

Soft tissue
Fibroblastic / myofibroblastic
Nodular fasciitis
Author: Brendan C. Dickson, M.D., M.Sc.
Editorial Board Member: Jose G. Mantilla, M.D.
Deputy Editor-in-Chief: Borislav A. Alexiev, M.D.
Editor-in-Chief: Debra L. Zynger, M.D.

Last author update: 9 March 2023
Last staff update: 9 March 2023
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Nodular fasciitis
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Molecular / cytogenetics images | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Dickson BC. Nodular fasciitis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/softtissuenf.html. Accessed April 20th, 2024.
Definition / general
- Neoplasm of fibroblastic / myofibroblastic derivation that is typically benign and self limited
- Virtually all cases contain fusion genes; MYH9::USP6 is the most common fusion product, although other USP6 partners have been identified (Lab Invest 2011;91:1427, Mod Pathol 2017;30:1577)
Essential features
- Neoplasm of fibroblastic / myofibroblastic derivation that is typically benign and self limited
- Virtually all cases contain recurrent gene fusions; MYH9::USP6 is the most common fusion product, although many other USP6 partners have been identified in nodular fasciitis and related entities (e.g., cranial fasciitis, fibroma of tendon sheath, myositis ossificans, aneurysmal bone cyst) (Lab Invest 2011;91:1427, Mod Pathol 2017;30:1577, Virchows Arch 2021;479:147, Histol Histopathol 2022 Oct 7 [Epub ahead of print])
- Wide range of age involvement and anatomic distribution (Am J Clin Pathol 1961;35:122, Cancer 1982;49:1668, Pathology 1984;16:161, Ann Diagn Pathol 2015;19:180)
Terminology
- Pseudosarcomatous fasciitis (obsolete)
