Skin nontumor
Lichenoid and interface reaction patterns
Chronic cutaneous lupus
Authors: Maryam Aghighi, M.D., Kiran Motaparthi, M.D.
Deputy Editor-in-Chief: Jonathan D. Ho, M.B.B.S., D.Sc.


Last author update: 3 January 2023
Last staff update: 3 January 2023
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Chronic cutaneous lupus
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Prognostic factors | Case reports | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Immunofluorescence description | Positive stains | Electron microscopy description | Sample pathology report | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Aghighi M, Motaparthi K. Chronic cutaneous lupus. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skinnontumorlupussle.html. Accessed October 1st, 2025.
Definition / general
- Lupus erythematosus is a multisystem autoimmune disease that involves the skin and internal organs
- Cutaneous lupus erythematosus is categorized as acute, subacute and chronic
Essential features
- Most common sites for discoid lupus erythematous are face, scalp and conchal bowl
- Discoid lupus erythematous presents with erythematous and scaly plaques with hyperpigmentation; scalp involvement may lead to scarring, dyspigmentation and alopecia
- Microscopic features of discoid lupus erythematous include epidermal atrophy, effacement of rete ridges, hyperparakeratosis, follicular keratotic plugging and basement membrane thickening with vacuolar interface change and keratinocyte apoptosis
Terminology
- Lupus erythematous (LE)
- Systemic lupus erythematous (SLE)
- Discoid lupus erythematous (DLE)
- Tumid lupus erythematosus
- Chilblain lupus erythematosus
- Lupus panniculitis
- Lupus profundus
ICD coding
- ICD-10: L93.0 - Discoid lupus erythematosus
Epidemiology
- Mostly young women between 20 and 30
- More common in persons of African descent than in Caucasians
Sites
- Discoid lupus erythematosus (DLE): face, scalp, conchal bowl
- Other variants of chronic cutaneous lupus erythematosus
- Tumid lupus erythematosus: upper trunk, lateral face
- Chilblain lupus erythematosus: acral
- Lupus panniculitis: upper extremities, upper trunk
Pathophysiology
- In patients with defects in innate immunity and opsonization, UV radiation causes apoptosis; subsequent phagocytosis leads to recognition of self antigens and autoimmunity
- Activated immune reaction is a result of interaction between hereditary predisposition and environmental or infectious agents
- MHC II may identify self antigens which show cross reactivity with pathogens
- HLA-B8, HLA-DR3, HLA-DR2, HLA-A1, HLA-B15, HLA-DRw6 are strongly associated with lupus (Arthritis Res Ther 2015;17:182)
Etiology
- Sun exposure (Int J Womens Dermatol 2019;5:320)
- Smoking is associated with discoid lupus erythematosus and tumid lupus erythematosus (Clin Cosmet Investig Dermatol 2019;12:707)
Clinical features
- Discoid lupus erythematosus: erythematous and scaly plaques with hyperpigmentation; scalp involvement often results in scarring, dyspigmentation and alopecia (Postepy Dermatol Alergol 2019;36:739)
- Tumid lupus erythematosus: erythematous plaques without scale or dyspigmentation
- Chilblain lupus erythematosus: violaceous patches or plaques incited or exacerbated by cold exposure
- Lupus panniculitis and profundus: tender subcutaneous nodules with or without epidermal or pigmentary changes
Diagnosis
- Clinical findings
- Blood draw
- Skin biopsy
Laboratory
- Localized discoid lupus erythematosus: 5% of cases associated with systemic lupus erythematosus (Int J Womens Dermatol 2017;3:S62)
- Generalized discoid lupus erythematosus: 30% of cases associated with systemic lupus erythematosus
- Tumid lupus erythematosus: rarely associated with systemic lupus erythematosus (J Clin Rheumatol 2008;14:338)
- In association with systemic disease: urinalysis, serum creatinine for renal disease, CBC / differential for anemia, leukopenia, lymphopenia, thrombocytopenia (Dtsch Arztebl Int 2015;112:423)
Prognostic factors
- Discoid lupus erythematosus is associated with low mortality but significant impact on quality of life due to dysesthesia, pruritus, scarring alopecia and dyspigmentation
- Early treatment helps to reduce scarring and atrophy (J Am Acad Dermatol 2011;64:849)
Case reports
- 19 year old man with lupus panniculitis (Medicine (Baltimore) 2016;95:e3429)
- 35 year old man with ankylosing spondylitis and discoid lupus erythematosus (North Clin Istanb 2019;6:412)
- 40 year old man with squamous cell carcinoma of the lower lip and discoid lupus erythematosus (Our Dermatol Online 2019;10:376)
- 54 year old woman with oral sarcoid granuloma associated with discoid lupus erythematosus (J Oral Diag 2017;02:e20170028)
- 57 year old African American woman with comedonal variant of chronic cutaneous lupus erythematosus (JAAD Case Rep 2019;5:801)
- 57 year old woman with sarcoidosis and chronic cutaneous lupus erythematosus (BMC Dermatol 2016;16:14)
Treatment
- Antimalarials such as hydroxychloroquine, immunosuppressants (including MTX, thalidomide) and topical steroids (Cochrane Database Syst Rev 2017;5:CD002954, Am J Clin Dermatol 2016;17:135)
- Direct sunlight avoidance
Clinical images
Contributed by Kiran Motaparthi, M.D.

