

Pleura & peritoneum
Peritoneum
Mesothelioma (peritoneum)-overview
Author: Yin P. (Rex) Hung, M.D., Ph.D.
Editor-in-Chief: Debra L. Zynger, M.D.

Last author update: 15 March 2022
Last staff update: 31 January 2023
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: peritoneal mesothelioma [title] pathology review [ptyp]


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Hung Y. Mesothelioma (peritoneum)-overview. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/pleuraperitmesotheliomageneral.html. Accessed April 18th, 2024.
Definition / general
- Tumor that originates from the serosal lining of the peritoneal cavity
Essential features
- Peritoneal mesothelioma shows weaker association with asbestos exposure and more likely involves women / young patients than pleural mesothelioma
- Histologic variants (epithelioid, biphasic and sarcomatoid) impart prognostic information with treatment implications
- Loss of BAP1 expression is seen in 40 - 60% of peritoneal mesothelioma, not sensitive but fairly specific for the diagnosis of mesothelioma in the appropriate histologic context
Terminology
- Peritoneal mesothelioma
- Malignant peritoneal mesothelioma
- Diffuse malignant peritoneal mesothelioma
- Abdominal mesothelioma
ICD coding
Epidemiology
- Accounts for ~10% of all mesotheliomas
- Incidence: ~300 new cases annually in the United States
- Presents with a wide age range and no apparent sex predilection (Cancer Causes Control 2009;20:935, Bull World Health Organ 2011;89:716, Clin Epidemiol 2016;8:743)
Sites
- Involves the serosal lining in the peritoneal cavity, often of multiple intra-abdominal organs
- Generally diffuse, rarely solitary / localized (Am J Surg Pathol 2005;29:866)
Etiology
- Associated with exposure to asbestos fibers in a subset of patients, typically with a long latency (median ~32 years); the association is weaker than in pleural mesothelioma (J Clin Oncol 1983;1:386, J Occup Med 1992;34:718, Arch Pathol Lab Med 2018;142:753)
- Rarely associated with exposure to non asbestos mineral fibers: erionite, fluoro-edenite and others (Arch Pathol Lab Med 2018;142:753)
- Rarely associated with prior exposure to therapeutic radiation for other malignancy with a latency of years to decades (J Clin Oncol 1983;1:695, Cancer 1988;61:2019, Arch Pathol Lab Med 2018;142:753)
- Rarely associated with recurrent peritonitis / chronic serosal inflammation secondary to Crohn disease, endometriosis or Familial Mediterranean Fever (J Clin Pathol 2017;70:228, J Clin Pathol 2018;71:971, Arch Pathol Lab Med 2018;142:753)
- Rarely associated with germline mutations and characteristic gene rearrangements (see molecular/cytogenetics section below)
Clinical features
- More likely to affect women and young patients as compared to pleural mesothelioma (Cancer Causes Control 2009;20:935)
- Symptoms can be nonspecific and depend on the extent of involvement
- Presentation includes most commonly abdominal pain, distension or ascites; rarely incidental or with new hernia, bowel obstruction or perforation (Tumori 2003;89:269, Ann Gastroenterol 2018;31:659)
- Morbidity / mortality primarily due to locoregional spread with extra-abdominal metastasis rare
- Median overall survival of 3 - 7 years with a 5 year survival rate of 40 - 60% with treatment (Ann Gastroenterol 2018;31:659)
Diagnosis
- Radiologic assessment of disease extent by computed tomography (CT) or magnetic resonance imaging (MRI)
- Cytologic analysis of peritoneal fluid, though this is not entirely sensitive
- Definitive diagnosis is most commonly based on histologic analysis of surgical specimen from laparoscopic / open or core needle biopsy
- Peritoneal mesothelioma, particularly the sarcomatoid variant, is difficult to diagnose and requires multiple immunohistochemical markers to exclude mimics
- Since no single immunohistochemical marker is entirely sensitive and specific for the diagnosis, a panel of at least 2 positive markers and 2 negative markers is recommended (Hum Pathol 2017;67:160)
Radiology description
- Multiple nodular lesions involving omentum and the mesentery, peritoneal thickening and accumulation of ascites (Anticancer Res 2016;36:1067)
