

Thyroid & parathyroid
Cytology
Fine needle aspiration
FNA-general
Editorial Board Member: Marc Pusztaszeri, M.D.
Deputy Editor-in-Chief: Andrey Bychkov, M.D., Ph.D.
Editor-in-Chief: Debra L. Zynger, M.D.


Last author update: 8 December 2022
Last staff update: 23 December 2022
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Thyroid fine needle aspiration

Table of Contents
Definition / general | Essential features | Terminology | CPT coding | Epidemiology | Sites | Diagrams / tables | Clinical features | Contraindications | Diagnosis | Radiology description | Radiology images | Case reports | Treatment | Benefits of ultrasound guided FNA compared to conventional FNA alone | Core biopsies | Set up | Needle based sample collection techniques | Sample preparation | Complications | Microscopic (histologic) description | Microscopic (histologic) images | Molecular / cytogenetics description | Molecular / cytogenetics images | Videos | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Jug R, Jiang X. FNA-general. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/thyroidFNA.html. Accessed April 18th, 2024.
Definition / general
- Minimally invasive technique to obtain cytologic specimens of thyroid nodules
- Recommended procedure when evaluating thyroid nodules for malignancy, to triage patients for possible surgery (Thyroid 2016;26:1)
- Can be performed using palpation guidance or ultrasound guidance
- Operators of thyroid fine needle aspiration (FNA) differ among countries and institutions: from clinicians (endocrinologist, head and neck surgeon) to radiologists and cytopathologists (J Pathol Transl Med 2017;51:571)
- Results are recommended to be reported in standardized format using the Bethesda System for Reporting Thyroid Cytopathology (see Bethesda categories)
- Sensitivity and specificity of FNA have been reported as high as 100% and 94%, respectively, if specimen is adequate; larger nodules have been reported to have higher false negative rate (PLoS One 2017;12:e0186242, BMC Res Notes 2008;1:12)
- Thyroid FNA was introduced in 1930 by Martin and Ellis, who used an 18 gauge needle aspiration technique; however, it became a mainstream approach much later, after introducing a so called small needle aspiration biopsy (now referred to as FNA) (Ann Surg 1930;92:169)
Essential features
- Superficial thyroid nodules may be targeted by palpation (if palpable) or with ultrasound guidance (nonpalpable or complex) with minimal complication
- Rapid on site evaluation (ROSE) may be performed to assess specimen adequacy
- Thyroid FNA is a highly accurate diagnostic procedure with few complications
- The Bethesda System for Reporting Thyroid Cytopathology is the recommended system to report results
Terminology
- Fine needle aspiration, thin needle aspiration, ultrasound guided fine needle aspiration (USG FNA) or palpation guided fine needle aspiration
- Fine needle aspiration cytology (FNAC), fine needle aspiration biopsy (FNAB)
CPT coding
- 10021 - fine needle aspiration
- 10022 - fine needle aspiration using imaging guidance
- 88112 - cytopathology, selective cellular enhancement technique with interpretation (e.g., liquid based slide preparation method), except cervical or vaginal (ThinPrep / SurePath technique)
- 88172 - cytohistologic evaluation of fine needle aspirate to determine adequacy for diagnosis
- 88173 - cytopathology, evaluation of fine needle aspirate; interpretation and report
- 88177 - cytohistologic evaluation of fine needle aspirate to determine adequacy for diagnosis (additional passes)
Epidemiology
- Thyroid nodules are common and are increasingly found incidentally
- Ultrasound identifies nodules in 19 - 68% of individuals selected at random (Thyroid 2016;26:1)
- More commonly found in women and the elderly
- Majority of thyroid nodules are benign (Thyroid 2016;26:1)
Sites
- In addition to presenting in the thyroid parenchyma, thyroid nodules may present as lymph nodes or other neck masses, as there can be ectopic thyroid or accessory thyroid nodules in thyroiditis
- Nodule location within thyroid gland should be confirmed by ultrasound to avoid unintentional biopsy of adjacent tissues (Diagn Cytopathol 2008;36:390)
Diagrams / tables
Contributed by Rachel Jug, M.B.B.Ch.
