Ovary
Sex cord stromal tumors
Pure stromal tumors
Thecoma
Editorial Board Member: Gulisa Turashvili, M.D., Ph.D.
Deputy Editor-in-Chief: Jennifer A. Bennett, M.D.

Last author update: 25 June 2021
Last staff update: 1 May 2024
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed search: Ovarian thecoma
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Frozen section description | Frozen section images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Collins V, Kalir T. Thecoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/ovarytumorthecoma.html. Accessed September 29th, 2025.
Definition / general
- Ovarian stromal neoplasm, almost always benign, composed of cells resembling theca cells
Essential features
- Almost always benign
- Usually occurs in postmenopausal women who present with uterine bleeding
- Histology shows a predominant population of cells with ovoid to round nuclei and pale gray cytoplasm
- Reticulin stain and molecular testing for FOXL2 mutation help distinguish thecoma from adult granulosa cell tumor
Terminology
- Theca cell tumor
ICD coding
- ICD-O: 8600/0 - thecoma, NOS
- ICD-10: D27 - benign neoplasm of ovary
- ICD-11: 2F32.Y & XH34A0 - other specified benign neoplasm of ovary & thecoma, NOS
Epidemiology
- Uncommon
- Usually postmenopausal women
- Mean age = 59 years (Ann Diagn Pathol 2008;12:12)
- Age ranges from 16 to 81 (Am J Surg Pathol 2014;38:1023)
Sites
- Ovary
Pathophysiology
- Molecular alterations, such as trisomy 12 and loss of heterozygosity (LOH) at the PTCH gene (see Molecular / cytogenetics description)
Etiology
- Unknown
Clinical features
- May be discovered incidentally
- Most common symptom is postmenopausal bleeding (Am J Surg Pathol 2014;38:1023)
- Symptoms can be related to mass: pelvic pain / pressure
- May present with estrogenic or androgenic manifestations
- Associated with endometrial hyperplasia and malignancy
Diagnosis
- Histologic examination
Laboratory
- Occasionally elevated serum inhibin A and inhibin B (Gynecol Oncol Rep 2020;34:100658, Gynecol Endocrinol 2016;32:872)
Radiology description
- Sonographic features:
- Adnexal hypoechoic mass with clear border and acoustic attenuation
- Minimal Doppler flow signal (J Ovarian Res 2016;9:81)
- Magnetic resonance imaging features:
- Isointense or slightly hyperintense
- Pelvic fluid accumulation (Medicine (Baltimore) 2020;99:e20358)
- Computed tomography features:
- Isodense or hypodense (J Comput Assist Tomogr 2012;36:46)