Discoid lupus erythematosus, nose

Discoid lupus erythematosus, scalp and ear
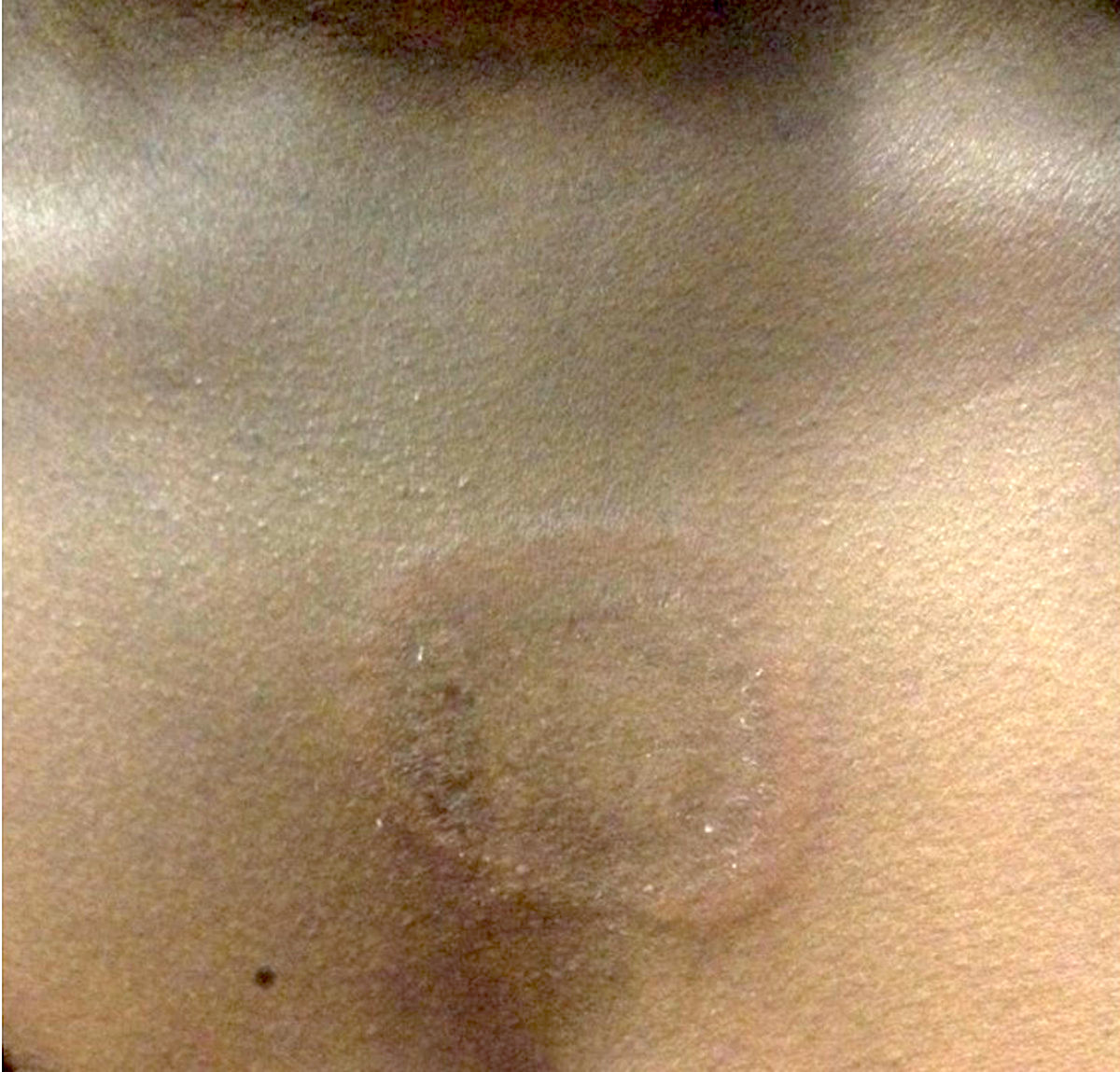
Tumid lupus erythematosus, chest


Chilblains lupus in patient with systemic lupus erythematosus

Lupus profundus
Images hosted on other servers:

Malar rash of face
Microscopic (histologic) description
- Discoid lupus erythematosus
- Epidermal atrophy or hypertrophy, attenuation (flattening) of rete ridges
- Hyperkeratosis and follicular keratotic plugging
- May have basement membrane thickening
- PAS highlighting the basement membrane zone
- Vacuolar degeneration with keratinocyte apoptosis in the basilar layer
- Cell poor infiltrate in the papillary dermis in most cases
- Lichenoid (band-like) infiltrate composed of lymphocytes in particularly hypertrophic cases