- Cranial fasciitis
ICD coding
- ICD-10: M72.4 - pseudosarcomatous fibromatosis
Epidemiology
- Relatively common mesenchymal neoplasm
- Predominates in young adults but can occur at virtually any age (Am J Clin Pathol 1961;35:122, Cancer 1982;49:1668, Pathology 1984;16:161, Ann Diagn Pathol 2015;19:180)
- No significant sex predilection
Sites
- Tumors arise throughout the body; common locations include the extremities, head and neck and trunk (Am J Clin Pathol 1961;35:122, Cancer 1982;49:1668, Pathology 1984;16:161, Ann Diagn Pathol 2015;19:180)
- May arise at unusual locations, such as intravascular, intra-articular, intraparotid, cranial and placental (Am J Surg Pathol 1981;5:29, Am J Surg Pathol 2006;30:237, Arch Pathol Lab Med 1989;113:1276, Head Neck Pathol 2020;14:257, Fetal Pediatr Pathol 2016;35:93)
- Most commonly originates in subcutis but may also arise in the dermis, fascia, skeletal muscle (Am J Clin Pathol 1961;35:122, Cancer 1982;49:1668, Pathology 1984;16:161, Ann Diagn Pathol 2015;19:180)
Pathophysiology
- Virtually all cases contain fusions genes; MYH9::USP6 is the most common fusion product, although many other genes may partner with USP6 (Mod Pathol 2017;30:1577)
Etiology
- Historically tumors were thought to result from trauma, although this is now considered unlikely
- Tumors appear to be sporadic and of unknown etiology
Clinical features
- Generally small (< 3 cm) but may be much larger (Am J Clin Pathol 1961;35:122, Cancer 1982;49:1668, Pathology 1984;16:161, Ann Diagn Pathol 2015;19:180)
- Rapid growth may be clinically concerning for malignancy (Am J Clin Pathol 1961;35:122)
- Mass may be tender, mildly painful or asymptomatic (Am J Clin Pathol 1961;35:122, Cancer 1982;49:1668, Pathology 1984;16:161, Ann Diagn Pathol 2015;19:180)