- Occasionally thecomas have positive F-FDG uptake on PET scan (J Obstet Gynaecol Res 2017;43:599)
Radiology images
Images hosted on other servers:

Bilateral thecomas on MRI
Prognostic factors
- Thecomas are almost always benign but may be associated with endometrial malignancy
Case reports
- 57 year old woman with postmenopausal bleeding and elevated serum inhibin B level (Gynecol Oncol Rep 2020;34:100658)
- 58 year old woman with progressive scalp hair loss (Skin Appendage Disord 2019;5:259)
- 61 year old woman with Meigs syndrome and elevated CA-125 level (J Menopausal Med 2015;21:56)
Treatment
- Oophorectomy if fertility sparing is desired
- Total hysterectomy with bilateral salpingo-oophorectomy is indicated in postmenopausal patients
- References: Gynecol Oncol 1994;55:S62, Acta Radiol Oncol 1980;19:241, Gynecol Oncol 1985;21:135
Clinical images
Images hosted on other servers:

Bitemporal hair loss

Frontal balding and hirsutism
Gross description
- Usually unilateral
- Most are < 5 cm
- Solid, yellow and lobulated or white with focal yellow areas
- Occasionally cystic change and hemorrhage are present
- Necrosis is rare (Am J Surg Pathol 2014;38:1023)
Gross images
Contributed by Victoria Collins, M.D., Tamara Kalir, M.D., Ph.D. and AFIP
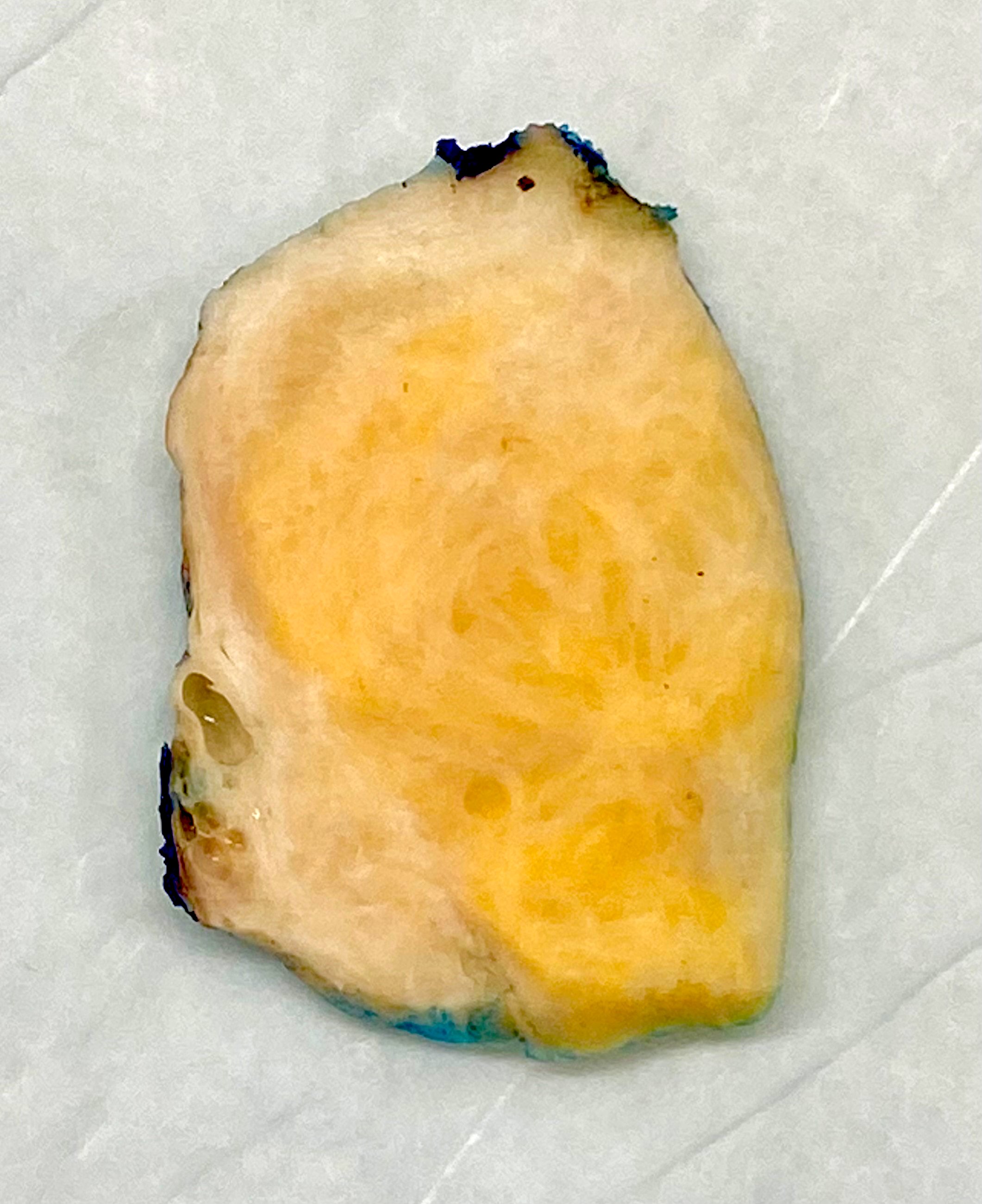