- Dilated blood vessels, edema and pigmentary incontinence in dermis
- Dense superficial and deep lymphocytic infiltrate around the adnexae and vessels
- Also increased plasma cells
- With or without increased mucin in dermis
- Pilosebaceous unit damage and broad zones of dermal fibrosis (Int J Womens Dermatol 2017;3:S62)
- Tumid lupus erythematous
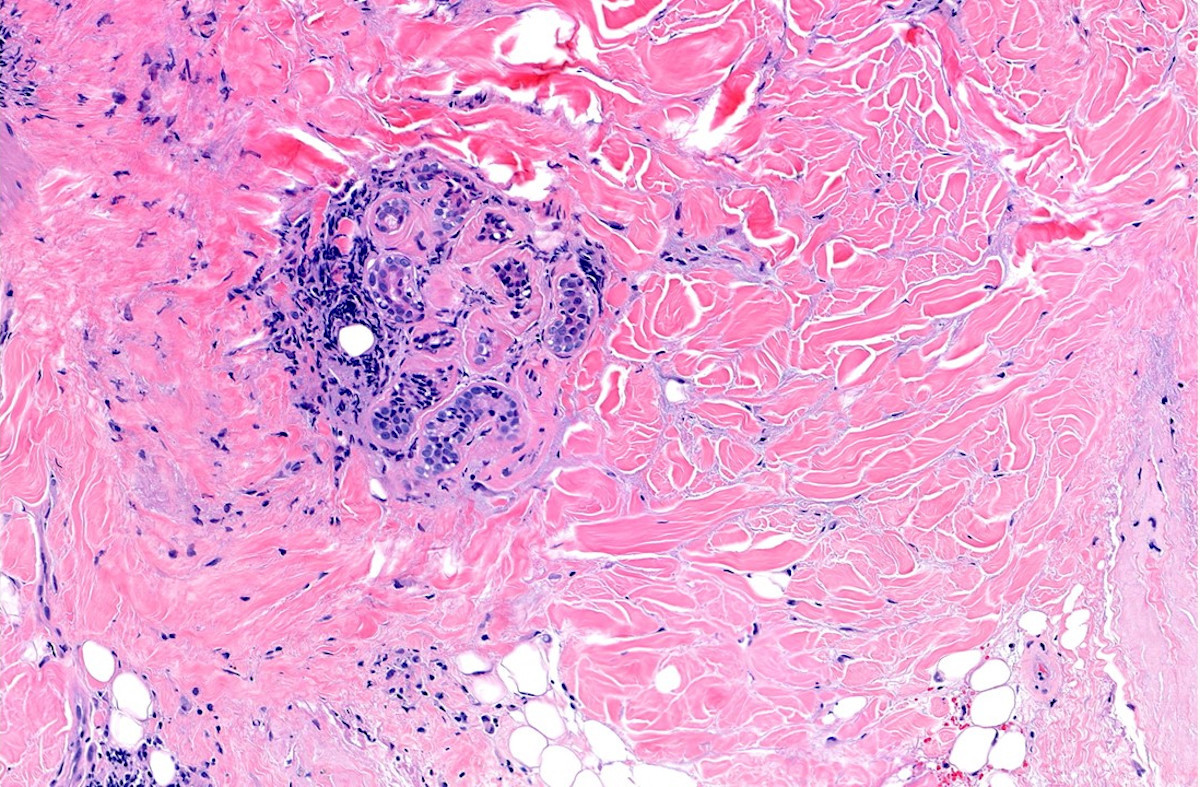
- Increased mucin in dermis
- Lymphocytic infiltrate in superficial and deep dermis, around the adnexae and vessels
- There is typically little to no involvement of the epidermis
- Chilblain lupus erythematosus
- Vacuolar interface change
- Papillary dermal edema
- Lymphocytic infiltrate in superficial and deep dermis and surrounding eccrine glands
- Variable vasculitic or vasculopathic changes (Br J Dermatol 2020;183:729)
- Lupus panniculitis and profundus