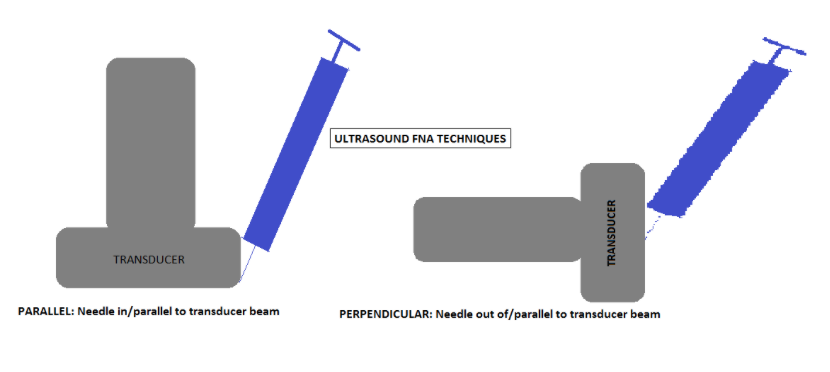
Ultrasound FNA techniques
Images hosted on other servers:

Risk based on appearance and nodule characteristics

Technique

Short, rapid strokes
with only slight
changes in direction
Clinical features
Indications (stratified by approach)
| Palpation guided | Ultrasound guided |
| Incidentally or radiographically identified predominantly solid (> 75%) thyroid nodule > 1 cm diameter confirmed by ultrasound | Complex and cystic nodules (> 25% cystic component); ultrasound helps target specific areas, such as solid areas (Diagn Cytopathol 2008;36:390) |
| Thyroid nodule of interest is discrete and palpable | Nonpalpable or difficult to palpate nodules (e.g., posteriorly located) (Diagn Cytopathol 2008;36:390) |
| When access to ultrasound guided FNA is limited, palpation guided FNA may be considered (Diagn Cytopathol 2008;36:390) | To aid skilled operator in ascertaining sample of specific nodule of interest and to avoid adjacent critical structures (Diagn Cytopathol 2008;36:390) |
| For repeat FNA, when a prior palpation guided FNA sample was insufficient (Diagn Cytopathol 2008;36:390) | |
| Follow up for patients, post partial or total thyroidectomy for malignancy, such as to sample thyroid bed (J Ultrasound Med 2013;32:1319) |
- 2015 American Thyroid Association (ATA) Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer (Thyroid 2016;26:1):
- Strongly recommends ultrasonic examination of thyroid nodules and cervical lymph nodes
- Recommended sampling if > 1 cm in greatest dimension and high suspicion sonographic pattern (estimates a 70 - 90% risk of malignancy), including solid hypoechoic nodule or nodule that is partially solid and hypoechoic and partially cystic with 1 or more of the following features:
- Irregular margins (infiltrative, microlobulated)
- Microcalcifications
- Oval (taller than wide) shape
- Rim calcifications with an extrusive soft tissue component
- Evidence of extrathyroidal extension
Contraindications
- Relative contraindications:
- Unable to lie recumbent
- Unable to control their rate and depth of respiration adequacy
- Severe anxiety (reassure variable anxiolytics)
- Young children (may require sedation)
- On heparin, warfarin, clopidogrel, high dose aspirin and other anticoagulants (Baskin: Thyroid Ultrasound and Ultrasound-Guided FNA, 2nd Edition, 2008)
- Variant anatomy due to previous illness or surgery
- Nodule of interest is hot on radionuclide thyroid scan
- Goiter (diffuse or asymmetric) precluding localization of nodule of interest (Diagn Cytopathol 2008;36:390)