Well circumscribed, yellow-tan mass

Lobulated and yellow
Images hosted on other servers:

Yellow, lobulated mass
Frozen section description
- Sheets of oval to round cells with moderate to abundant pale gray cytoplasm
- Bilaterality should raise suspicion for metastasis
- Signet ring cells may be missed on frozen section and misinterpreted as fibrothecoma (Yeungnam Univ J Med 2019;36:163)
Frozen section images
Contributed by Victoria Collins, M.D. and Tamara Kalir, M.D., Ph.D.

Spindled to ovoid cells

Moderate cytoplasm
Microscopic (histologic) description
- Predominant population of cells showing ovoid to round nuclei and pale gray cytoplasm, which can be abundant
- Minor component of the tumor may have spindled nuclei, reflecting overlap between fibroma and thecoma
- Indistinct cell membranes impart a syncytial appearance
- Diffuse or nodular growth pattern
- Absent or minimal nuclear atypia
- Mitotic rate usually < 5/10 high power fields
- Hyaline plaques
- Cytoplasmic lipid vacuoles may be present but are not essential
- May show aggregates of cells with brightly eosinophilic cytoplasm (lutein cells)
- Calcification is more common in young patients (Int J Gynecol Pathol 1988;7:343)
- Uncommon features include keloid-like sclerosis, nuclear grooves, bizarre nuclear atypia (Am J Surg Pathol 2014;38:1023)
- Rarely contains a minor component of sex cord elements (Int J Gynecol Pathol 1983;2:227)
- Malignant thecoma: very rare, diagnosis requires diffuse moderate to severe nuclear atypia and high mitotic rate (> 4/10 high power fields) (Am J Surg Pathol 2011;35:e15)
Microscopic (histologic) images
Contributed by Victoria Collins, M.D., Tamara Kalir, M.D., Ph.D., AFIP and @SeoparjooAzmel on Twitter
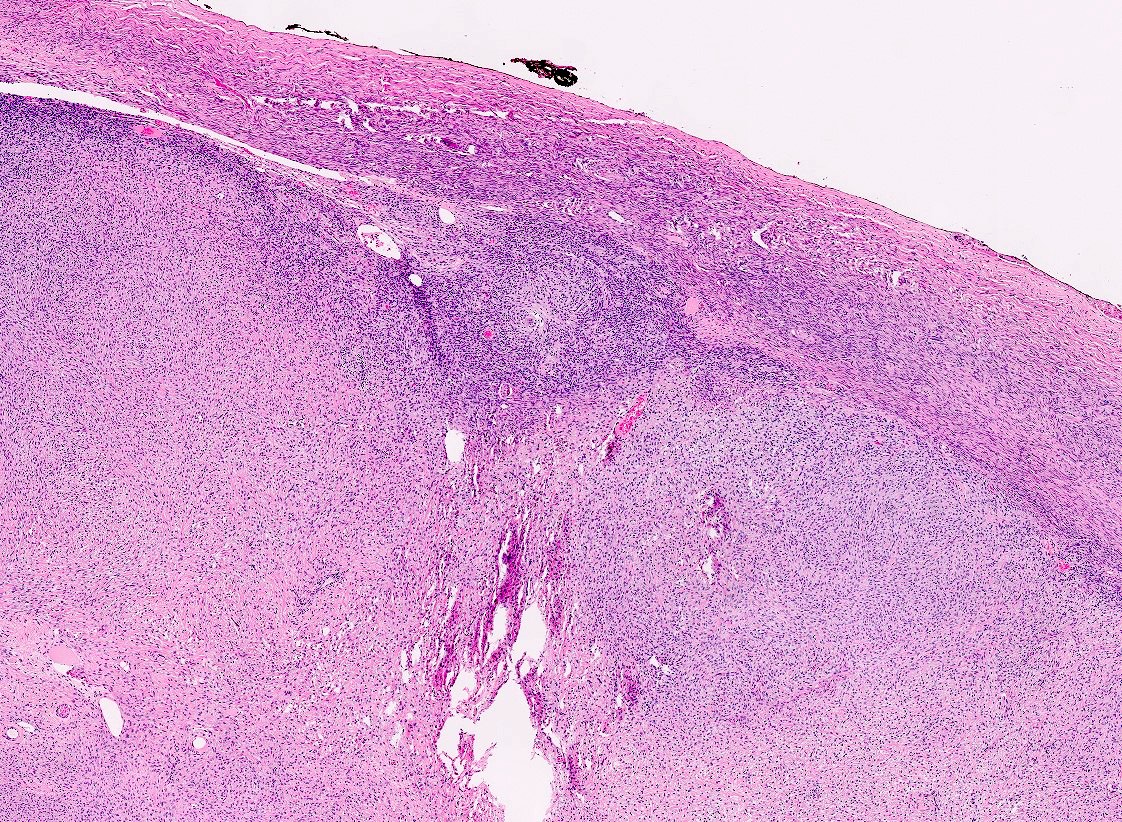
Well circumscribed

Ovoid to round cells
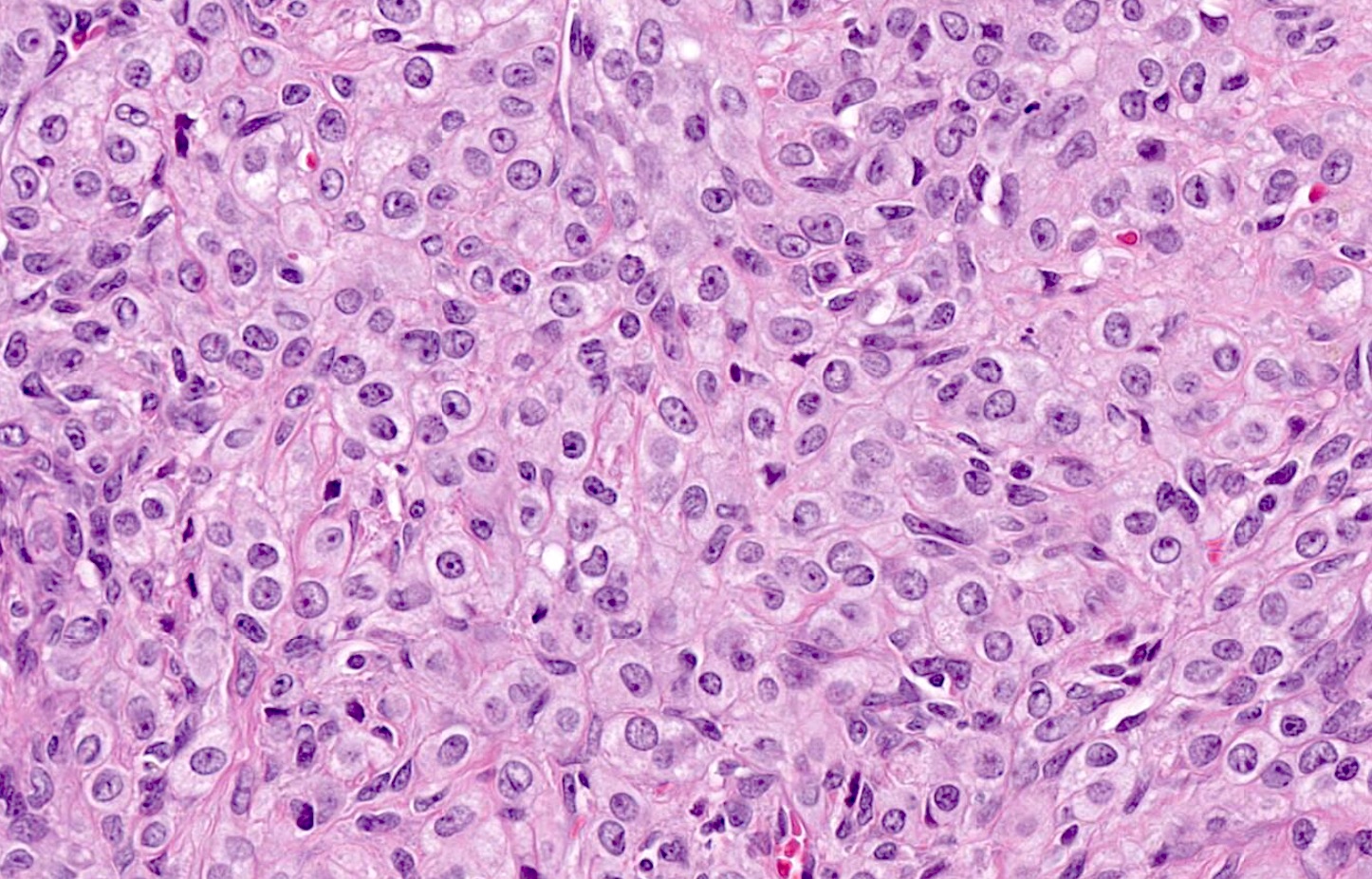
Mild nuclear atypia
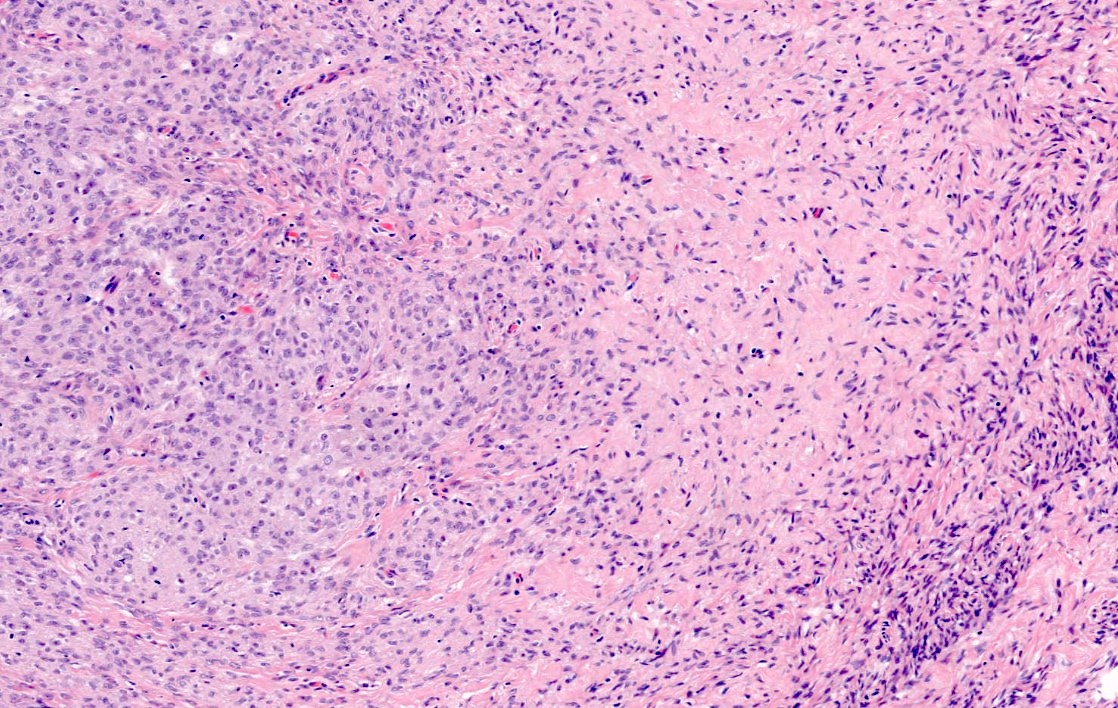
Thecoma and fibroma areas

Cystic change
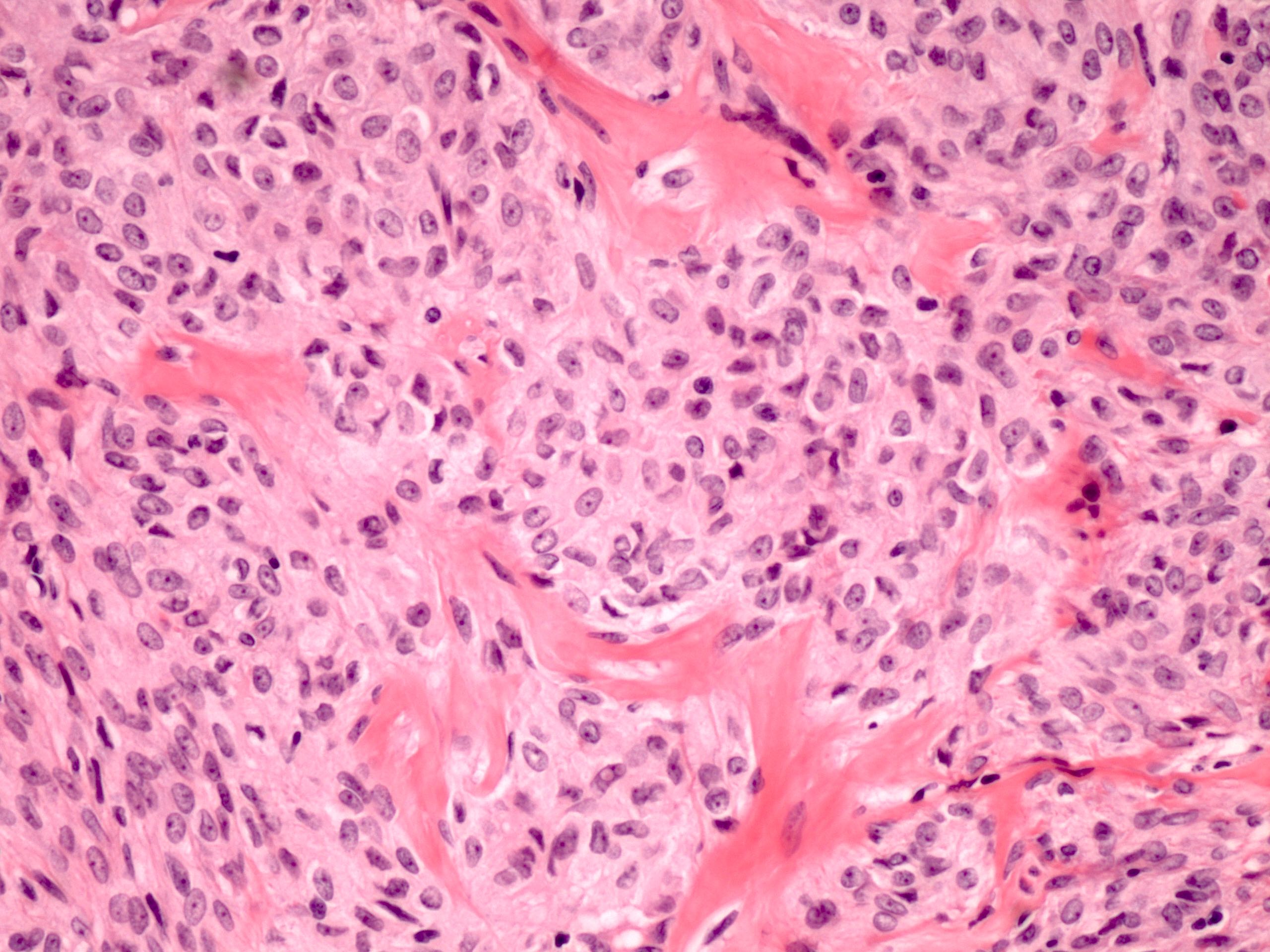
Hyaline plaques
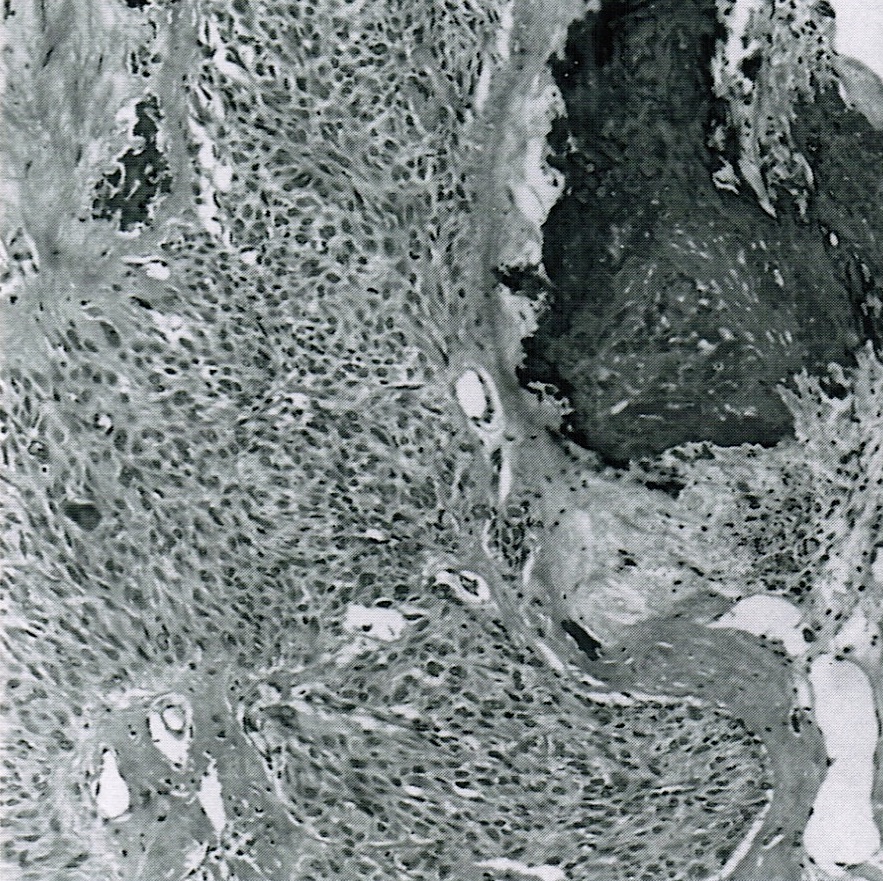
Stromal calcification
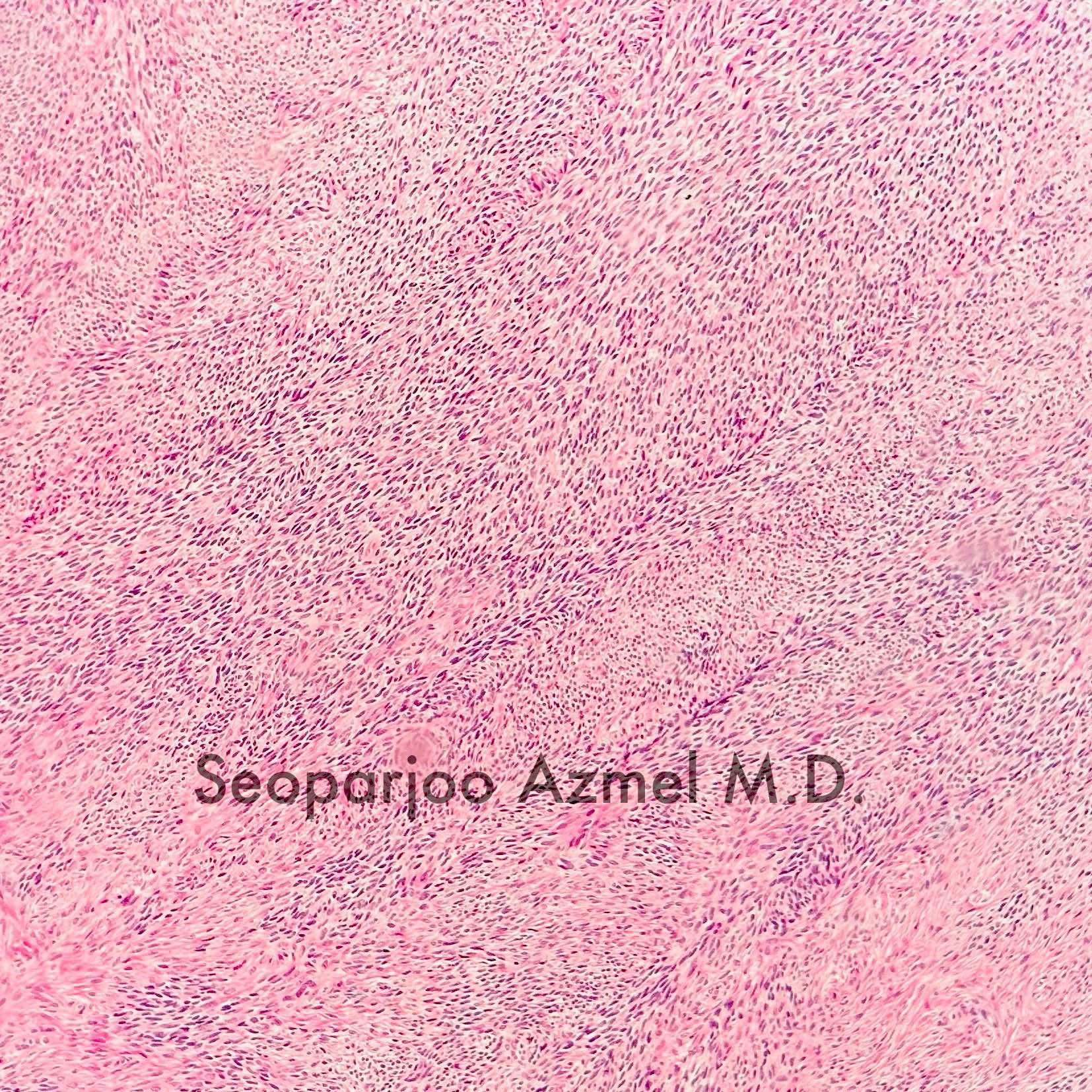
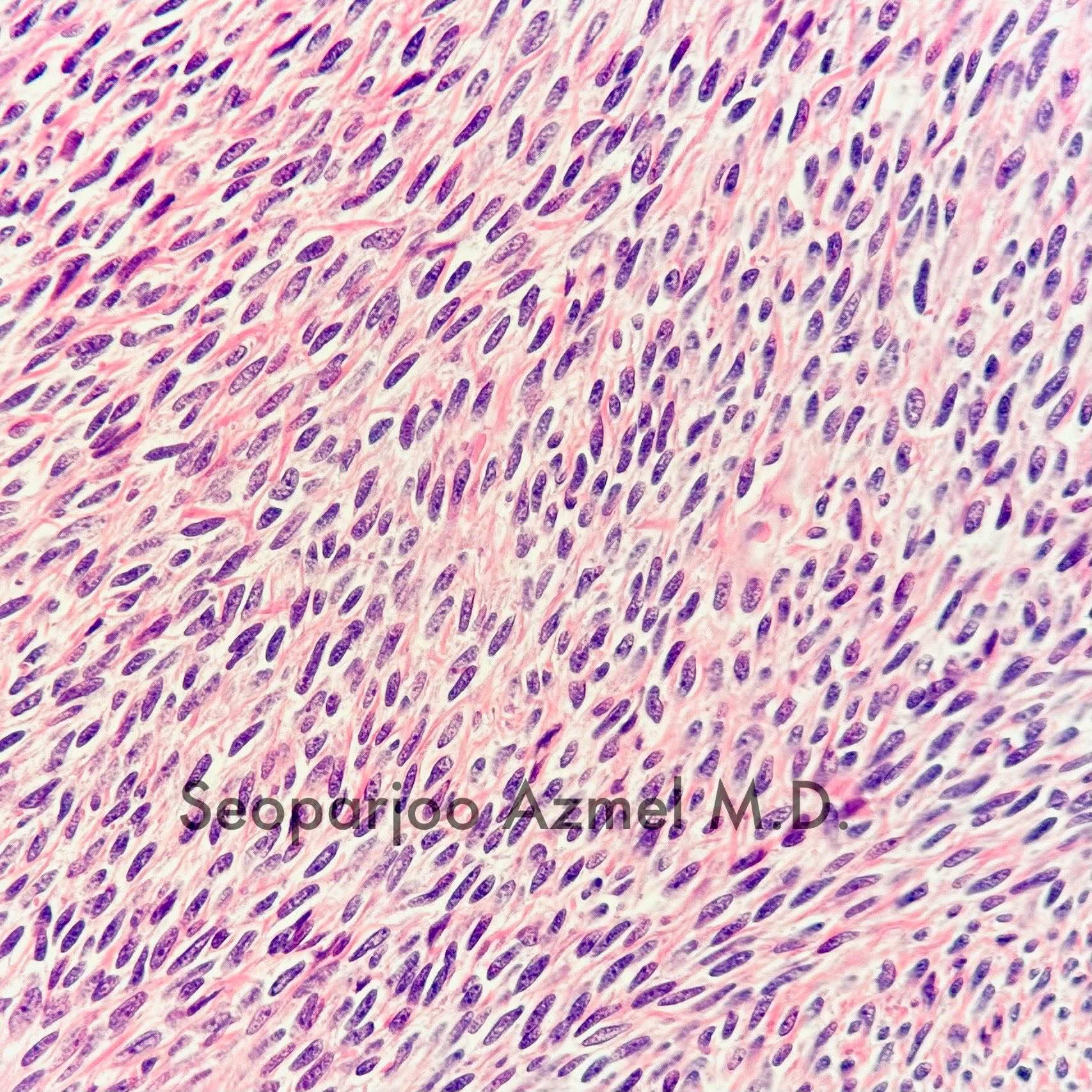
Thecoma
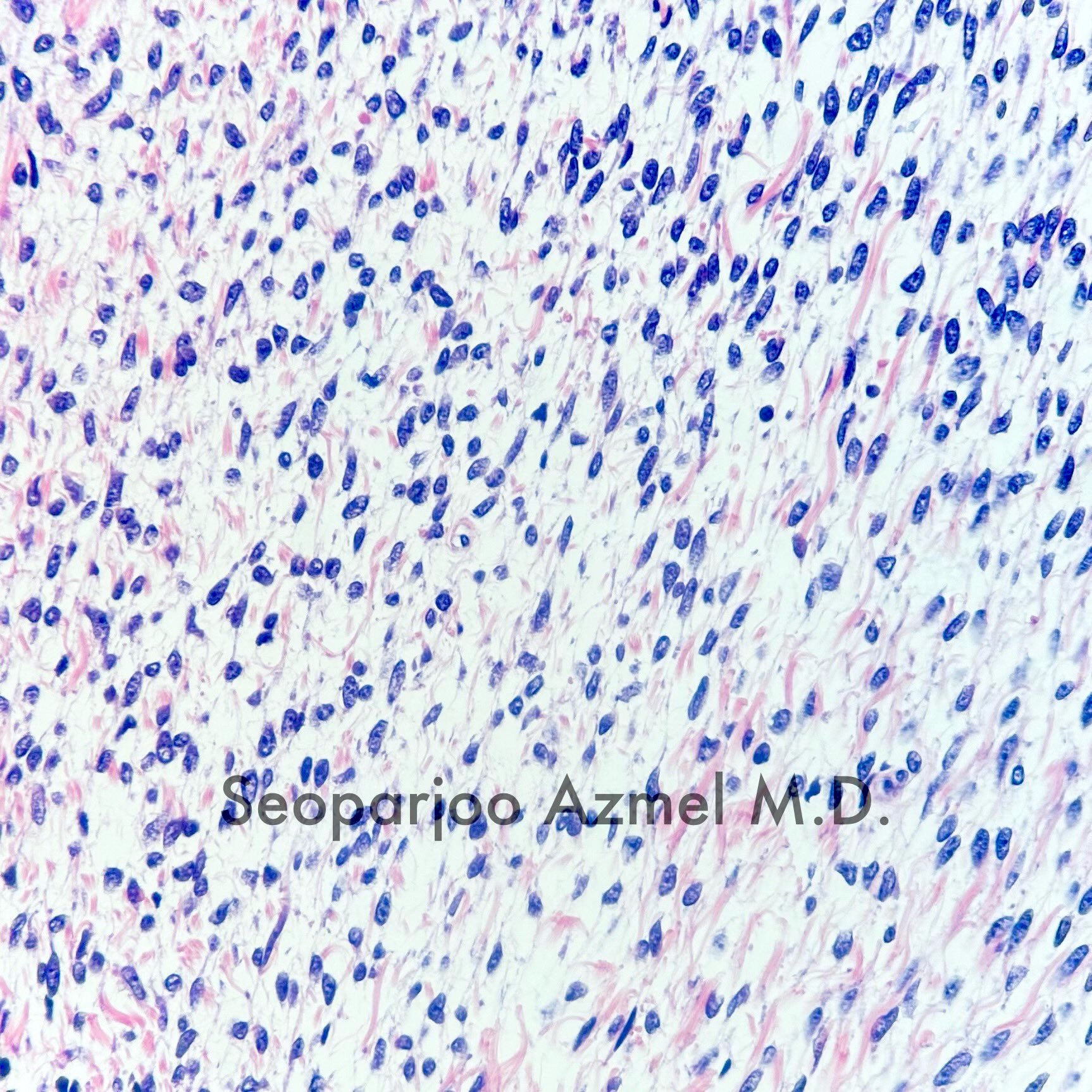
Thecoma
Vacuolated tumor cells
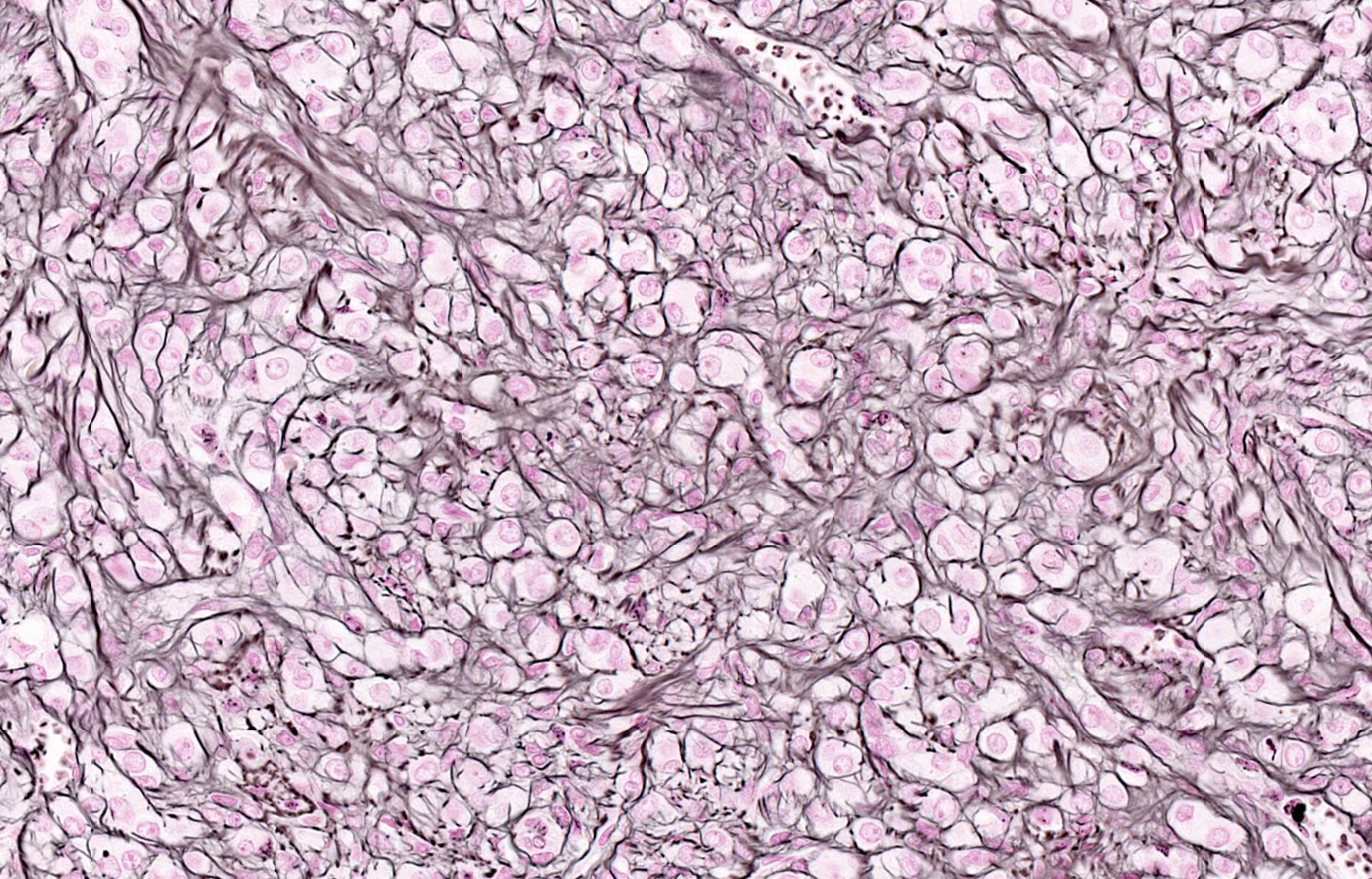
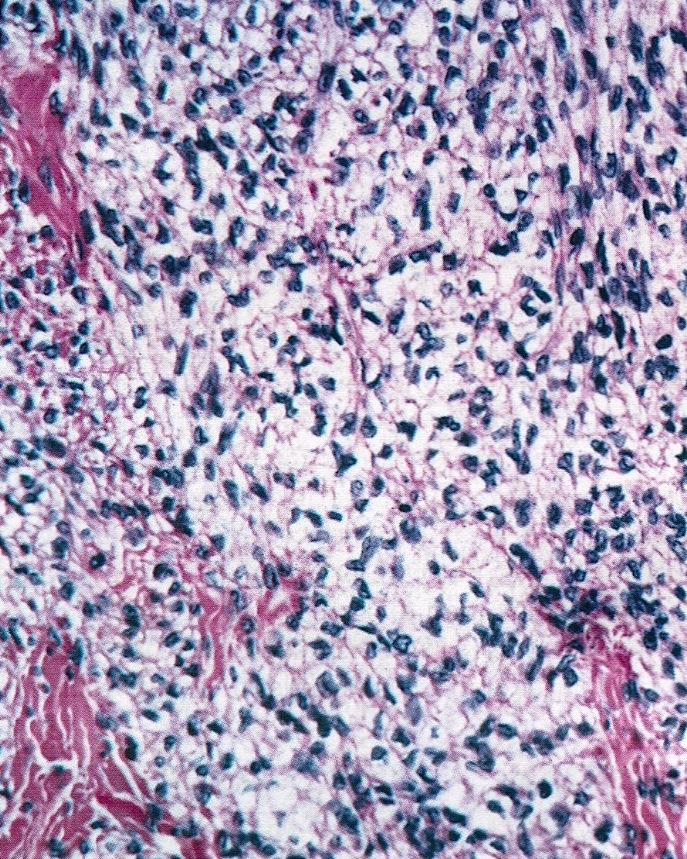
Reticulin
Inhibin
Oil red O stain
Virtual slides
Images hosted on other servers:

Thecoma, with cystic change

Thecoma, reticulin stain
Positive stains
- Inhibin
- Calretinin