- Lupus profundus
- Hyperkeratosis and acanthosis
- Vacuolar interface change
- With or without increased mucin in dermis
- Lymphocytic infiltrate in superficial and deep dermis, around the adnexae and vessels
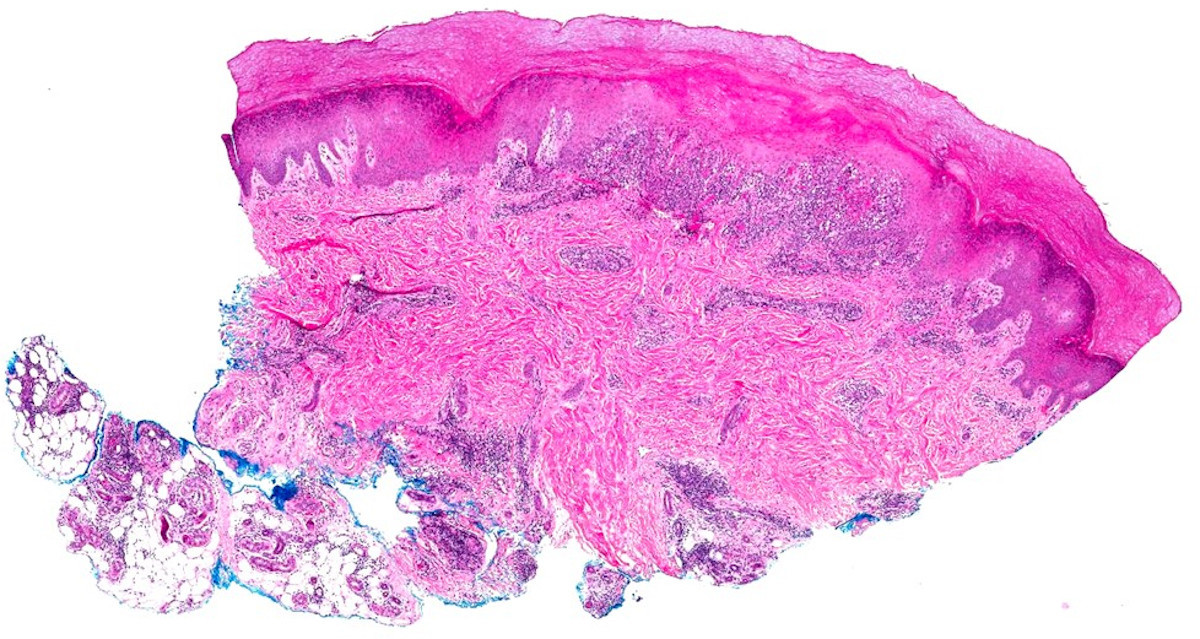
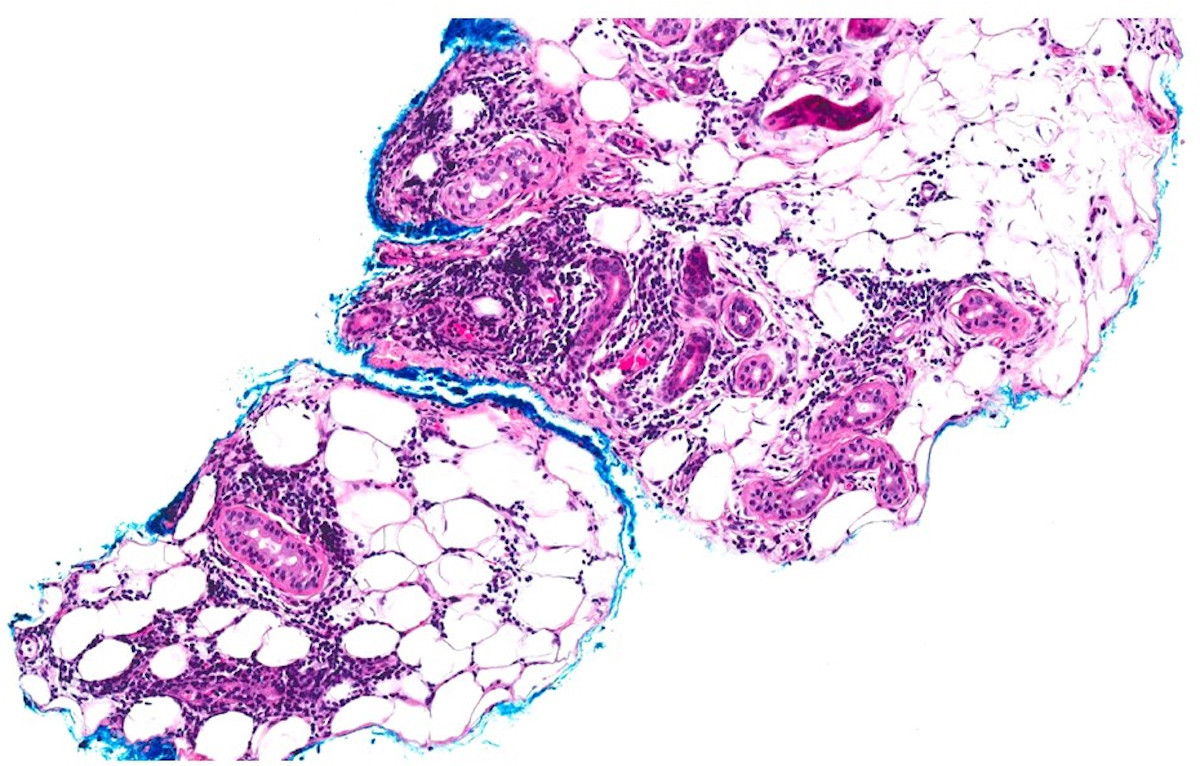
- Lupus panniculitis and profundus
- Lymphocytes, plasma cells, neutrophils with karyorrhectic debris and rare eosinophils in subcutaneous fat lobules and septa
- While typically lymphoplasmacytic, neutrophils and even rare eosinophils may be present
- Hyaline fat necrosis
- Lupus profundus
Microscopic (histologic) images
Contributed by Kiran Motaparthi, M.D.

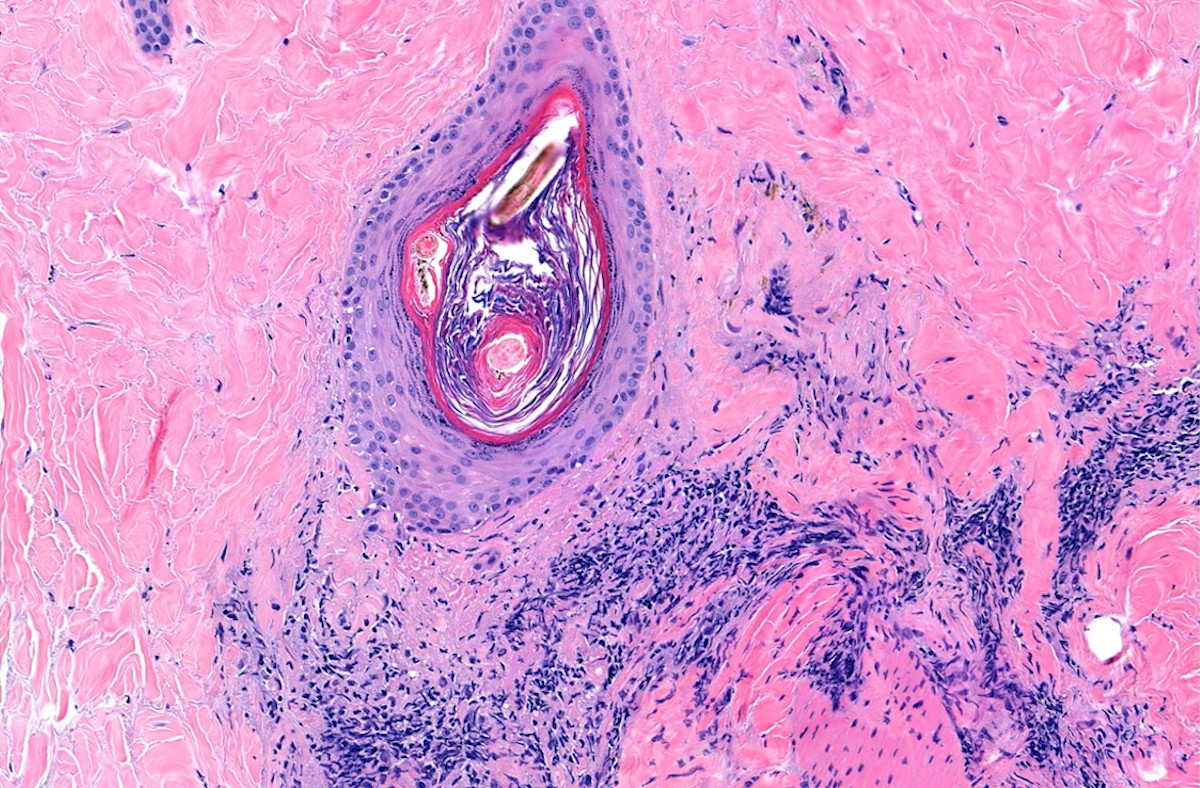
Discoid lupus erythematosus, late
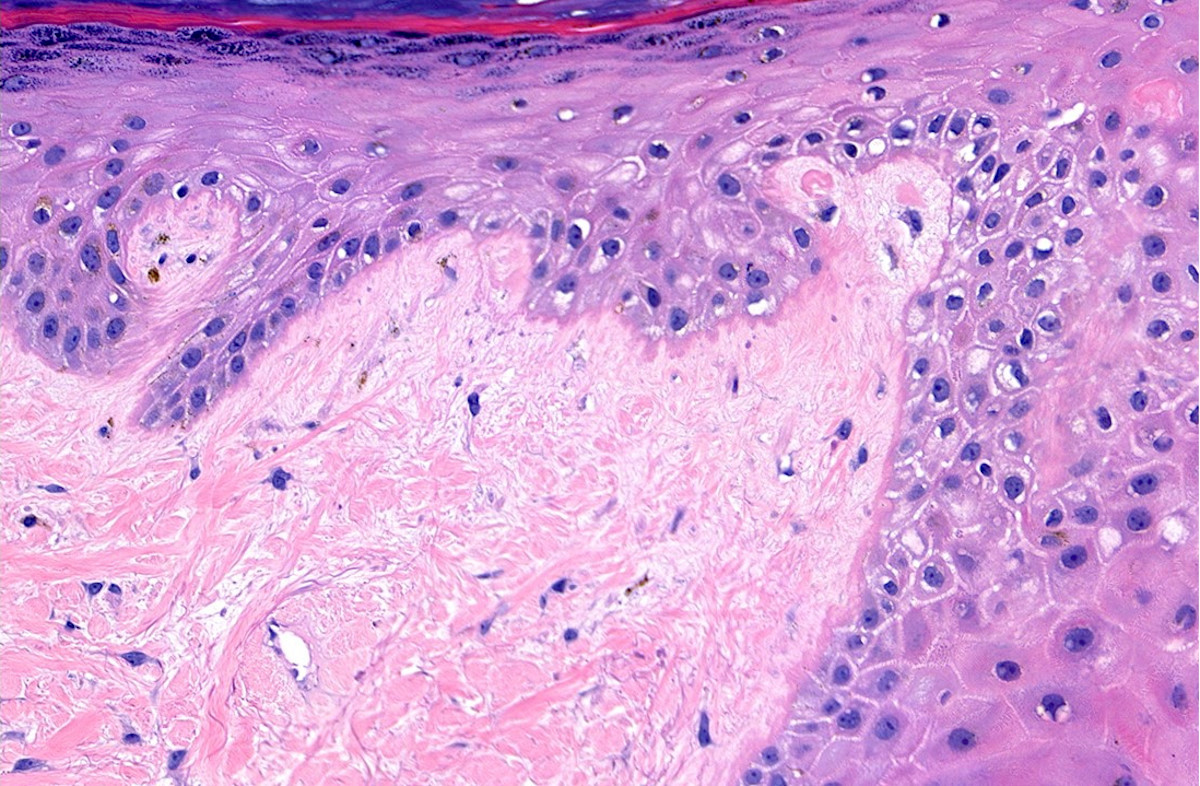
Discoid lupus erythematosus, late