- Absolute contraindication: severe coagulopathy disorder
Diagnosis
- Comparison of procedural ultrasound is made with diagnostic ultrasound to corroborate lesion of interest; findings on diagnostic ultrasound contribute to risk stratification of thyroid lesions in accordance with the 2015 ATA Management Guidelines (see Thyroid gland - Ultrasound) (Thyroid 2016;26:1)
- Diagnostic categories are assigned based on the Bethesda system for reporting thyroid cytopathology (Thyroid 2016;26:256)
Radiology description
Radiology images
Case reports
- 29 and 42 year old women with pneumothorax after thyroid FNA (Case Rep Otolaryngol 2021;2021:8944119)
- 30 year old woman with acute thyroid swelling after thyroid FNA (BMC Surg 2021;21:175)
- 56 year old man with acute thyroid swelling after thyroid FNA ( Diagn Cytopathol 2022;50:E193)
- 78 year old woman with a fatal hemorrhage after thyroid FNA (Am J Forensic Med Pathol 2022;43:291)
- 80 year old man with a massive hemorrhage after thyroid FNA (BMC Surg 2021;21:220)
Treatment
- Following the FNA procedure, ultrasound may be utilized to scan the neck for potential complications before they become apparent and prior to the patient leaving the clinic / hospital (AJSP 2018;23:165)
- Patient should be reminded of aftercare:
- Acetaminophen and icing may be used to relieve pain and swelling in accordance with medication directions on the packaging, if they do not have contraindications
- If bleeding is profuse or massive swelling occurs, patients should present to urgent care or emergency department for further evaluation
Benefits of ultrasound guided FNA compared to conventional FNA alone
- Ultrasound guided has higher adequacy and fewer false negative rates than palpation guided (J Clin Ultrasound 1994;22:535, Thyroid 1998;8:15, Thyroid 1998;8:283)
- Potentially lowers risk of damage to surrounding structures, which can be visualized
- Varying reports on cost effectiveness (BMC Endocr Disord 2009;9:14, Thyroid 2006;16:555)
- Efficacy of ultrasound guided FNA is improved by the presence of a cytopathologist on site, decreasing the overall inadequacy rate from 9.3% to 6% and improving adequacy rate and concordance with final diagnoses (Br J Radiol 2014;87:20130571, Cancer Cytopathol 2017;125:161)
- For additional details on thyroid ultrasound features and performance, see Thyroid gland - Ultrasound
Core biopsies
- Core biopsies are not the preferred initial procedure of choice in evaluation of a concerning thyroid nodule, as per ATA 2015 guidelines (Thyroid 2016;26:1)