- Exceptionally these tumors may be morphologically or clinically malignant (Virchows Arch 2021;479:623, Int J Surg Pathol 2021;29:642, Virchows Arch 2021;479:1007, Genes Chromosomes Cancer 2016;55:640, Pathol Int 2019;69:706)
Diagnosis
- Tumors are morphologically distinctive and typically amenable to classification on the basis of H&E
- There is a limited role for immunohistochemistry as tumors show a myofibroblastic immunophenotype
- USP6 rearrangement can be confirmed by FISH, PCR or next generation sequencing
Radiology description
- Imaging findings, including MRI, are nonspecific and may be difficult to differentiate from sarcoma (Skeletal Radiol 2013;42:975)
Prognostic factors
- Not applicable; nodular fasciitis is considered benign
Case reports
- 22 month old boy with molecularly confirmed nodular fasciitis and atypical features (Virchows Arch 2021;479:623)
- 19 year old man with molecularly confirmed intravascular nodular fasciitis (Virchows Arch 2020;477:455)
- 30 and 56 year old women with molecularly confirmed nodular fasciitis arising intra-articularly (J Orthop Sci 2021;26:1138)
- 38 year old woman with molecularly confirmed nodular fasciitis of the orbit (Ophthalmic Plast Reconstr Surg 2017;33:S152)
- 48 year old woman with molecularly confirmed nodular fasciitis of the breast (BMJ Case Rep 2015;2015:bcr2015213076)
- 52 year old woman with molecularly confirmed nodular fasciitis of the vulva (APMIS 2016;124:534)
- 2 cases of molecularly confirmed nodular fasciitis of the placenta (Fetal Pediatr Pathol 2016;35:93)
Treatment
- Simple excision is generally curative
- Occasionally may spontaneously regress (e.g., following biopsy)