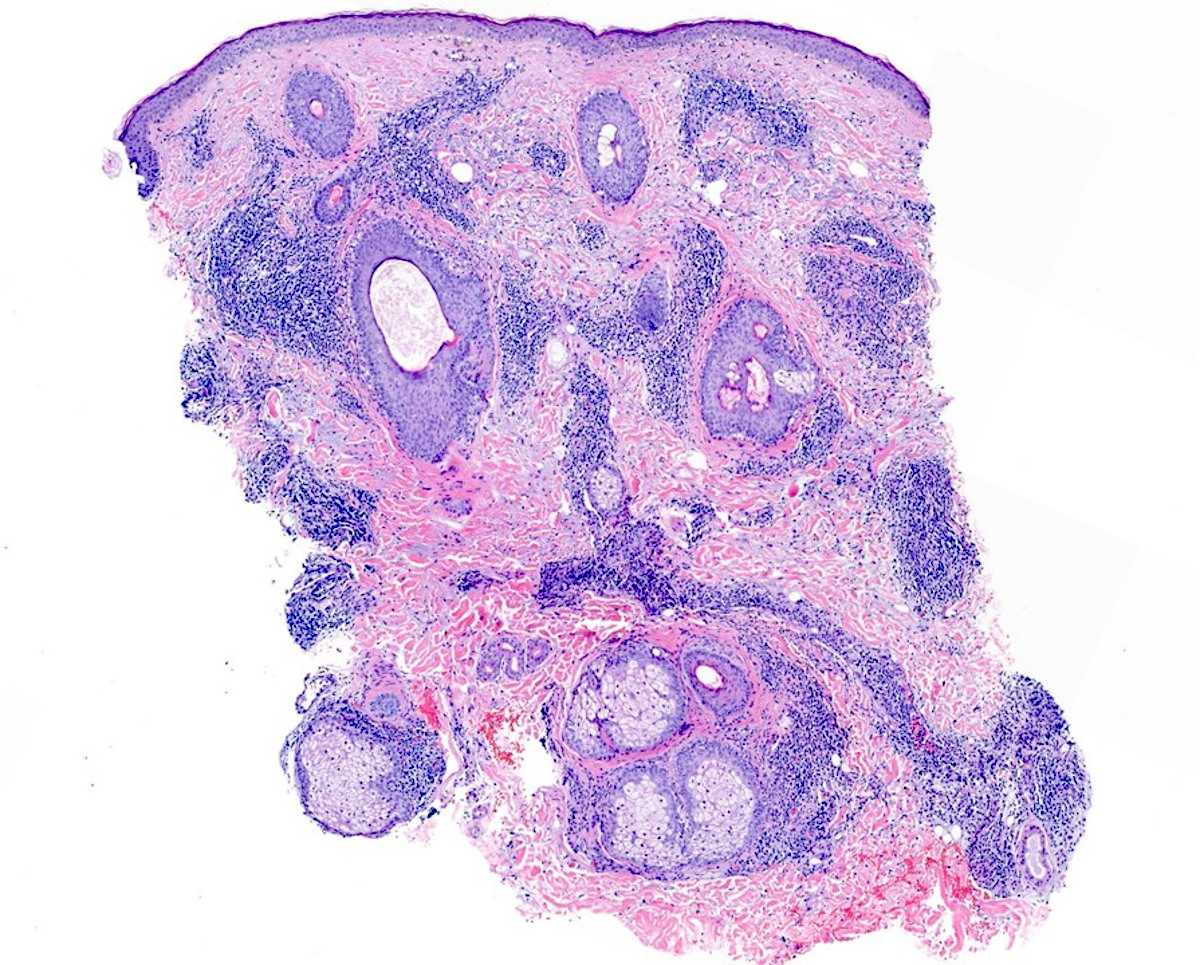
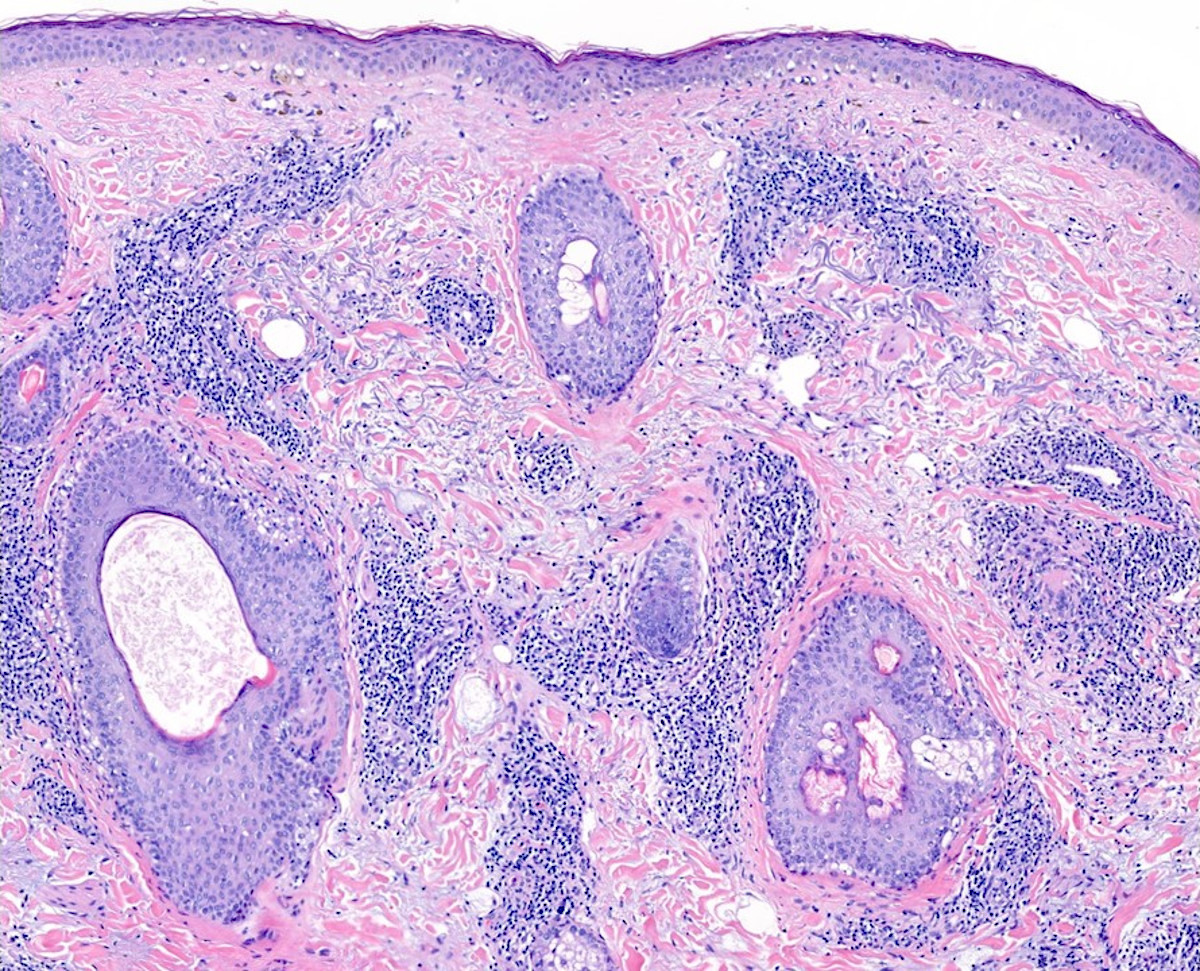

Tumid lupus erythematosus
Chilblains lupus

Chilblains lupus
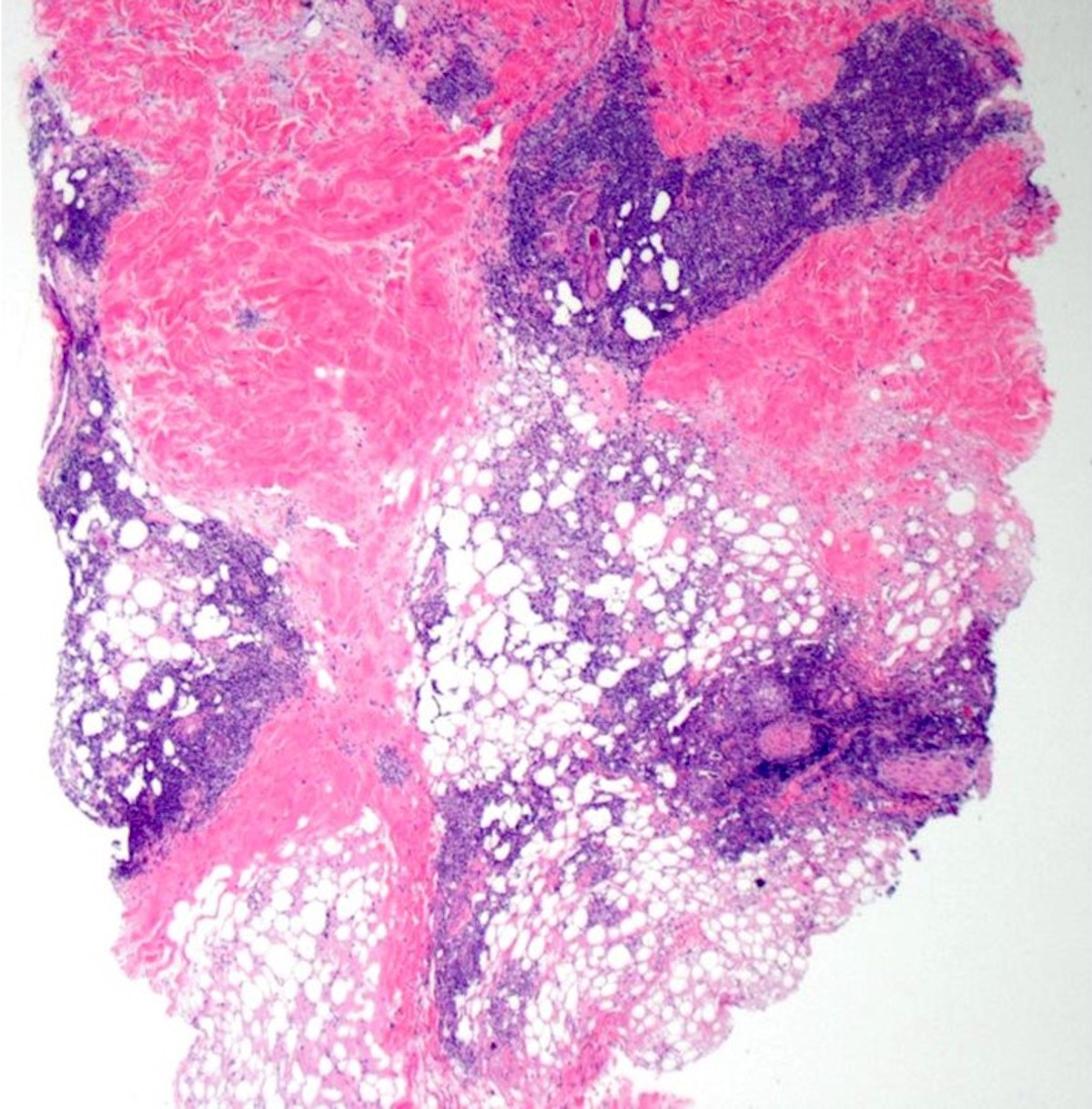

Lupus panniculitis
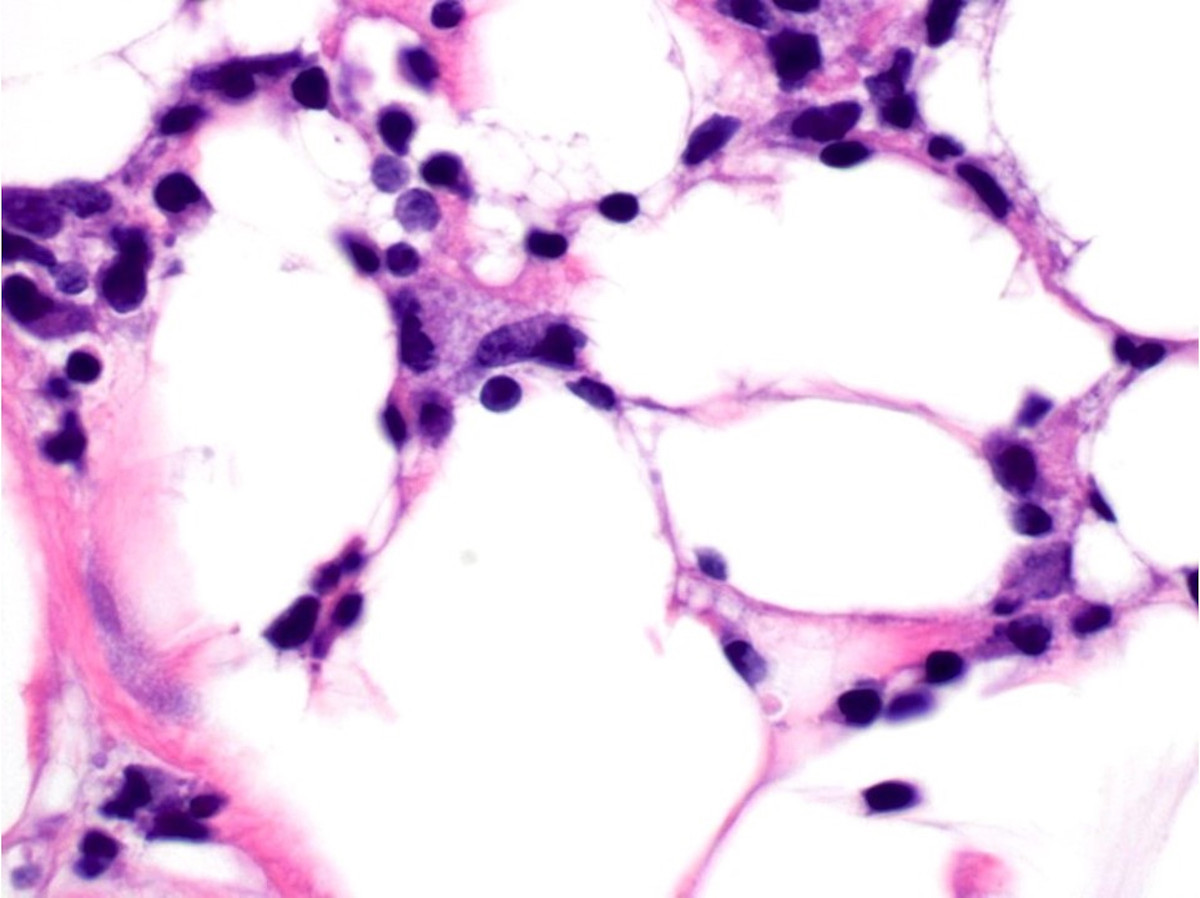
Lupus panniculitis
Virtual slides
Images hosted on other servers:

Discoid lupus erythematous

Lupus erythematosus profundus
Immunofluorescence description
- Positive lupus band test: IgM is most common, while IgG is most specific and C3 may also be paired with IgM (PLoS One 2013;8:e70983)
- Granular IgM is continuous in sun exposed skin and interrupted in sun protected skin
- In patients with systemic lupus, lupus band is identified in lesional and nonlesional skin, while in patients with cutaneous lupus but no systemic involvement, immunoreactant deposition is only identified in lesional skin