Radiology images
Images hosted on other servers:

Omental caking
Prognostic factors
- Improved survival has been associated with the following:
- Age < 60 years (J Clin Oncol 2003;21:4560, Ann Surg Oncol 2018;25:2159, Ann Surg Oncol 2018;25:2018)
- Female gender (Ann Surg Oncol 2018;25:2159, Ann Surg Oncol 2018;25:2018)
- Epithelioid variant (J Clin Oncol 2009;27:6237, Pathology 2014;46:604, Ann Surg Oncol 2018;25:2018)
- Complete cytoreduction (J Clin Oncol 2003;21:4560, J Clin Oncol 2009;27:6237, Ann Surg Oncol 2015;22:1686, J Gastrointest Oncol 2017;8:915)
- Lack of lymph node metastasis (J Clin Oncol 2009;27:6237, J Gastrointest Oncol 2017;8:915)
- Low peritoneal cancer index (PCI) (Cancer 2011;117:1855, J Gastrointest Oncol 2017;8:915)
- Absence of loss of chromosomal region 9p21 / CDKN2A (Mod Pathol 2010;23:531, JAMA Oncol 2018;4:235)
- Worse survival has been noted to be associated with the following, although more data is needed for definitive conclusion:
- BAP1 molecular or expression status (J Thorac Oncol 2017;12:724)
- Elevated mitotic count (Clin Cancer Res 2005;11:3303, Histopathology 2016;68:729)
- High nuclear grade (Am J Surg Pathol 2016;40:1243)
- Solid pattern in epithelioid variant (Histopathology 2016;68:729)
Case reports
- 19 year old woman with abdominal pain and cachexia (epithelioid) (Cold Spring Harb Mol Case Stud 2019;5:a003566)
- 35 year old woman with omentum caking (epithelioid, deciduoid) (BMC Clin Pathol 2017;17:13)
- 40 year old woman with abdominal pain and distension (epithelioid) (Gastroenterology Res 2019;12:48)
- 61 year old woman with abdominal distension and ascites (epithelioid, clear cell pattern) (Pathol Res Pract 2017;213:580)
- 63 year old woman with abdominal pain (epithelioid, clear cell pattern with VHL mutation) (Hum Pathol 2019;83:199)
- 81 year old man with refractory ascites (biphasic) (Intern Med 2017;56:861)
Treatment
- Cytoreductive surgery, often combined with hyperthermic intraoperative chemotherapy, generally recommended for treating epithelioid variant (and some biphasic) but not sarcomatoid variant (Ann Surg Oncol 2015;22:1686, Ann Surg Oncol 2018;25:667)
- Chemotherapy types: hyperthermic intraoperative chemotherapy (HIPEC), early postoperative intraperitoneal chemotherapy (EPIC), long term intraperitoneal (IP) chemotherapy and systemic chemotherapy (Eur J Cancer 2016;65:69, Eur J Surg Oncol 2017;43:1228)
- Radiation
- Immunotherapy: clinical trial on using tremelimumab (anti-CTLA4 monoclonal antibody) and durvalumab (PD-L1 blockade) ongoing (Lancet Respir Med 2018;6:451)
Gross description
- Multiple omental / serosal nodules and thickened peritoneum
Gross images
Images hosted on other servers:

Adhesion of abdominal organs
Microscopic (histologic) description
- Unequivocal indicator of malignancy: invasion into adipose tissue or stromal invasion (Am J Surg Pathol 2000;24:1183, Arch Pathol Lab Med 2018;142:89)
- Histologically classified into epithelioid, biphasic and sarcomatoid variants with implications on prognosis and treatment planning
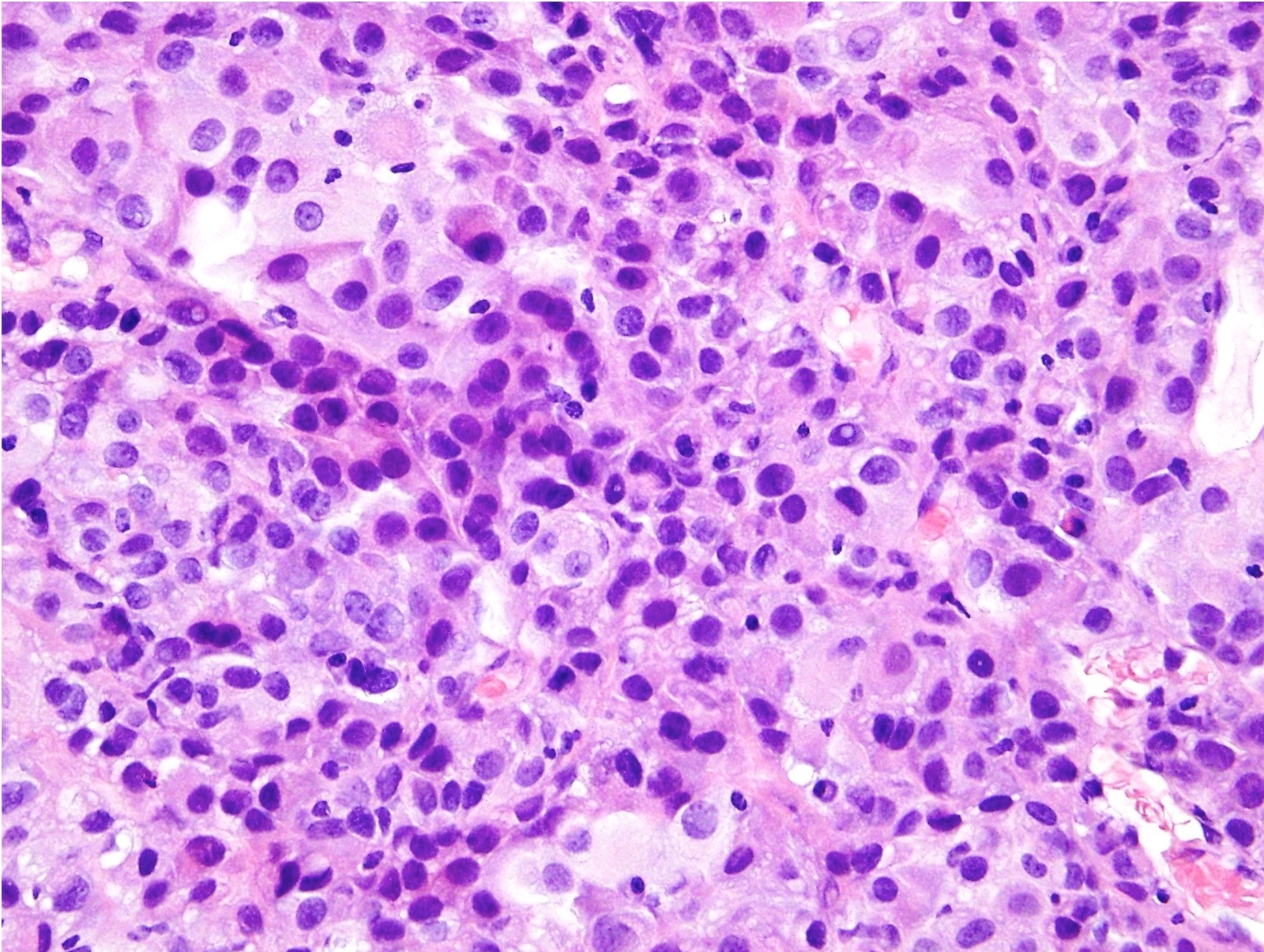
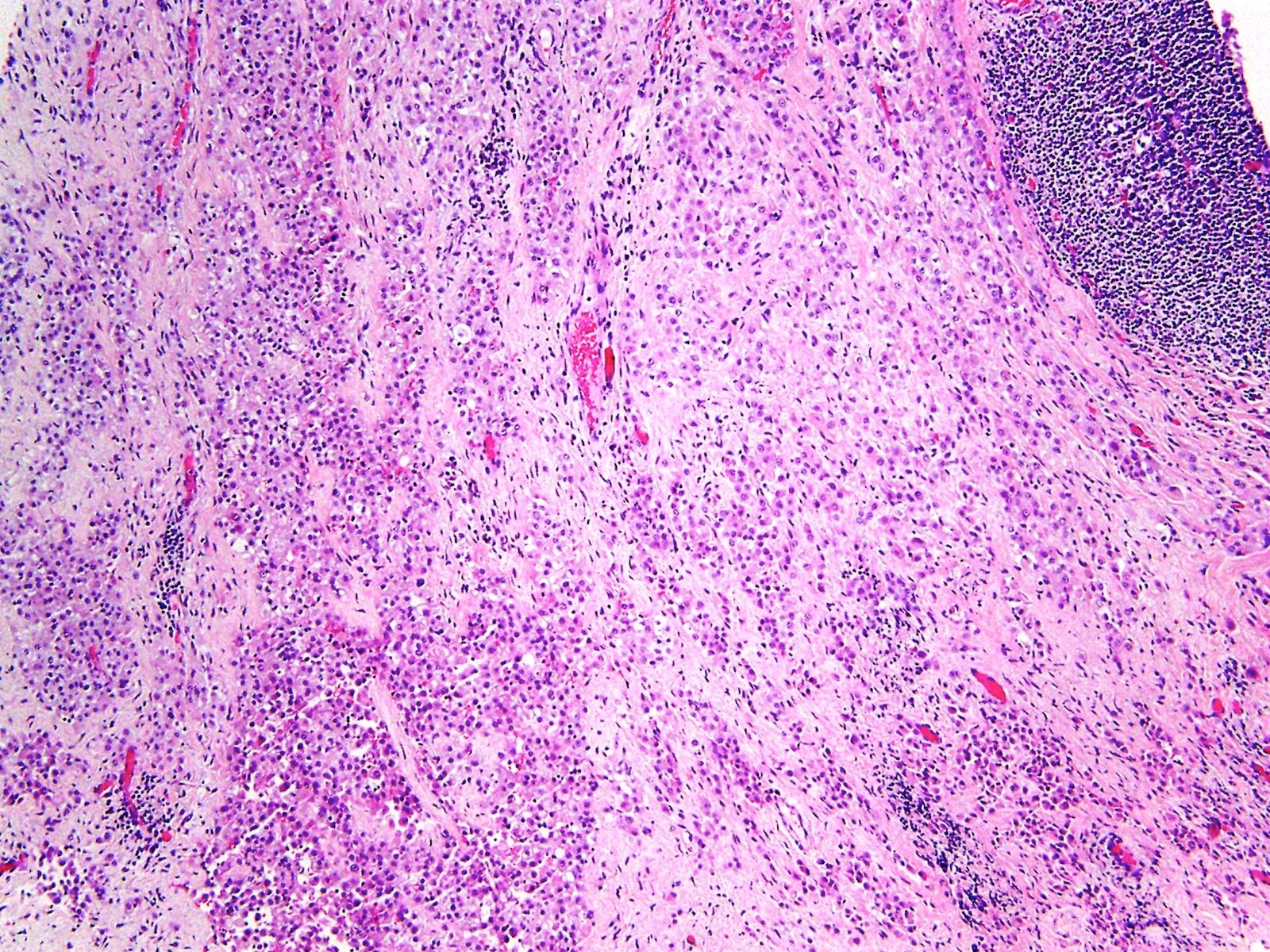
- Epithelioid mesothelioma is characterized by epithelioid to round tumor cells, which are often more monotonous than what are seen in most carcinomas
- Sarcomatoid mesothelioma is characterized by spindled tumor cells
- Biphasic mesothelioma is characterized by the presence of both epithelioid and sarcomatoid components, each comprising at least 10% of the tumor
- In epithelioid mesothelioma, architectural / cytologic features that can be seen are diverse; histologic patterns most commonly seen are tubular, papillary and solid and more rarely micropapillary, trabecular, acinar, adenomatoid-like, clear cell, deciduoid, adenoid cystic-like, signet ring cell, small cell and rhabdoid (Arch Pathol Lab Med 2013;137:647)
- In sarcomatoid mesothelioma, histologic patterns include conventional, desmoplastic, lymphohistiocytoid and those with heterologous differentiation (Arch Pathol Lab Med 2013;137:647, Am J Surg Pathol 2015;39:1568)
Microscopic (histologic) images
Contributed by Yin P. Hung, M.D., Ph.D.