- Rarely recurs after incomplete excision
Clinical images
Images hosted on other servers:

Digital nerve
Gross description
- Solitary
- Typically < 3 cm but may grow up to 7 cm in rare cases (Ann Diagn Pathol 2015;19:180)
- Varies from soft to firm (Am J Clin Pathol 1961;35:122, Ann Diagn Pathol 2015;19:180)
- Peripheral margins may be circumscribed or infiltrative (Am J Clin Pathol 1961;35:122, Ann Diagn Pathol 2015;19:180)
- Color ranges from white to gray, tan and light pink; may have glistening cut surface (Am J Clin Pathol 1961;35:122, Ann Diagn Pathol 2015;19:180)
Gross images
Images hosted on other servers:

Breast
Microscopic (histologic) description
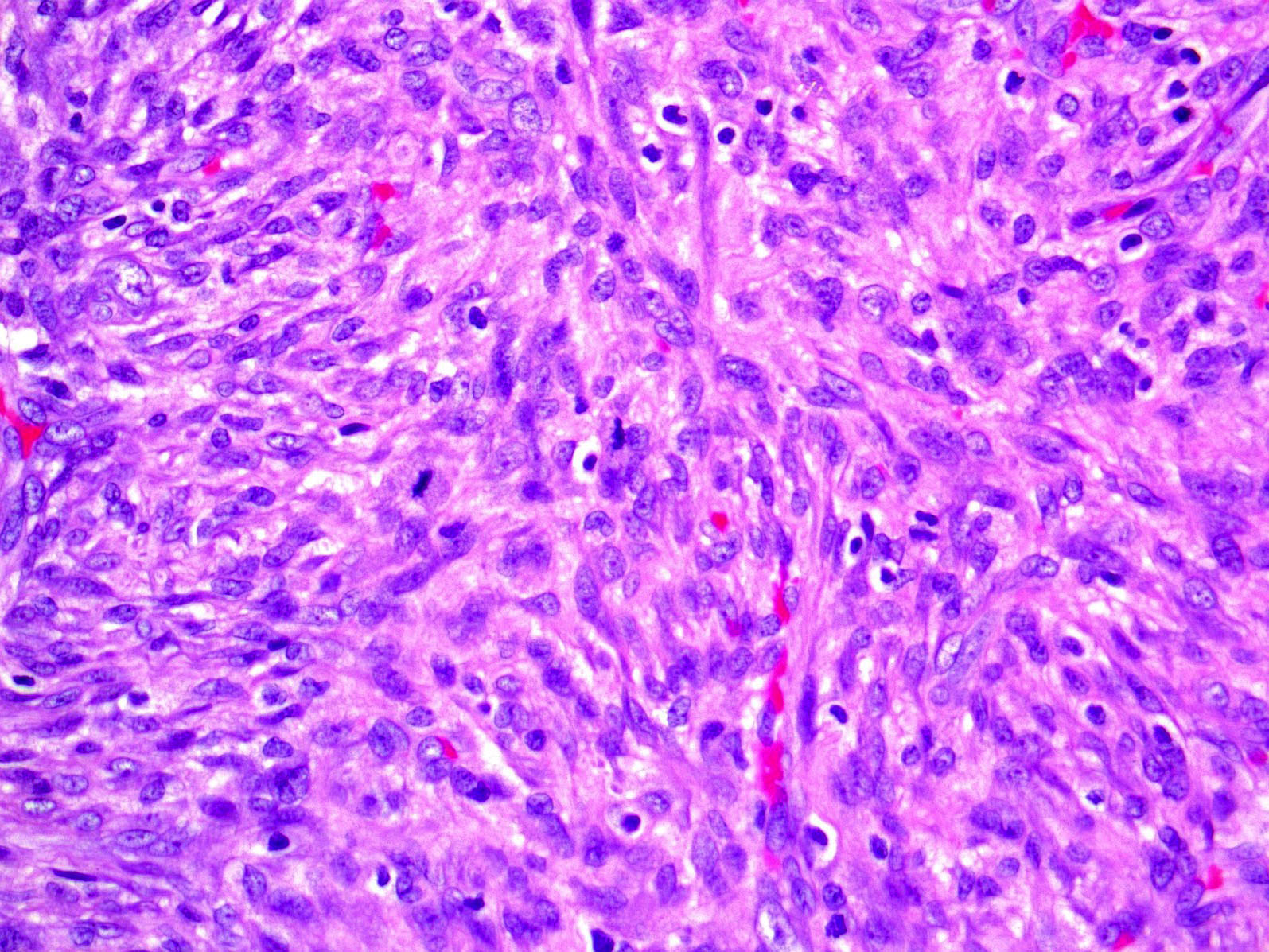
- Variable cellularity
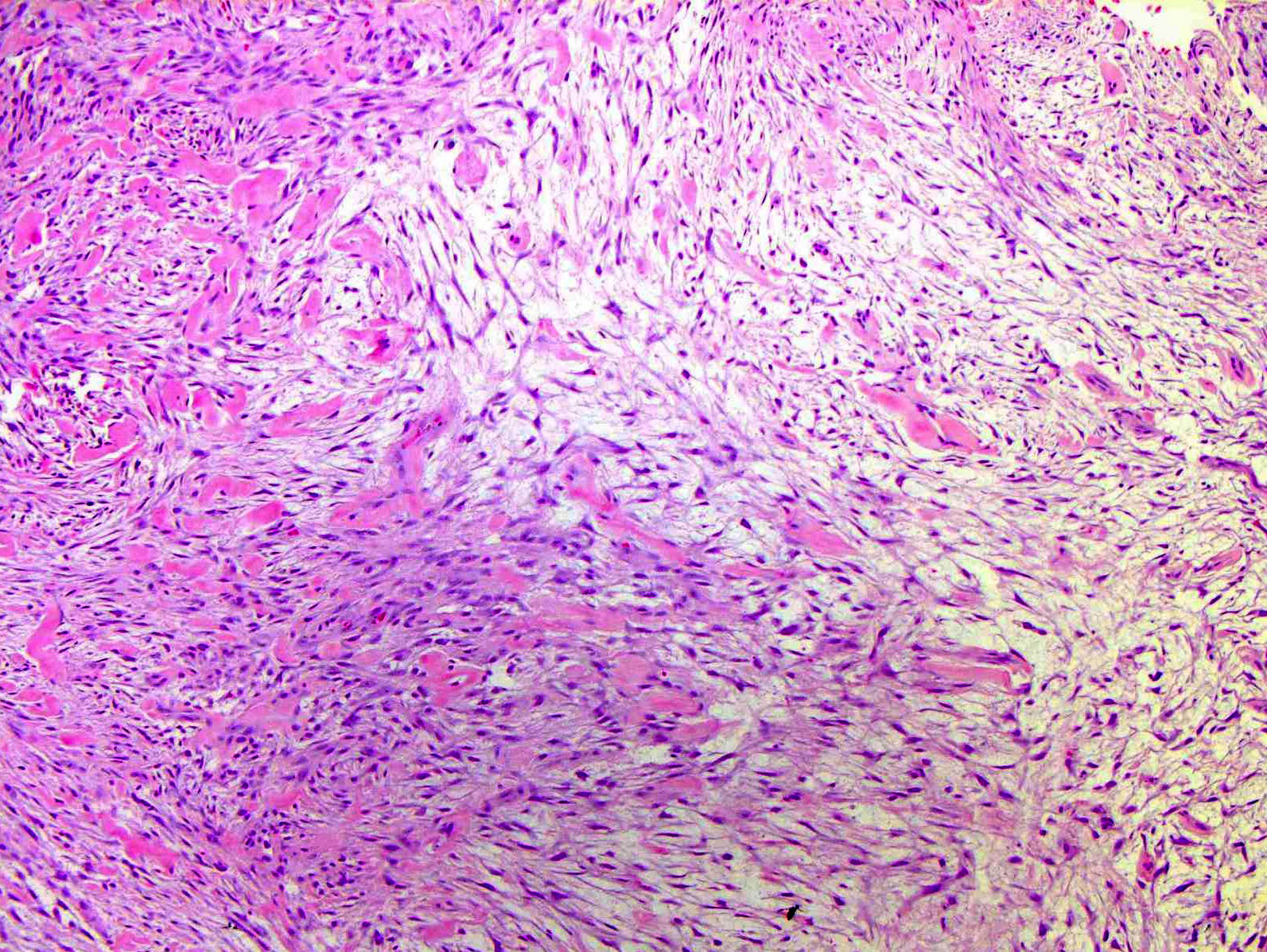
- Extracellular matrix ranges from myxoid to collagenous
- Older lesions may be more collagenous
- Areas of cystic degeneration may be identified
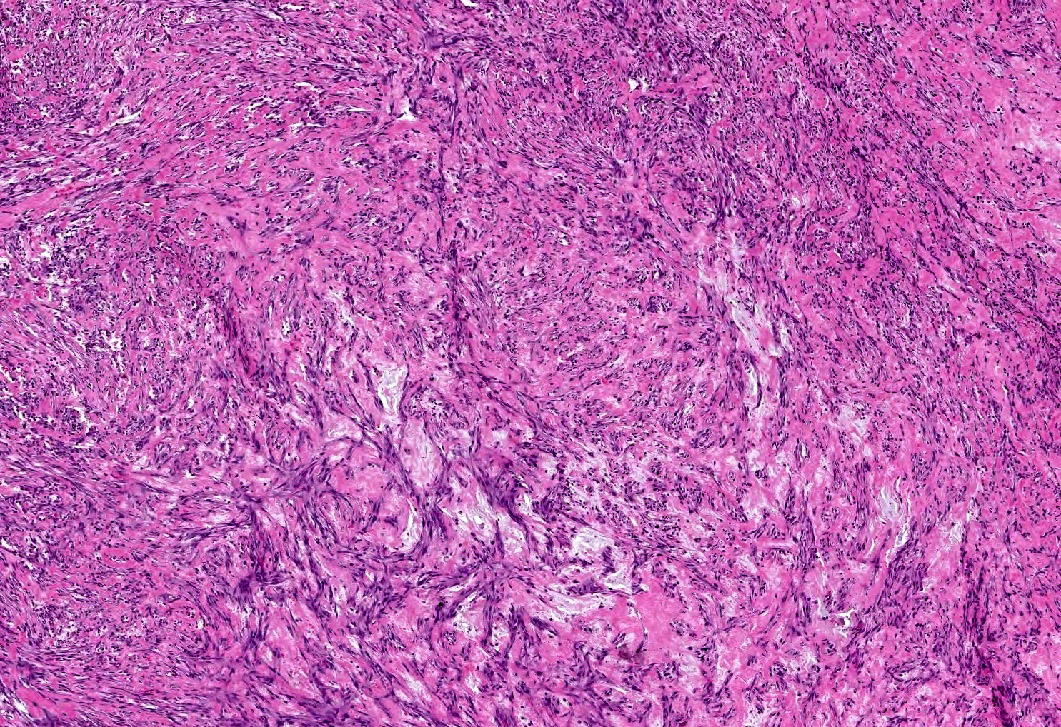
- Spindle stellate cells with a loose fascicular to storiform pattern (so called tissue culture-like and feathery growth)
- Bland ovoid nuclei
- Mitotic activity may be conspicuous; however, atypical figures are not a feature
- Scattered lymphocytes, histiocytes and osteoclast type giant cells often present
- Exceptionally rare tumors may have malignant morphologic features, including pleomorphism or atypical mitotic figures; in this context, a relationship with nodular fasciitis can only be made following molecular confirmation of USP5 rearrangement (Virchows Arch 2021;479:623, Int J Surg Pathol 2021;29:642, Virchows Arch 2021;479:1007)
Microscopic (histologic) images
Contributed by Brendan C. Dickson, M.D., M.Sc.