- However, a positive lupus band can be observed in sun exposed skin of healthy patients; specificity is increased in sun protected skin
- Possibility of in vivo antinuclear antibody in patients who have systemic lupus erythematosus (Ann Rheum Dis 1990;49:163)
- IgM also highlights cytoid bodies in cutaneous lupus erythematosus (J Cutan Pathol 2007;34:481)
Positive stains
- Alcian blue or colloidal iron highlights interstitial and periadnexal mucin deposition
- Periodic acid Schiff (PAS) and collagen IV highlight basement membrane thickening in discoid lupus erythematosus
- CD123 in discoid lupus erythematosus and chilblain lupus erythematosus (Int J Trichology 2020;12:62)
- Also useful in evaluating lupus panniculitis (Histopathology 2019;74:908)
- More CD123 positive plasmacytoid dendritic cells in dermis and fewer in epidermis of discoid lupus erythematosus compared with dermatomyositis (J Cutan Pathol 2008;35:452)
- CD123 fails to distinguish chilblain lupus erythematosus from idiopathic perniosis (Am J Dermatopathol 2018;40:265)
Electron microscopy description
- Subendothelial, subepithelial and mesangial deposits in discoid lupus erythematosus (Front Immunol 2016;7:647)
Sample pathology report
- Scalp, biopsy:
- Discoid lupus erythematosus (see comment)
- Comment: There is epidermal atrophy and follicular ostia are dilated and contain keratotic plugs. There is vacuolar degeneration in the basilar layer along with basement membrane thickening. There is a superficial and deep perivascular and periadnexal lymphocytic infiltrate with plasma cells. Dermal mucin is increased.