Epithelioid variant, solid growth

Calretinin
WT1
Epithelioid variant, infiltrative growth
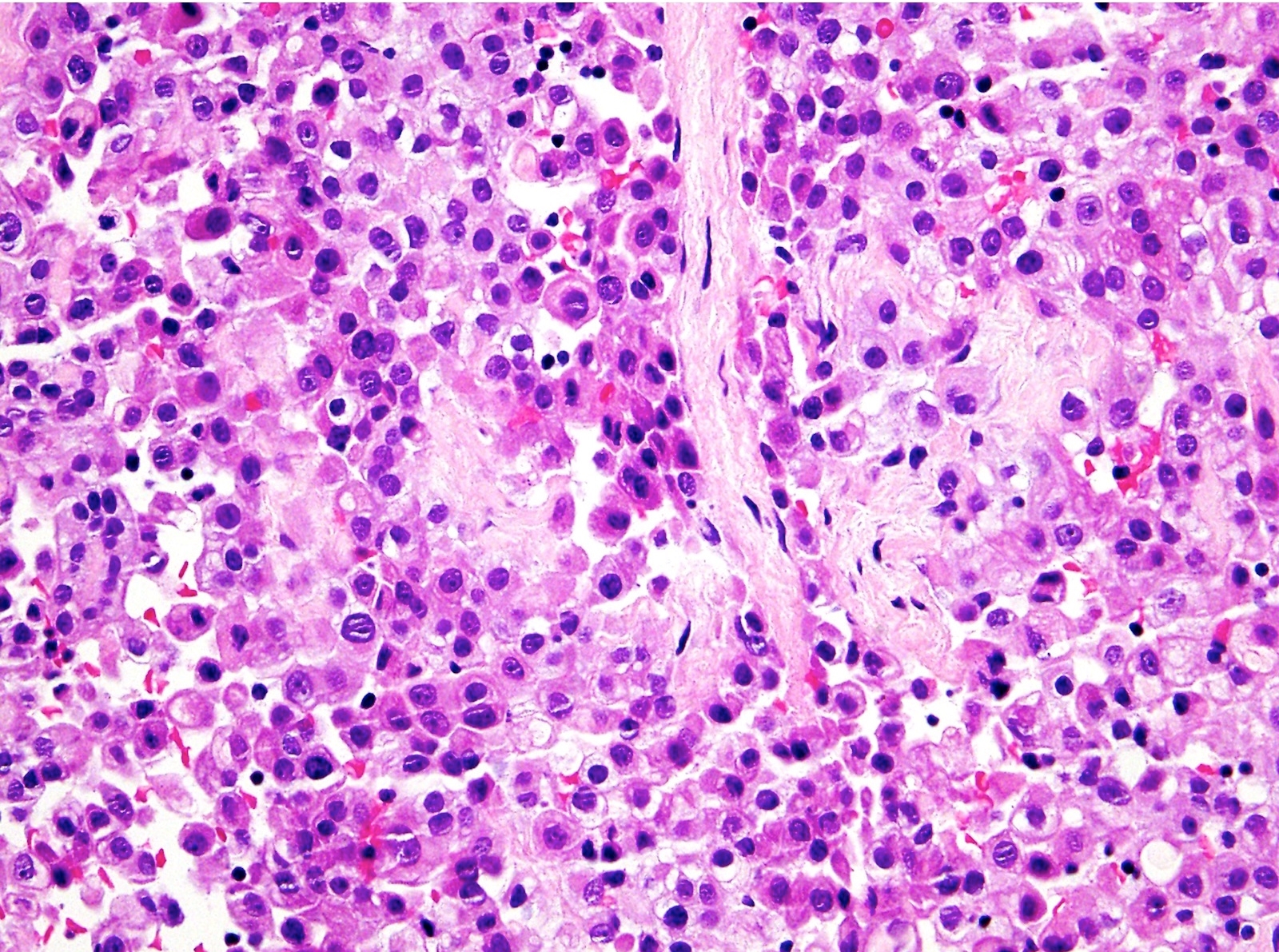
Typically uniform tumor cells
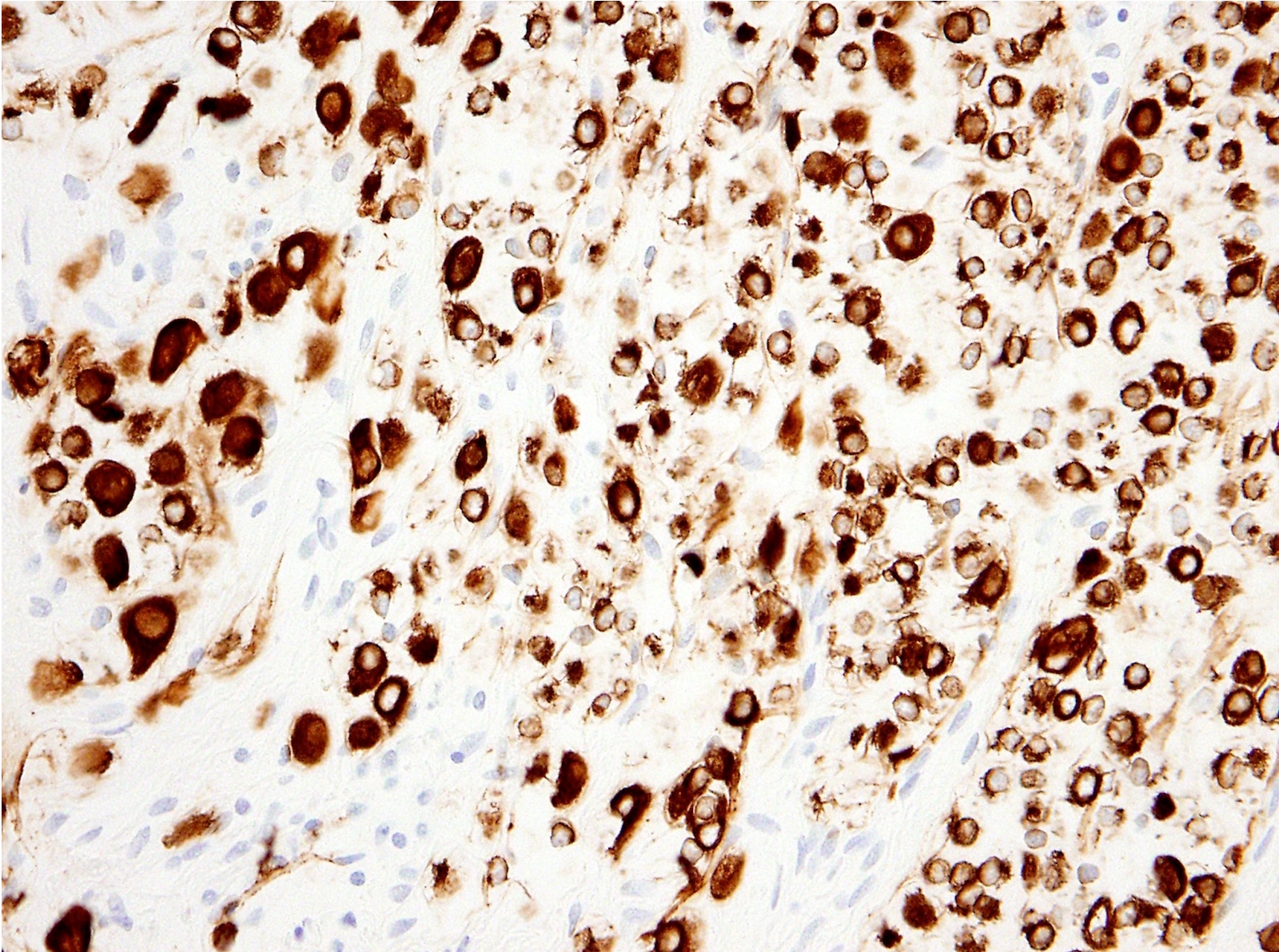
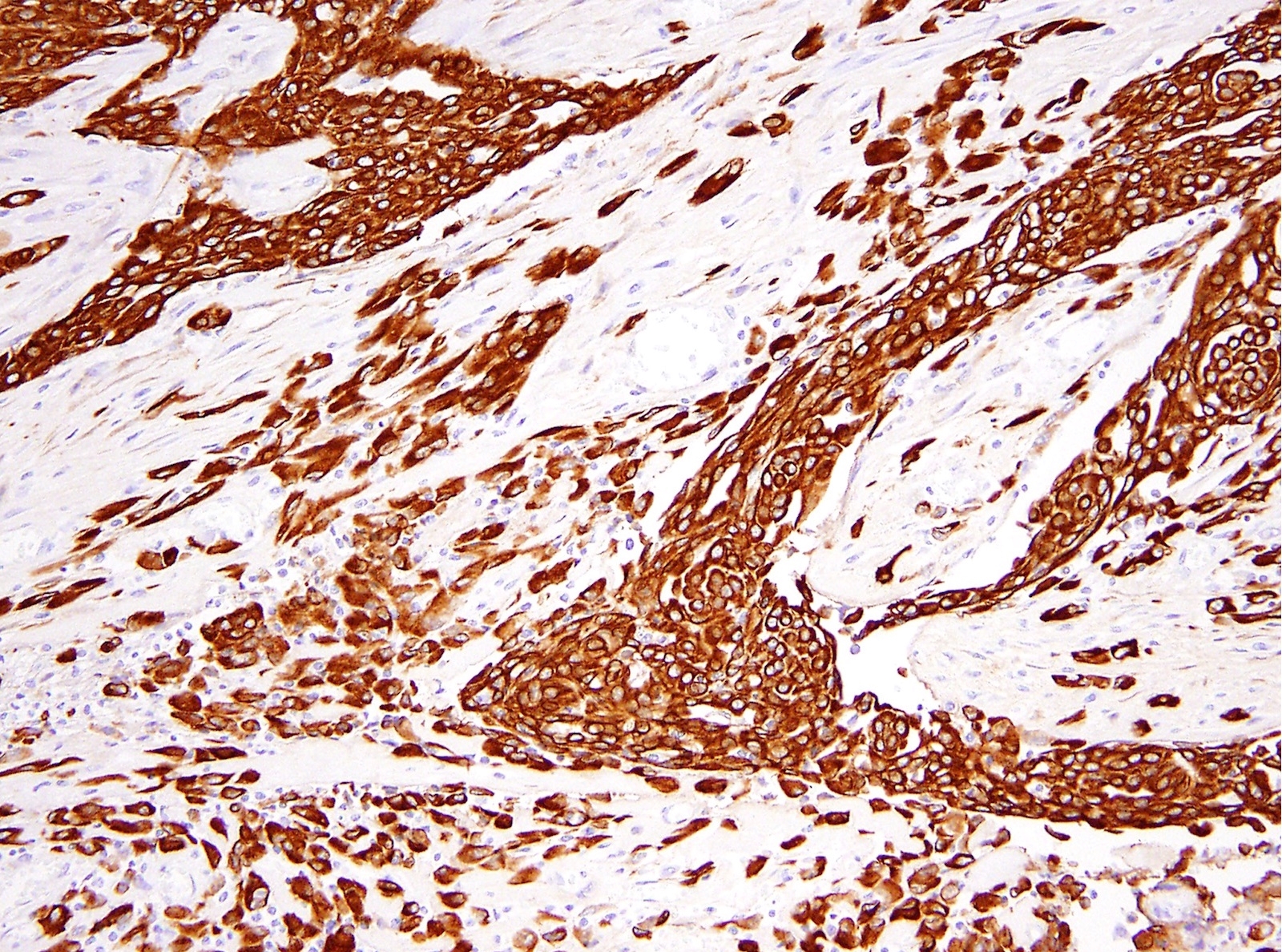
AE1 / AE3
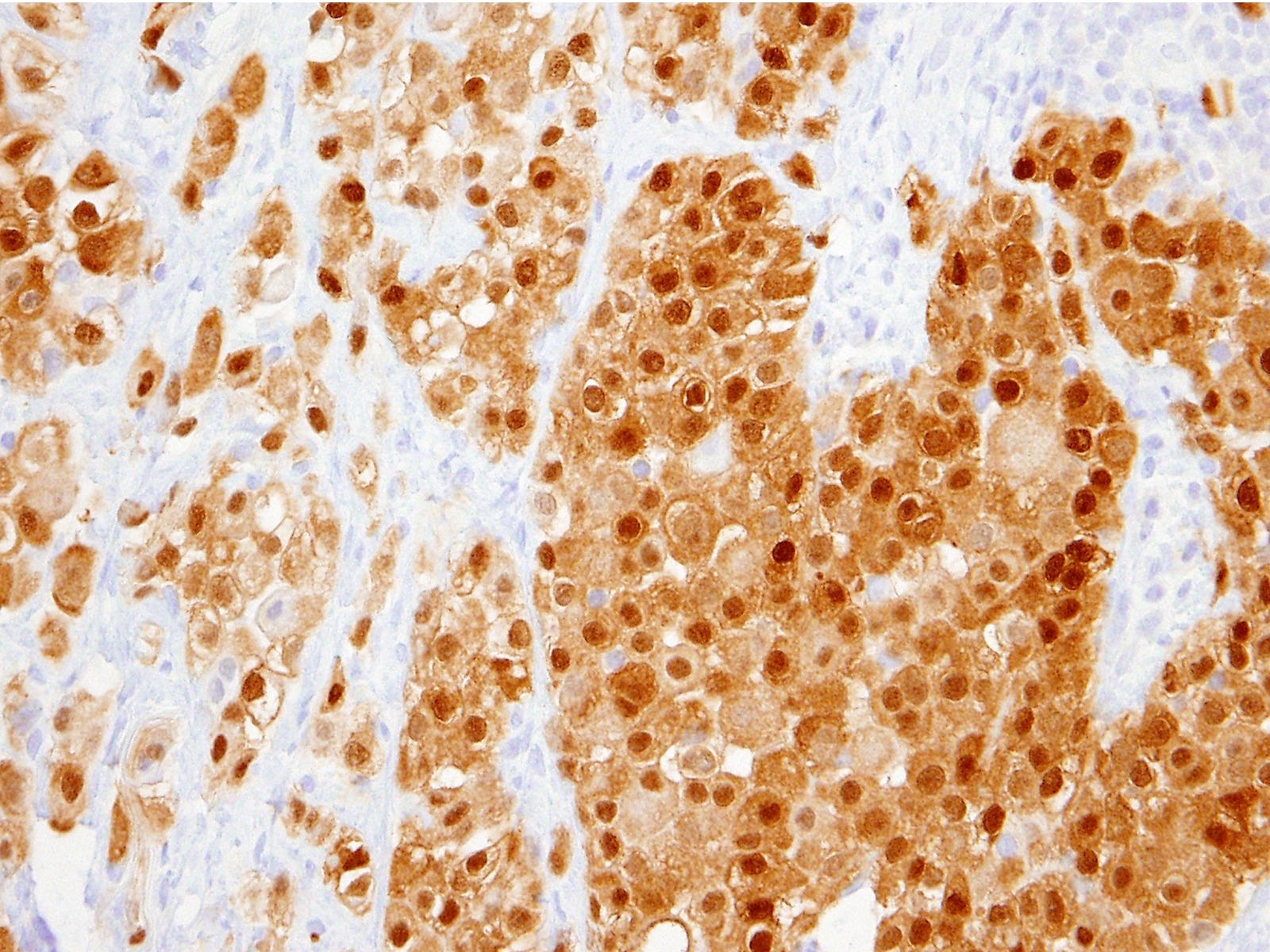
Calretinin
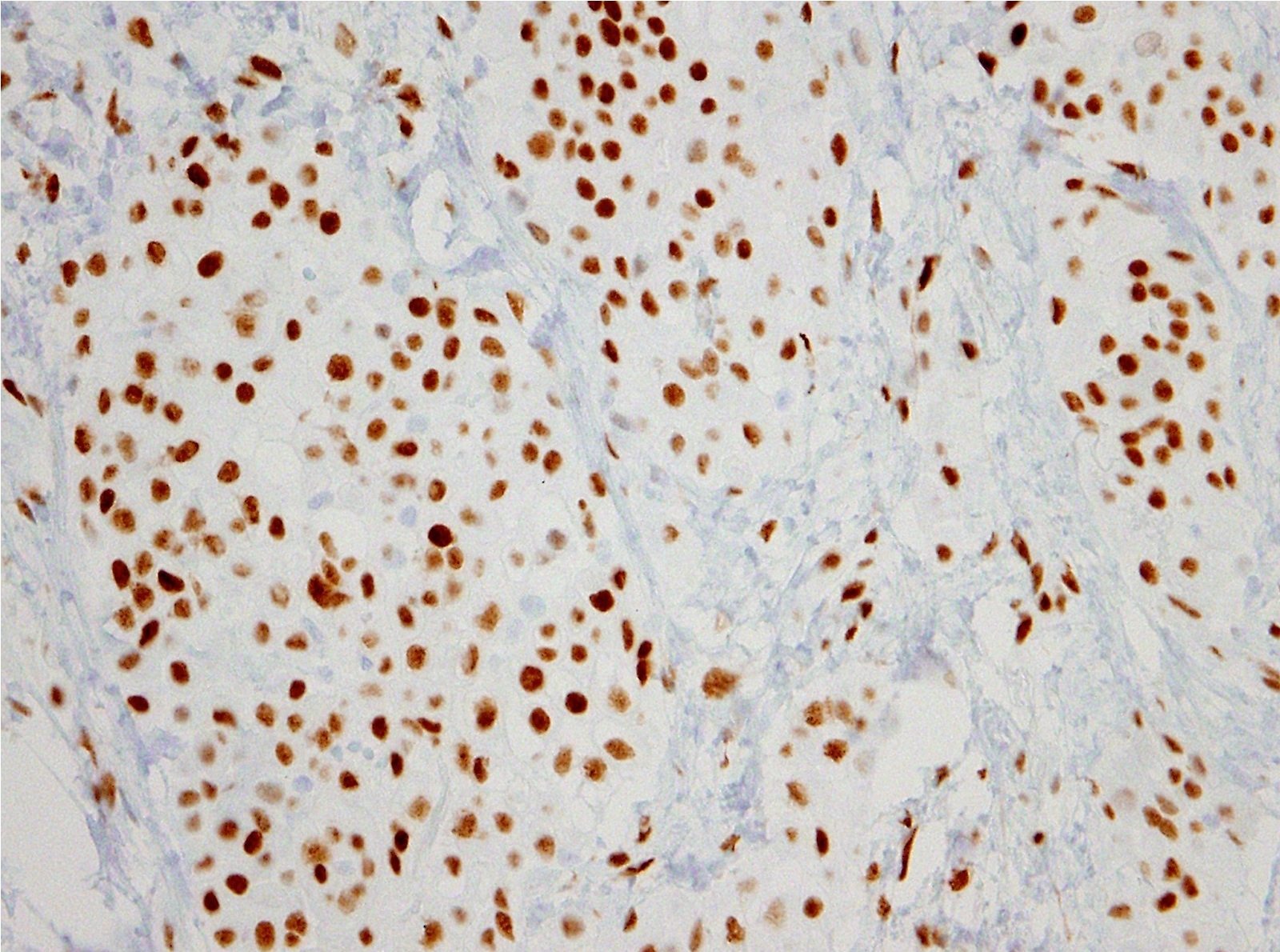
WT1
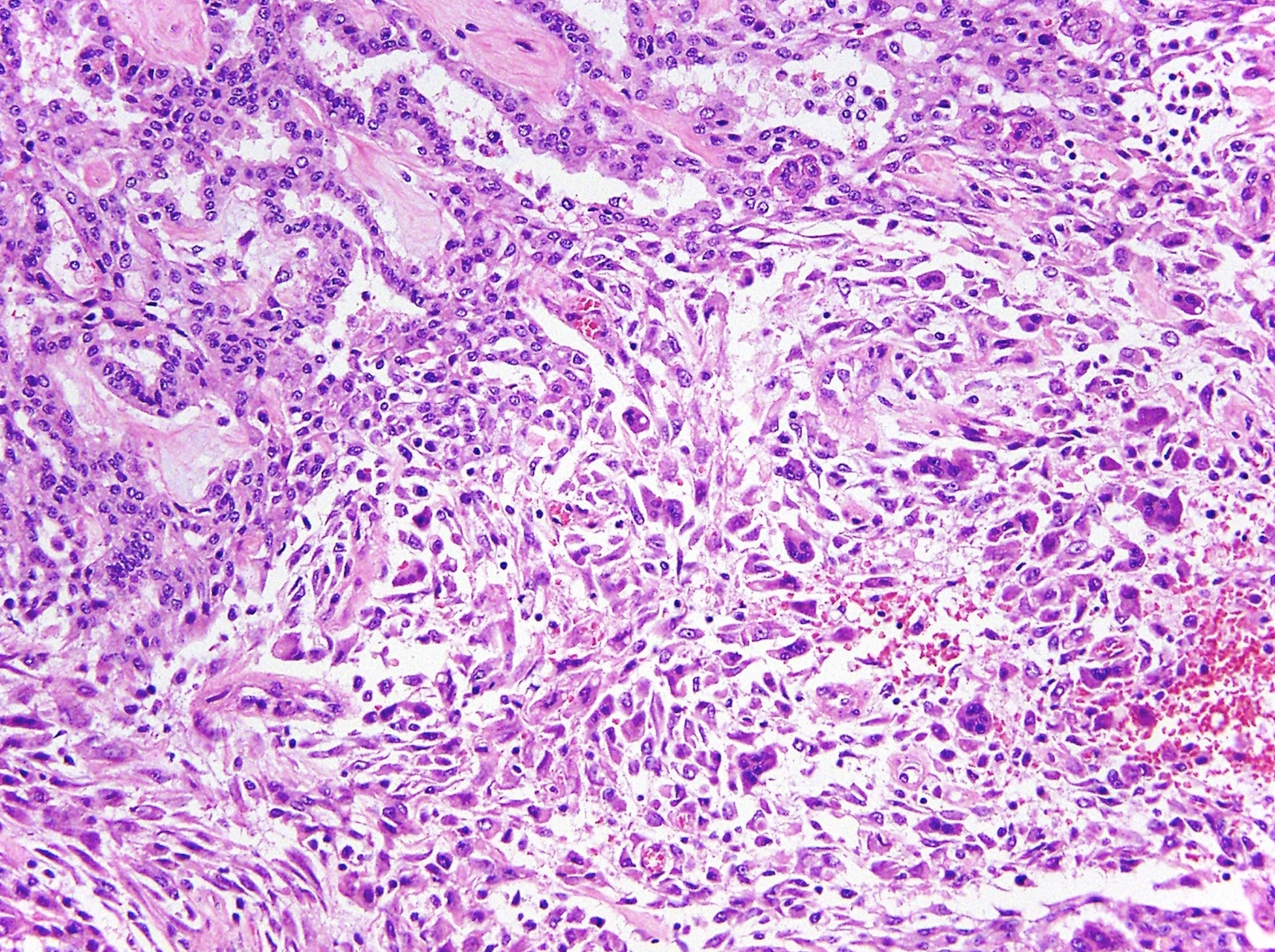
Biphasic variant
AE1 / AE3
Cytology description
- Large clusters to sheets of fairly monotonous mesothelial tumor cells
- Limitation of cytologic diagnosis: rarely definitive, since tissue invasion is difficult to assess
Positive stains
- Mesothelial markers: calretinin, WT1 and D2-40 (podoplanin), CAIX (J Clin Pathol 2016;69:706, Arch Pathol Lab Med 2018;142:236, Arch Pathol Lab Med 2018;142:89)
- Keratins such as AE1 / AE3, CAM 5.2 and broad spectrum pankeratin
- Keratin 5 / 6: expressed in most epithelioid mesotheliomas (rarely adenocarcinomas)
- Mesothelin, thrombomodulin, HBME1
- GATA3: expressed in a large subset of sarcomatoid mesothelioma (also in breast and urothelial carcinoma)