- Core biopsies may be useful for fibrotic nodules that yield inadequate samples on repeat FNA or for collecting additional material for ancillary testing (Endocrinol Metab (Seoul) 2017;32:407)
- Korean Thyroid Association 2019 practice guidelines for thyroid core needle biopsy (J Pathol Transl Med 2020;54:64)
Set up
- Position patient supine with neck extended and pillow under shoulders
- Seated or semi-seated position used in some hospitals
- Examine the thyroid lobes and neck for thyroid masses and lymphadenopathy
- Assess the size of suspicious nodules identified; this is to help select FNA needle size and length to obtain an appropriate sample (Baskin: Thyroid Ultrasound and Ultrasound-Guided FNA, 2nd Edition, 2008)
Needle based sample collection techniques
- Determine how you want to hold the needle during the procedure; options include the French technique (open ended needle without suction with or without syringe attached without plunger), syringe pistol / gun, pencil grip syringe holder, vibrating holder (experimental) (Niger Postgrad Med J 2013;20:116, Diagn Cytopathol 1999;20:99, Laryngoscope 2021;131:E1393)
- Prior to aspiration with needle, use nondominant hand to stabilize the nodule and pull the skin taught between stabilizing fingers; clean the site with alcohol and let it dry prior to needle entry to prevent stinging
- Approach the skin at 45 degree angle with needle
- Local anesthetic with buffered lidocaine may be used but is not necessary (and adds an extra needle stick that may compromise cytology) since the majority of patients do not report pain after the procedure (J Emerg Med 1992;10:411, J Pain Res 2017;11:61)
- With aspiration / suction:
- 27 or 25G needle attached to a 10 cc syringe (with or without extension tubing), withdrawn so that 1 - 2 cc of negative pressure induces aspiration
- Without aspiration / nonsuction:
- 27 or 25G needle (with or without stylet, may attach open syringe) is introduced into nodule and capillary action causes uptake of cellular material into the needle
- Systematic review and meta analysis concluded superiority of thyroid FNA with smaller needle gauges (24 - 27G) and without aspiration (Thyroid 2018;28:857)
- May opt to use larger needle (22G) in severely calcified nodules to prevent bending of smaller needles within the lesion (Endocr J 2019;66:143)
- Use of a bare needle without a syringe or negative suction is termed the Zajdela technique, which capitalizes on the capillary action induced by forward motion of the needle in contrast to the application of suction (by syringe with or without a syringe holder)