- Reticulin stain shows a pericellular pattern (Int J Gynecol Pathol 2018;37:305)
- SF1
- FOXL2 (Mod Pathol 2013;26:860)
- WT1 (Am J Surg Pathol 2009;33:354)
- CD56 (Am J Surg Pathol 2008;32:884)
- Vimentin
- Oil red O in lipid rich cells
- GLUT5 in FDG PET positive tumors (J Obstet Gynaecol Res 2017;43:599)
Negative stains
Electron microscopy description
- Cytoplasmic lipid (Ultrastruct Pathol 1992;16:363)
- Type I cells: dispersed chromatin, basal lamina investment of each cell, coiled / branching rough endoplasmic reticulum, sparse smooth endoplasmic reticulum, irregular mitochondria
- Type II cells: degenerative changes, large round mitochondria with incomplete cristae and centers displaced by microfilaments (Hum Pathol 1984;15:153)
Molecular / cytogenetics description
- Trisomy 12 or tetrasomy 12 (Gynecol Oncol 1990;36:413, Cancer Genet Cytogenet 1993;71:180)
- Trisomy 4 (Gynecol Oncol 1992;45:66)
- Loss of heterozygosity (LOH) at 9q22.3 (PTCH1) and 19p13.3 (Hum Pathol 2005;36:792)
- FOXL2 mutation has been reported in a subset of thecomas (3 out of 14 tumors in one series) (N Engl J Med 2009;360:2719)
- However these may represent misdiagnosed granulosa cell tumors (PLoS One 2009;4:e7988)