Negative stains
- Epithelial markers: claudin4, BerEP4, MOC31, B72.3, CEA
- TTF1
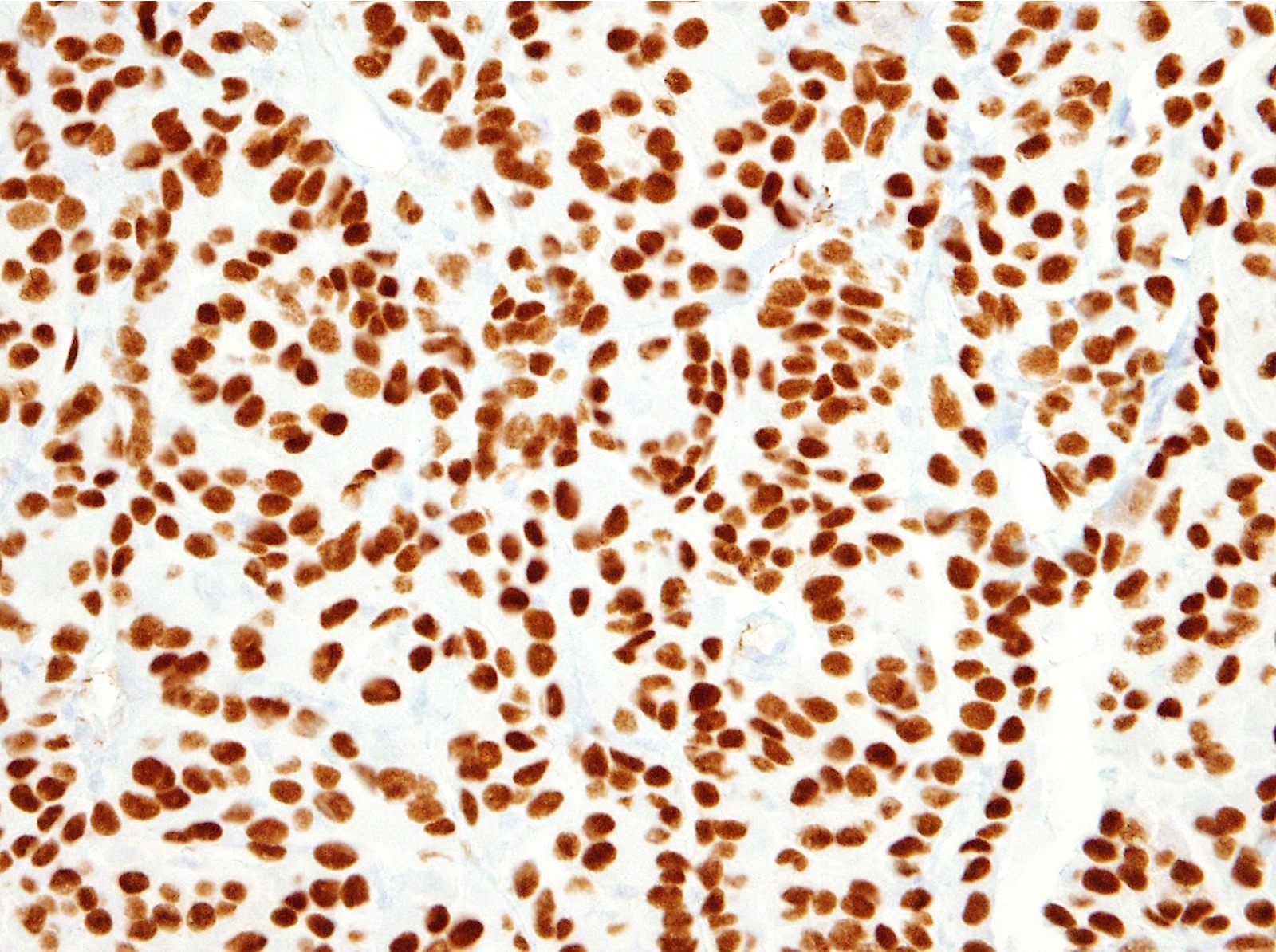
- BAP1: complete loss of BAP1 expression in 40 - 60% (lost in < 1% of carcinomas and not in reactive mesothelial proliferation) (Am J Surg Pathol 2015;39:977, Hum Pathol 2016;51:9, J Thorac Oncol 2017;12:724)
- PAX8: expression in 10 - 20% (Hum Pathol 2018;72:160, Am J Surg Pathol 2017;41:1675, Arch Pathol Lab Med 2018;142:89)
Electron microscopy description
- Microvilli and desmosomes
Molecular / cytogenetics description
- BAP1 somatic mutations in 40 - 70% (J Transl Med 2015;13:122, Mod Pathol 2017;30:246, J Thorac Oncol 2017;12:724)
- Copy number loss of BAP1 in 3p21, CDKN2A in 9p21 and NF2 in 22q12 in 20 - 40% (Mod Pathol 2010;23:531, Hum Pathol 2016;55:72)
- Somatic mutations in SETD2, DDX3X and others in a subset (Mod Pathol 2017;30:246)
- Germline mutations in BAP1, ATM or other regulators in DNA repair in a subset (J Clin Oncol 2018;36:2863, J Pediatr Hematol Oncol 2018;40:e511)