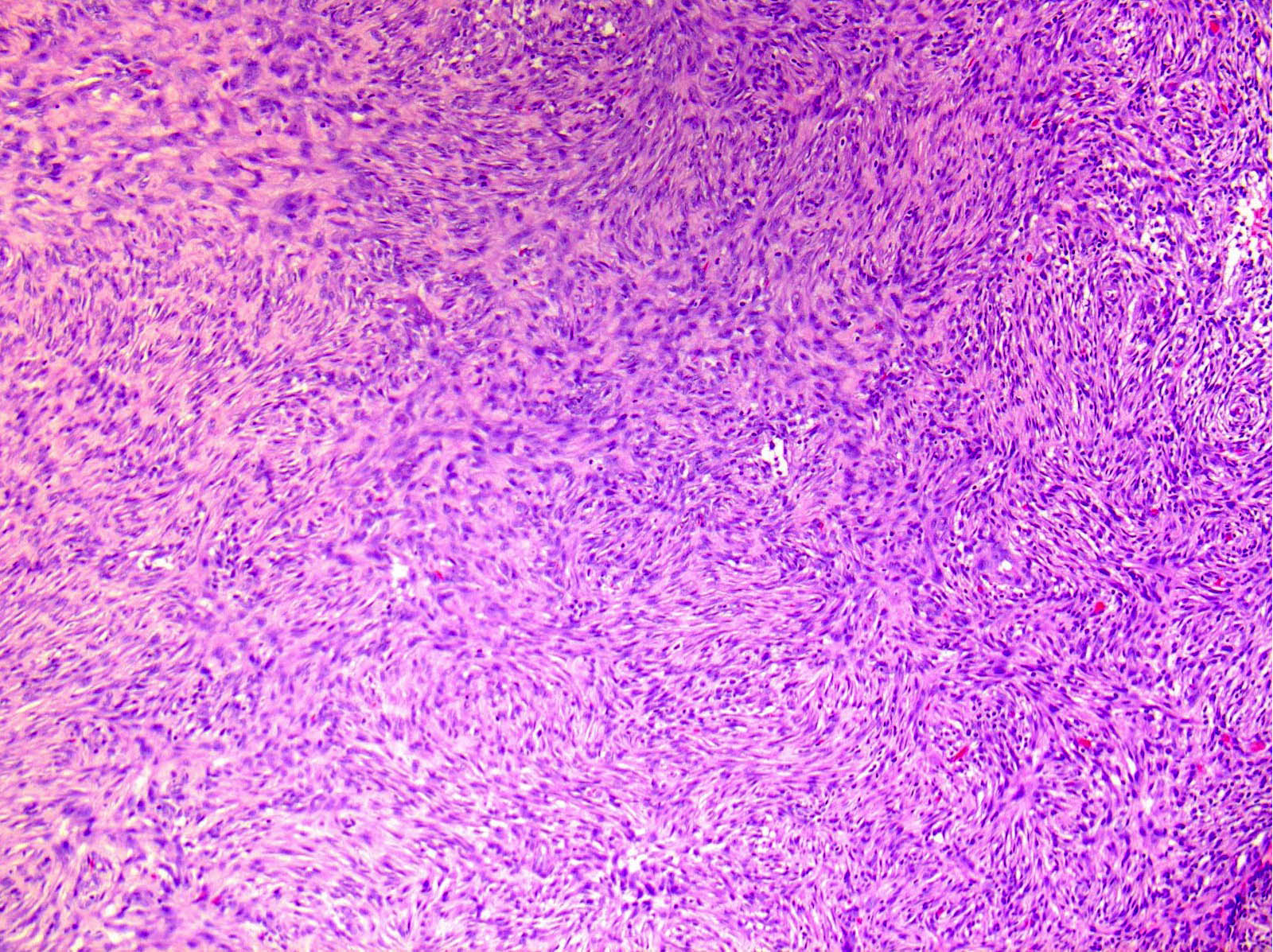
Cellular
Storiform
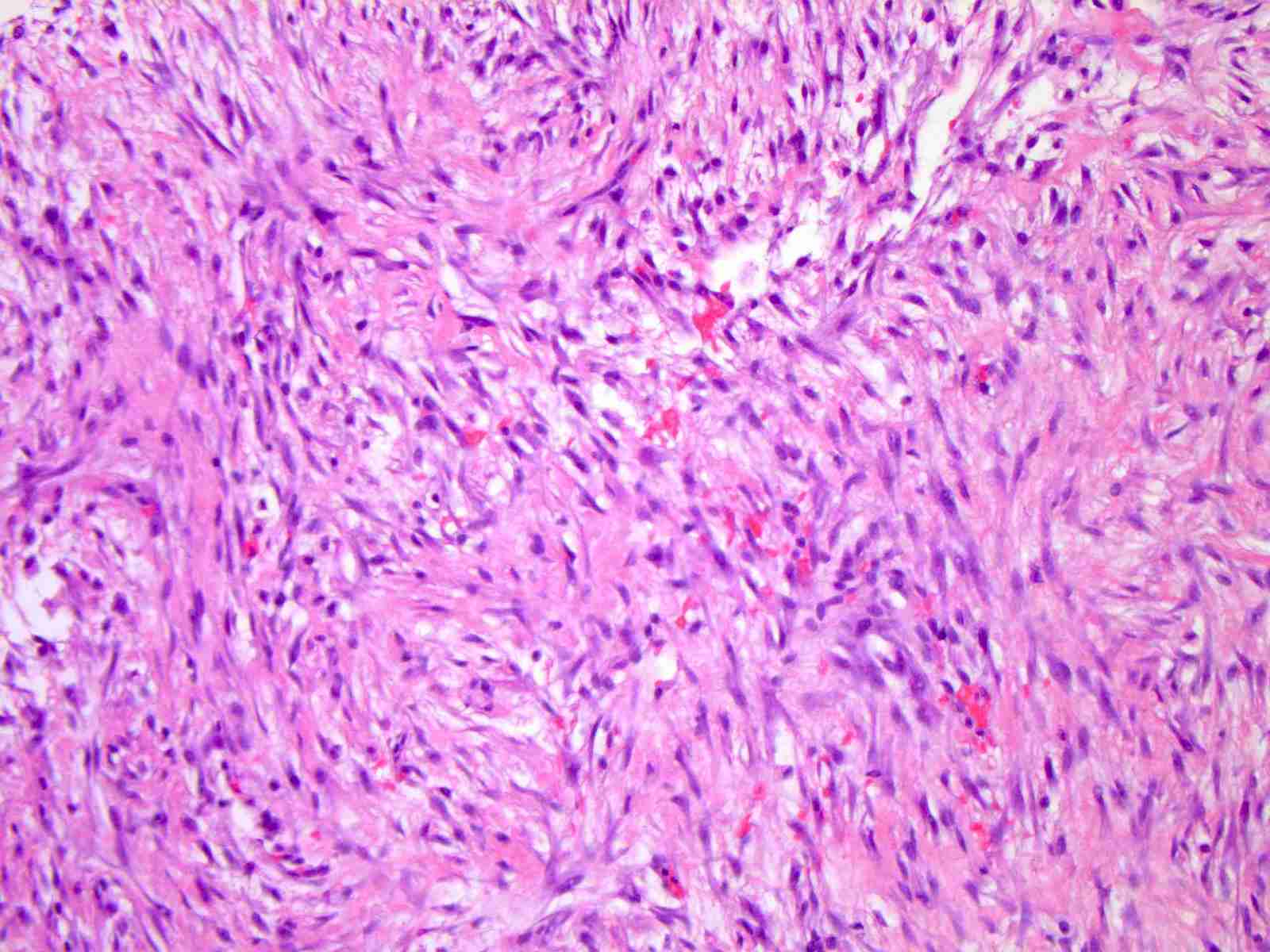
Myxoid
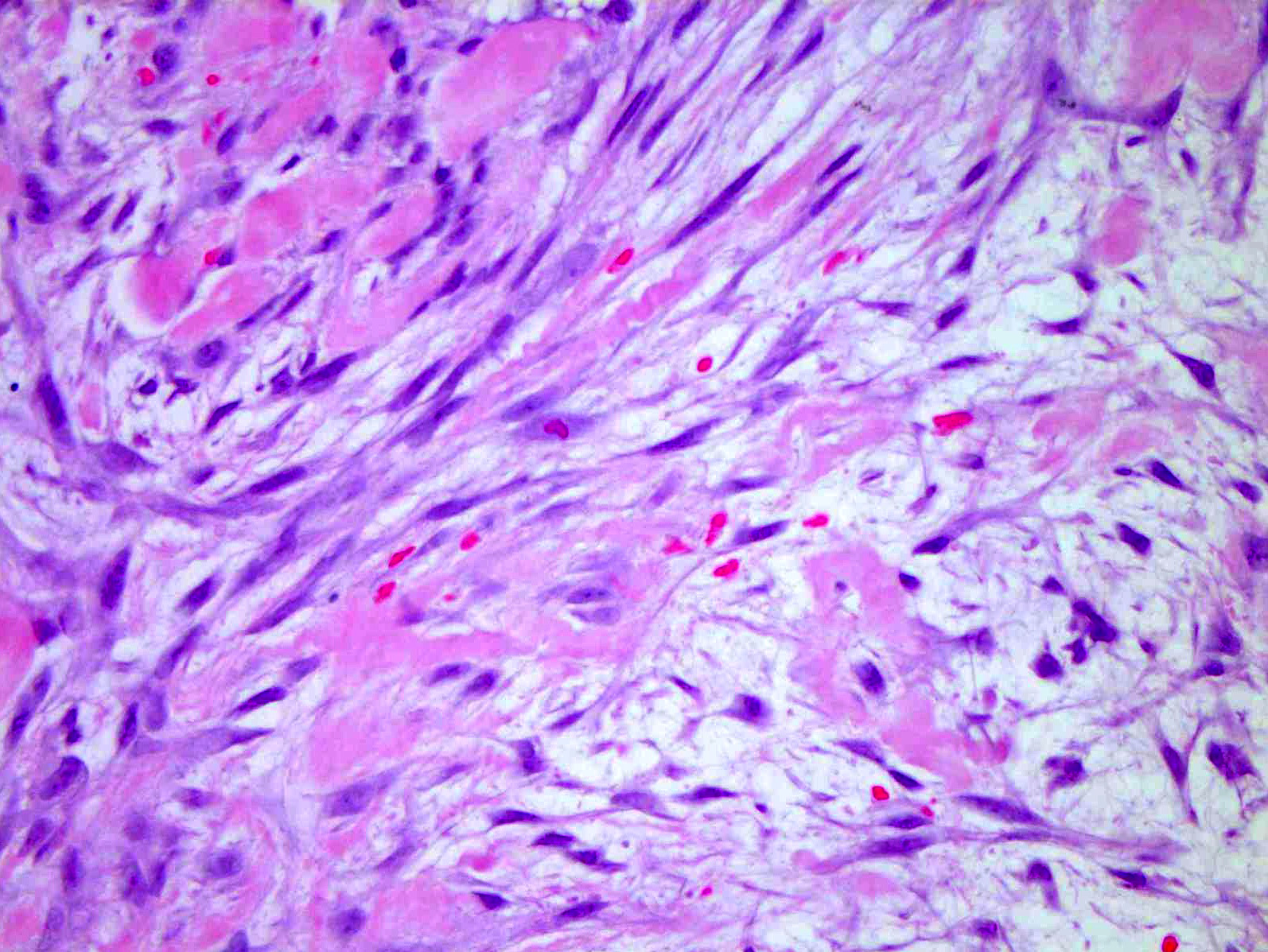
Extravasated erythrocytes
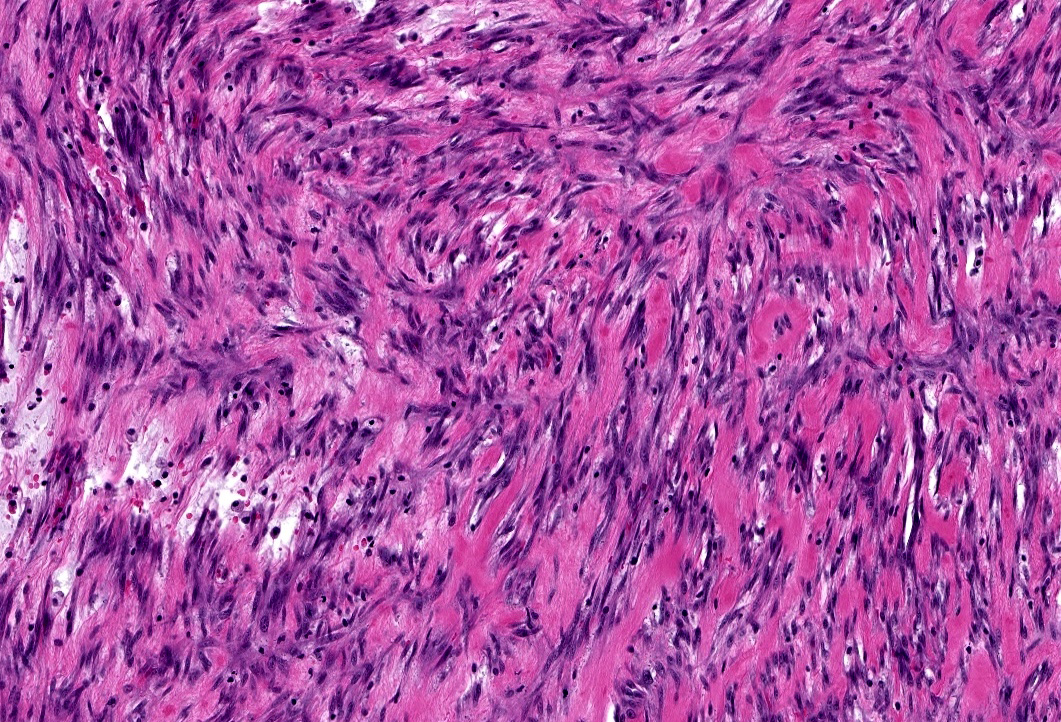
Collagenous
Positive stains
Negative stains
Electron microscopy description
- Ultrastructural features typical of fibroblasts; in addition, there are peripheral, longitudinal, myofilaments and hemidesmosome-like structures (Cancer 1976;38:2378)
Molecular / cytogenetics description