- Pericellular reticulin staining is 100% specific for absence of FOXL2 mutation (Int J Gynecol Pathol 2018;37:305)
Videos
Thecoma of ovary
Ovarian pathology
Sample pathology report
- Right ovary and fallopian tube, salpingo-oophorectomy:
- Ovarian thecoma
- Fallopian tube with no significant pathologic changes
Differential diagnosis
- Adult granulosa cell tumor:
- Reticulin stain shows nested pattern (Int J Gynecol Pathol 2019;38:143)
- Harbors FOXL2 mutation (Mod Pathol 2013;26:860, Int J Gynecol Pathol 2018;37:305)
- Fibroma:
- Intersecting bundles of spindle cells producing collagen
- A morphologic spectrum between fibroma and thecoma exists
- Indeterminate tumors have been called fibrothecoma
- Luteinized thecoma associated with sclerosing peritonitis:
- Younger age at presentation (median age: 28)
- Symptoms include abdominal pain, ascites and bowel obstruction
- Cutaneous involvement has been reported (Ann N Y Acad Sci 1985;448:231)
- Bland spindle cell proliferation circumferentially involving the ovarian cortex with sparing of the medulla
- Almost always bilateral (Am J Surg Pathol 2008;32:1273)
- Sclerosing stromal tumor:
- Pseudolobular growth pattern with cellular nodules separated by dense collagenous or edematous connective tissue (Cancer 1973;31:664)
- Staghorn vessels