- EWSR1-ATF1 or FUS-ATF1 gene fusion in rare cases (Am J Surg Pathol 2017;41:980)
- ALK gene rearrangement in rare cases but enriched in young patients (JAMA Oncol 2018;4:235)
Sample pathology report
- Peritoneum and omentum, resection:
- Mesothelioma, epithelioid variant, 5.0 cm in greatest dimension
- Surgical margins, negative for tumor
- Comment: The tumor cells are positive for WT1, calretinin and D2-40, and are negative for claudin4, PAX8, MOC31 and CEA.
Differential diagnosis
- Metastatic adenocarcinoma
- Variable histologic overlap
- Typically expresses other epithelial markers: claudin4, BerEP4, polyclonal CEA, MOC31 and B72.3
- Rarely express keratin 5 / 6 and mesothelial markers (calretinin and D2-40), though WT1 is commonly expressed in carcinomas of Müllerian primary and CAIX is expressed in renal cell carcinoma, clear cell type
- Expression of PAX8 favors renal or gynecologic origin and TTF1 favors lung origin
- Sclerosing peritonitis
- Reactive proliferation of stromal myofibroblasts, often associated with adjacent linear arrangement of mesothelial cells, chronic inflammation, surface fibrin deposition and occasionally entrapped fat
- Associated with various conditions including luteinized thecomas (Am J Surg Pathol 1994;18:1)
- Distinction can be challenging, particularly in small biopsies, cases with tangential sectioning or fat entrapment (Am J Surg Pathol 2000;24:1183)
- Well differentiated papillary mesothelial tumor
- Most commonly in the peritoneum, rarely pleura and other sites
- Histology: papillae with myxoid cores, each lined by a single mesothelial cell layer
- Invasion is typically not present (Am J Surg Pathol 2014;38:990)
- Overall more indolent than peritoneal mesothelioma (Ann Surg Oncol 2019;26:852)
- Recurrent mutations in TRAF7 or CDC42 (Mod Pathol 2019;32:88)
- Adenomatoid tumor of genital type
- Benign mesothelial tumor that arises mostly commonly near the genital tract
- Histology: a microcystic low power appearance with poor margination and tubules / cords of epithelioid cells with characteristic cytoplasmic vacuolation
- Associated with immunosuppressive state in some cases (Histopathology 2018;73:1013)
- Recurrent mutations in TRAF7 (Mod Pathol 2018;31:660)
- Peritoneal inclusion cyst
- Also known as multilocular inclusion cyst
- Histology: multiple cysts of various sizes, each with thin fibrous walls lined by flattened mesothelial cells (Cancer 1989;64:1336)
- TNS3-MAP3K3 or ZFPM2-ELF5 gene fusion in rare cases (Cancer Lett 2015;357:502)
- Epithelioid hemangioendothelioma
- Rare distinctive malignant vascular tumor
- Most commonly involves liver, lung / pleura, bone or soft tissue
- Histology: cord-like pattern, myxohyaline matrix, epithelioid cells with intracytoplasmic vacuoles
- Immunohistochemistry: typically positive for CAMTA1 and endothelial markers (ERG, CD31, CD34 and D2-40) but negative for calretinin and WT1 (Am J Surg Pathol 2016;40:94)
- WWTR1-CAMTA1 gene fusion in most cases, YAP1-TFE3 fusion in rare cases (Sci Transl Med 2011;3:98ra82, Genes Chromosomes Cancer 2011;50:644, Genes Chromosomes Cancer 2013;52:775)
Board review style question #1
- Which of the following is true regarding peritoneal mesothelioma?