- Regardless of the method, immobilization of the target while completing multiple rapid passes through the lesion in a fanning motion is required to adequately sample the lesion (Diagn Cytopathol 2008;36:407)
Sample preparation
- Sample preparation depends on the institution's preferred method
- Preparation methods include smears (air dried and alcohol fixed), liquid based preparations (ThinPrep, SurePath, etc.) and cell block
- For air dried slides, the Romanowsky staining method (using a stain such as Diff-Quik) is commonly used and alcohol fixed smears prevent drying artifacts and may be stained with the Papanicolaou stain
- For cases with rapid on site evaluation for adequacy, air dried slides can be used to evaluate material
- If the initial smear is of poor quality or insufficient to make a diagnosis, create another set of smears; otherwise, put the remainder of the sample into an ethanol based solution for ThinPrep processing (Papsociety.org: FNA Techniques [Accessed 8 June 2022])
- If a pathologist is not present to perform the FNA or to provide rapid on site evaluation, the institution may prefer to prepare exclusively Papanicolaou stained or ThinPrep slides
- Telecytology can be used for remote ROSE
- Additional material for ancillary tests, including biochemical (thyroglobulin washout, calcitonin, parathyroid hormone, etc.) and molecular testing (see Molecular testing in FNA) may be collected; for the latter, aspirated material is placed into nucleic acid preservative solution at the time of all initial thyroid biopsies or at the time of repeat sampling of an indeterminate nodule
- Tips:
- If samples are very bloody, consider placing excess blood / clot into a liquid based sample vial or making cell block, rather than making multiple bloody smears
- Follicular epithelium may get stuck in needle hubs; needle shield devices may be used to help flick excess material out of needle hub safely
Complications
- Hemorrhage (including local puncture site bleeding, ecchymosis, hematoma formation)
- Puncture site infection (Baskin: Thyroid Ultrasound and Ultrasound-Guided FNA, 2nd Edition, 2008)
- Damage to surrounding structures (e.g., potentially leading to dysphonia)
- Pain at puncture site (Nuklearmedizin 2018;57:211)
- Serious complications of FNA procedure are very rare (Clin Endocrinol (Oxf) 2009;71:157)
Microscopic (histologic) description
- Histopathological changes in thyroid after FNA procedure include acute and chronic:
- Acute changes are hemorrhage, granulation tissue, giant cells, hemosiderin laden macrophages, cholesterol clefts, necrosis, rarely infarction (Diagn Cytopathol 1996;15:211)
