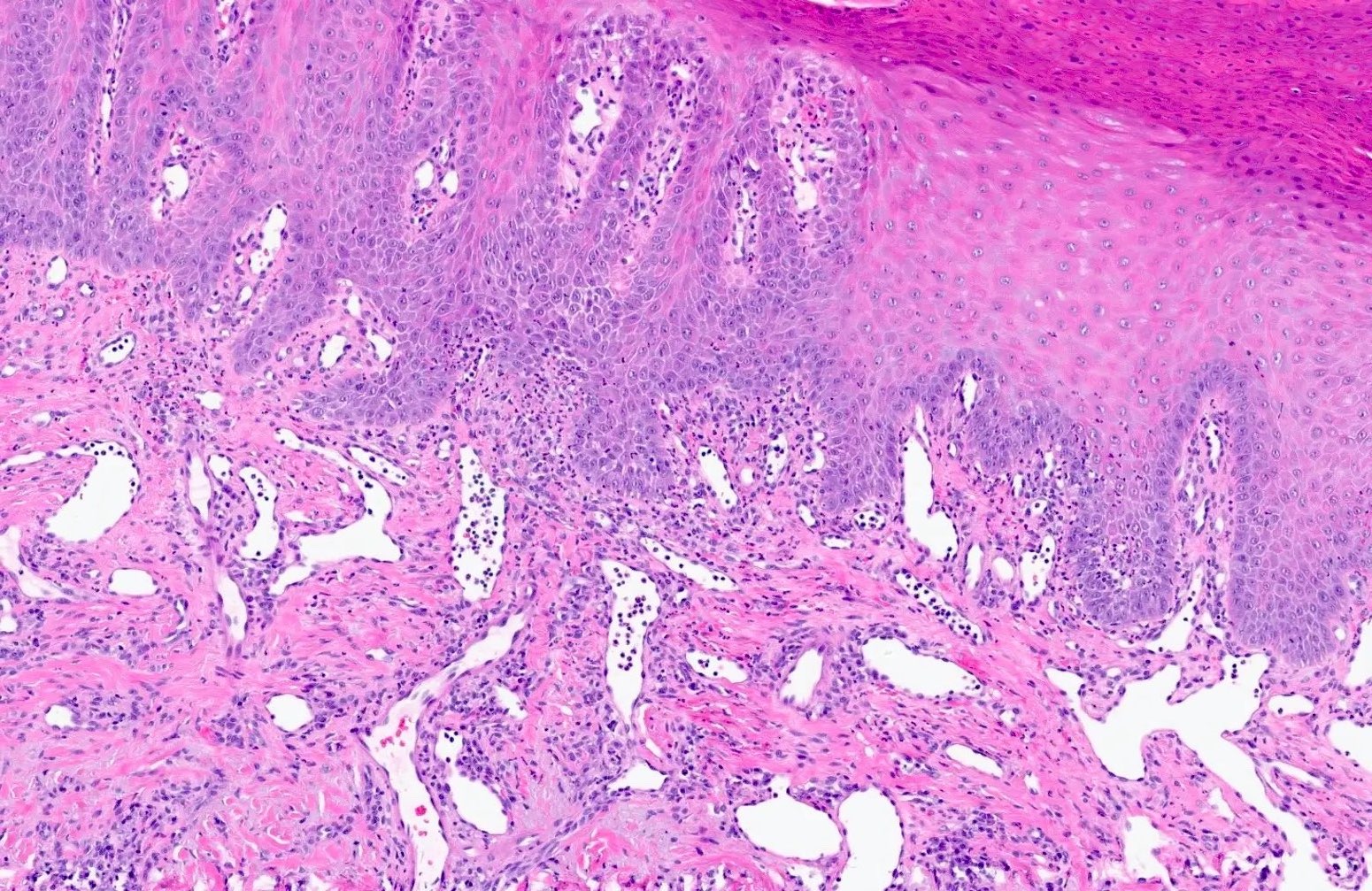
Epithelial dysplasia and dilated vessels
Positive stains
- p53 is variable; may have extreme (loss or gain) staining of surface epithelium or may be nonextreme (nonmutated)
- MDM2 coexpression may also be increased (Oral Oncol 2008;44:878)
- Ki67 and IMP3 may exhibit respective increased proliferation and expression within surface epithelium (Oral Maxillofac Surg 2022;26:587)
Negative stains
- SOX10, MelanA / MART1, MITF and HMB45
Sample pathology report
- Left lower lip, incisional biopsy:
- Actinic cheilitis (see comment)
- Comment: Actinic cheilitis is considered a premalignant condition. Long term monitoring is advised. Further, the patient should be cautioned against future unprotected sun exposure and smoking (if applicable) (Oral Surg Oral Med Oral Pathol Oral Radol and Endodontol 1999;88:181).