- All cases are associated with asbestos exposure
- Compared to pleural mesothelioma, peritoneal mesothelioma more likely involves women and children
- Copy number loss of CDKN2A and NF2 is detected in all cases
- Histologic subtyping has no prognostic value
- The presence of intact BAP1 protein expression rules out malignancy entirely
Board review style answer #1
B. Compared to pleural mesothelioma, peritoneal mesothelioma more likely involves women and children
Comment Here
Reference: Peritoneal mesothelioma
Comment Here
Reference: Peritoneal mesothelioma
Board review style question #2
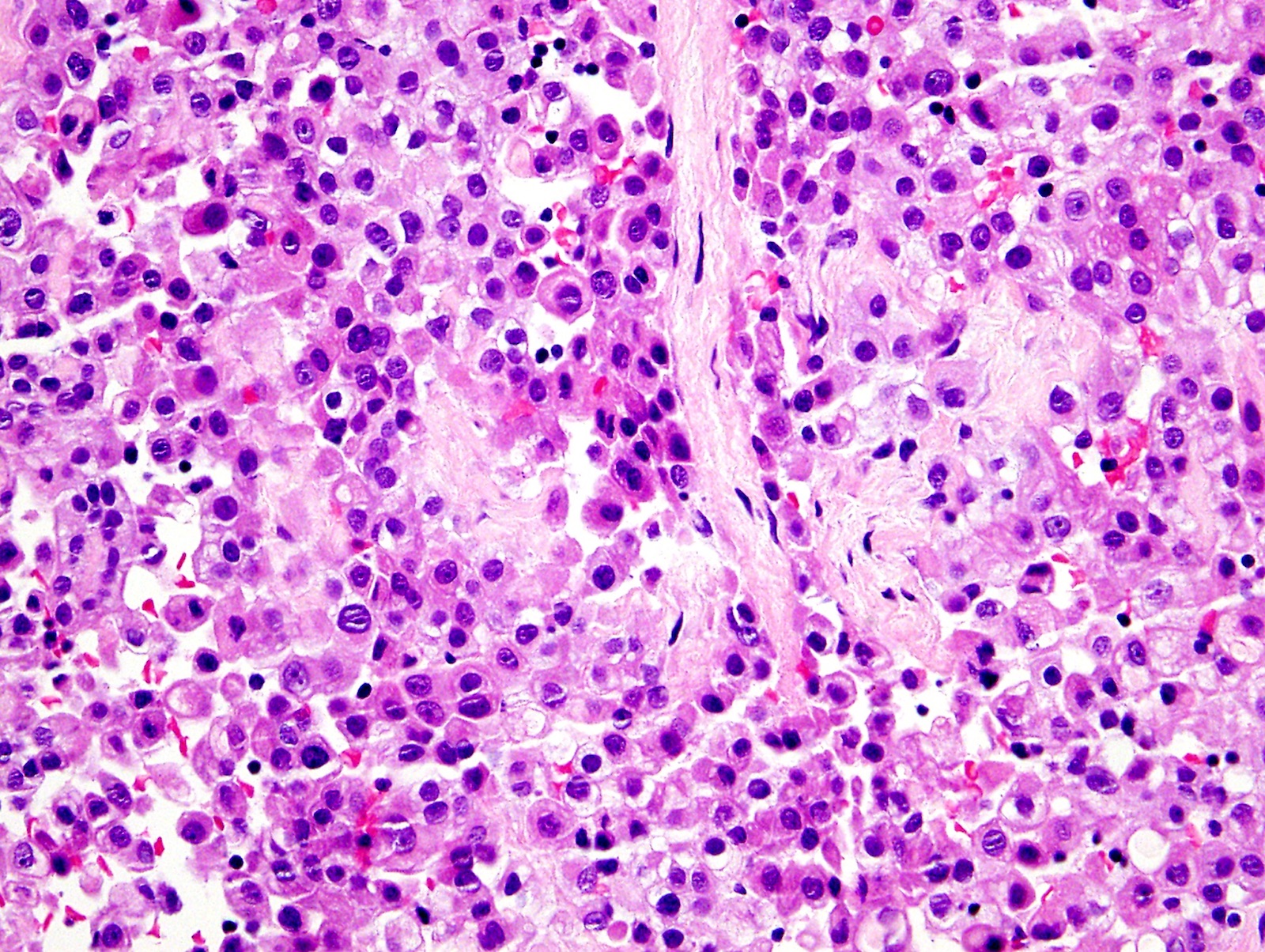
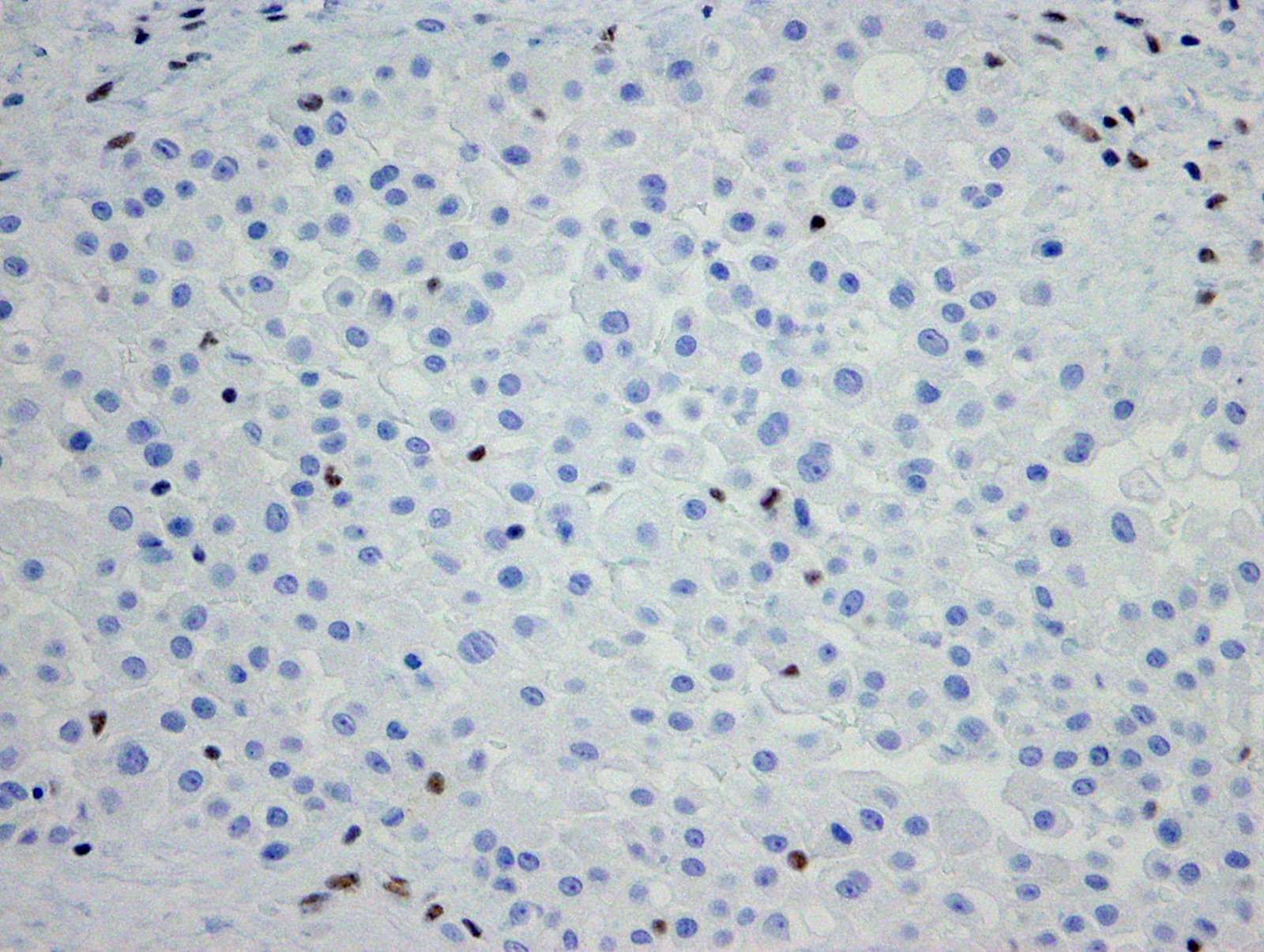
- Which of the following is true regarding the two images (the tumor and the corresponding BAP1 immunostain) illustrated?
- This indicates germline BAP1 mutation(s) in all cases
- This is a metastatic adenocarcinoma
- This is a reactive mesothelial proliferation
- This is a sarcomatoid mesothelioma
- This is an epithelioid mesothelioma
Board review style answer #2