- Chronic changes are infarction, oncocytes, squamous or spindle metaplasia, fibrosis, calcification, vascular thrombosis; rarely tumor implantation along needle tract, rarely papillary endothelial hyperplasia (World J Surg 2020;44:378, Pathol Res Pract 2007;203:641, Arch Pathol Lab Med 1992;116:1040, Arch Pathol Lab Med 1991;115:240)
Microscopic (histologic) images
Contributed by Andrey Bychkov, M.D., Ph.D. and AFIP
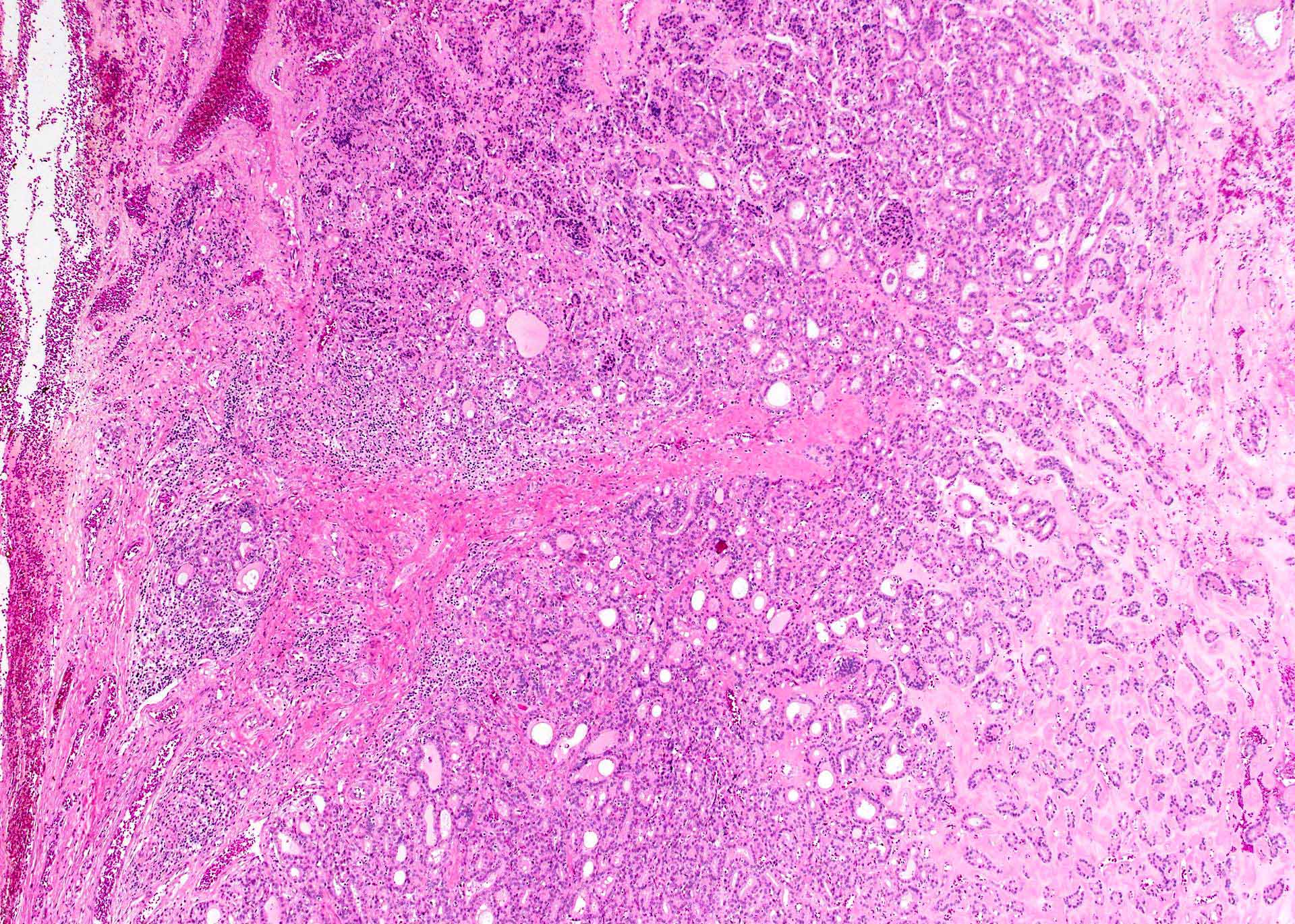
FNA induced alterations in thyroid nodule
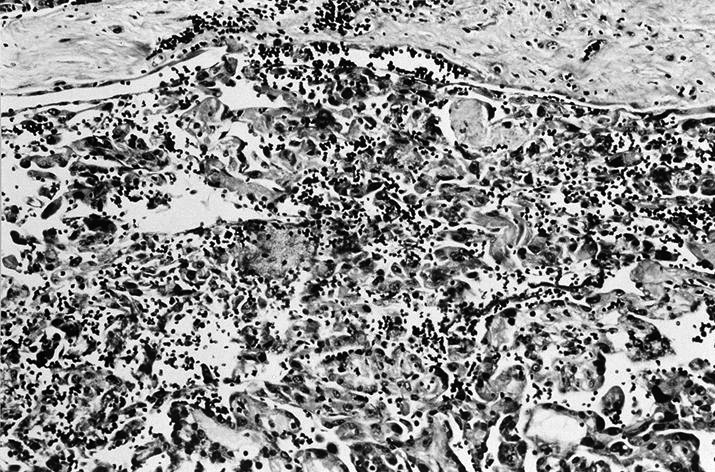
Pseudo angiosarcomatous pattern
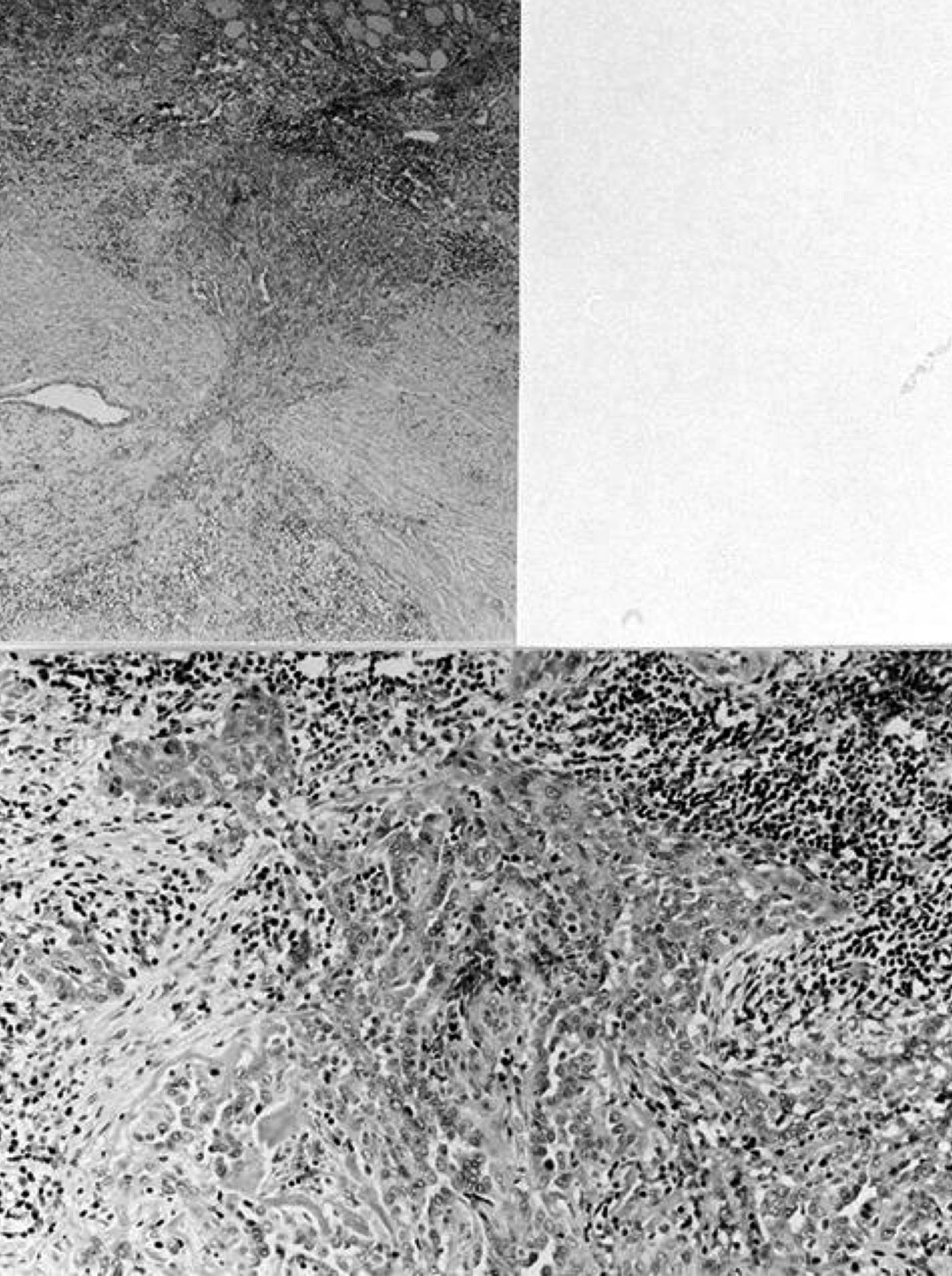
Fine needle
induced changes
in follicular
adenoma
Molecular / cytogenetics description
Molecular / cytogenetics images
Videos
FNA biopsy techniques
Thyroid FNA and smearing techniques
Superficial FNA technique
Additional references
- AJSP 2018;23:176, Baskin: Thyroid Ultrasound and Ultrasound-Guided FNA, 3rd Edition, 2013, Milas: Advanced Thyroid and Parathyroid Ultrasound, 1st Edition, 2017, Bardales: The Invasive Cytopathologist - Ultrasound Guided Fine-Needle Aspiration of Superficial Masses, 2014, Yang: Thyroid Fine Needle Aspiration, 1st Edition, 2013
Board review style question #1
What type of sample is evaluated during a rapid on site evaluation of a thyroid fine needle aspiration?
- Air dried stained slide
- Cell block material
- Core biopsy slide
- SurePath slide
- ThinPrep slide
Board review style answer #1
A. Air dried stained slide. Air dried slides are ideal for rapid on site evaluation.
Comment Here
Reference: FNA-general
Comment Here
Reference: FNA-general
Board review style question #2

Which of the following fine needle aspiration indications would favor using ultrasound guided rather than palpation guided fine needle aspiration?
- First biopsy of the specific lesion in question
- Patient referred specifically for fine needle aspiration with rapid on site evaluation
- Predominantly solid nodule
- Superficial thyroid nodule > 1 cm
- Thyroid nodule of interest in background of a multinodular goiter
Board review style answer #2
E. Thyroid nodule of interest in background of a multinodular goiter. Ultrasound guidance will assist in localizing fine needle aspiration to nodule of interest as opposed to off target nodules with benign radiographic features. Ultrasound guided fine needle aspiration allows for real time correlation to diagnostic ultrasound images.
Comment Here
Reference: FNA-general
Comment Here
Reference: FNA-general