Differential diagnosis
- Squamous cell carcinoma:
- Invasive tumor islands are seen within the connective tissue
- Abnormal mitotic figures and keratin pearl formation may be seen
- Cheilitis glandularis:
- Inflammatory condition of the minor salivary glands and excretory duct dilation, particularly of the lower lip
- Nodular enlargement, reduced mobility and eversion of the affected lip(s) (J Am Dent Assoc 1989;118:317)
- Basal cell carcinoma:
- Nests of basaloid cells with peripheral palisading associated with a fibromyxoid stroma
- Basaloid cells have a high N:C ratio with hyperchromatic nuclei
- Nests of basaloid cells with peripheral palisading associated with a fibromyxoid stroma
- Herpes labialis:
- Intraepidermal blisters with acantholytic epithelium and solitary keratinocytes within the blister pouch
- Nuclei of the keratinocytes show nuclear changes, including margination of chromatin, multinucleation and nuclear inclusions
- Nuclear viral inclusions are small, pink deposits with a clear halo
- Initial clinical lesions appear as blisters that rupture and ulcerate
- The condition is self limiting and recurrences may occur
- Intraepidermal blisters with acantholytic epithelium and solitary keratinocytes within the blister pouch
Board review style question #1
A biopsy of the lower lip of a 65 year old man reveals high grade dysplastic change, solar elastosis and telangiectasia. Based on these findings, what is the most appropriate diagnosis?
- Actinic cheilitis
- Cheilitis glandularis
- Keratoacanthoma
- Squamous cell carcinoma
Board review style answer #1
A. Actinic cheilitis. High grade dysplasia in the context of solar elastosis and telangiectasias is consistent with actinic cheilitis. Answer B is incorrect because cheilitis glandularis appears as inflammation of the salivary glands and dilation of the excretory ducts. Answer C is incorrect because keratoacanthomas are nodular with a central keratin plug. Answer D is incorrect because squamous cell carcinomas appear as nests of atypical epithelial cells within the stroma that arise from the surface.
Comment Here
Reference: Actinic cheilitis
Comment Here
Reference: Actinic cheilitis
Board review style question #2
A 60 year old, fair skinned woman presents with blurring of the vermilion and mucosa of the lower lip with an associated white plaque with prominent, surrounding erythema. Based on the clinical image, what is the lesion?
- Actinic cheilitis
- Basal cell carcinoma
- Cheilitis glandularis
- Melanoma
Board review style answer #2
A. Actinic cheilitis. This clinical image depicts blurring of the lower lip vermilion that is consistent with chronic solar damage. Answer B is incorrect because basal cell carcinoma often appears as ulcerated, nodular lesions with associated telangiectasias. Answer C is incorrect because cheilitis glandularis presents as nodular enlargement and eversion of the affected lip(s). Answer D is incorrect because melanoma (cutaneous) often exhibits irregular, pigmented areas.
Comment Here
Reference: Actinic cheilitis
Comment Here
Reference: Actinic cheilitis