- Majority contain MYH9::USP6 fusion genes (Lab Invest 2011;91:1427)
- USP6 rearrangement can be established by FISH, PCR or next generation sequencing techniques
Molecular / cytogenetics images
Images hosted on other servers:

USP6 FISH
Sample pathology report
- Soft tissue, neck, biopsy:
- Nodular fasciitis (see comment)
- Comment: This is a spindle stellate cell neoplasm arranged in short bundles and fascicles. The nuclei are ovoid and monomorphic, with occasional mitotic activity. The stroma is variably myxoid to collagenous, with scattered lymphocytes and extravasated erythrocytes. The cells are positive for smooth muscle actin; they are negative for desmin, S100, CD34 and epithelial membrane antigen.
Differential diagnosis
- Dermatofibrosarcoma protuberans:
- Predominant storiform pattern
- Diffuse expression of CD34
- Desmoid type fibromatosis:
- Predominant fascicular pattern
- Expression of beta catenin
- Fibrous histiocytoma:
- Peripheral collagen entrapment
- Variable expression of factor XIIIa
- Mixed population including foamy macrophages
Additional references
Board review style question #1
Most cases of nodular fasciitis are characterized by which of the following gene fusions?
- ARL17A::USP6
- COL1A1::USP6
- MYH9::USP6
- PPP6R3::USP6
Board review style answer #1
Board review style question #2
Which of the following is generally true about the entity seen in the image above?
- Benign and self limiting
- Benign with frequent local recurrence
- Malignant and frequently metastasizing
- Malignant with frequent local recurrence
Board review style answer #2