- Microcystic stromal tumor:
- Small, anastomosing cysts
- Inhibin-, calretinin-
- Nuclear beta catenin+
- Cyclin D1+
- CD10+ (Am J Surg Pathol 2015;39:1420)
- Steroid cell tumor, NOS:
- FOXL2- (Am J Surg Pathol 2011;35:484)
- Polygonal cells with abundant eosinophilic cytoplasm
- Typically has a component of lipid rich cells (pale and vacuolated) (Arch Pathol Lab Med 2018;142:1459)
- Leydig cell tumor:
- Tumor centered in ovarian hilus
- Cytoplasmic Reinke crystals
- Nuclei tend to cluster, forming eosinophilic nuclei free zones (Int J Gynecol Pathol 1989;8:299)
- Fibrinoid necrosis of blood vessel walls
Additional references
Practice question #1
A 59 year old woman presents with bitemporal hair loss and hirsutism. Exploratory laparotomy reveals a 6 cm right ovarian mass, which is resected. Which of the following is true of this tumor?
- 30 - 40% are malignant
- CD10 positive
- Harbors a FOXL2 mutation
- Reticulin stain shows a pericellular pattern
Practice answer #1
Practice question #2

A 62 year old woman presents with postmenopausal bleeding and on workup is found to have a 5 cm left ovarian mass. Which of the following immunostains is typically positive in this tumor?
- AE1 / AE3
- CD99
- Cyclin D1
- DOG1
- Inhibin
Practice answer #2