- Central chest, biopsy:
- Tumid lupus erythematosus (see comment)
- Comment: There is a superficial and deep perivascular and periadnexal lymphocytic infiltrate with plasma cells. Dermal mucin is increased.
- Shoulder, biopsy:
- Lupus profundus (see comment)
- Comment: There is epidermal hyperkeratosis and acanthosis. There is vacuolar degeneration in the basilar layer. Dermal mucin is increased. There is a superficial and deep perivascular, periadnexal and subcutaneous lymphocytic infiltrate with plasma cells. There is hyaline fat necrosis with karyorrhexis.
Differential diagnosis
- Discoid lupus erythematosus:
- Lymphocytic infiltrate of Jessner:
- Variant of tumid lupus erythematosus
- Erythematous annular plaques that heal without scarring or dyspigmentation
- Superficial and deep perivascular and periadnexal lymphocytic infiltrate with plasma cells
- Absence of epidermal changes and mucin in dermis is differentiating feature from discoid lupus erythematosus
- Lymphocytic infiltrate of Jessner:
- Lichen planus variants:
- Hypertrophic lichen planus:
- Violaceus, hyperkeratotic and lichenified plaques on extensor surfaces
- Parakeratosis, hypergranulosis and pseudoepitheliomatous hyperplasia
- Lichenoid interface dermatitis limited to base of rete ridges
- Differentiated from hypertrophic (verrucous) discoid lupus erythematosus by presence of eosinophils and absence of periadnexal and deep perivascular inflammation
- Lichen planopilaris:
- Perifollicular scale, erythema and scarring alopecia
- Lichenoid interface tissue reaction affects infundibulum and isthmus, with or without involvement of the epidermis
- Differentiated from discoid lupus erythematosus by absence of deep and perieccrine inflammation and mucin
- Lupus erythematosus and lichen planus overlap:
- Differentiated from discoid lupus erythematosus based on combination of histopathologic and immunopathologic features
- Epidermal changes typical of lichen planus along with deep and periadnexal inflammation
- Immunofluorescence findings of lupus erythematosus and lichen planus
- Hypertrophic lichen planus:
- Rosacea:
- Presents with erythematous papules and pustules and involvement of nasolabial folds
- No pigmentary changes, scarring or atrophy
- Lymphohistiocytic perifolliculitis, with variable perifollicular and intrafollicular neutrophils
- Lupus panniculitis:
- Subcutaneous panniculitis-like T cell lymphoma (SPTCL):
- Atypical T cells in subcutis which rim adipocytes
- Typically lacks plasma cells, eosinophils or neutrophils
- Bean bag cells: histiocytes which demonstrate erythrophagocytosis and cytophagocytosis
- Monoclonal T cell receptor gene rearrangement
- Positive for CD8, TCR beta F1 and cytotoxic markers
- Negative for CD4, TCR delta, CD56 and EBER
- Subcutaneous panniculitis-like T cell lymphoma (SPTCL):
- Chilblain lupus erythematosus:
- Perniosis:
- Painful erythematous or edematous nodules on acral skin following exposure to cold
- Clinical context variable: chronic cutaneous lupus erythematosus (CCLE) without systemic disease, chilblain lupus erythematosus in the context of systemic lupus erythematosus, idiopathic perniosis and COVID-19
- Vacuolar interface change is common
- Marked subepidermal edema
- Superficial and deep perivascular and perieccrine lymphocytic infiltrate
- Vasculitis variable
- Interstitial fibrin and increased mucin favor chilblain lupus erythematosus over idiopathic perniosis (Am J Dermatopathol 2018;40:265)
- Perniosis:
- Tumid lupus erythematosus:
- Polymorphous light eruption:
- Pruritic papules, vesicles and plaques with photodistribution
- Marked papillary dermal edema
- Superficial and deep perivascular lymphocytic infiltrate
- Distinguished from tumid lupus by marked edema, absence of mucin and lack of significant periadnexal inflammation
- Polymorphous light eruption:
Additional references
Practice question #1
A 37 year old woman presents with erythematous plaques without dyspigmentation or scale on her upper trunk. The biopsy demonstrates a perivascular and periadnexal lymphocytic infiltrate without epidermal changes. Which of the following statements is correct?
- Edema is typically prominent
- The histopathologic findings include prominent keratinocyte necrosis in the basal layer of the epidermis and follicular epithelium
- These findings represent polymorphous light eruption
- These findings represent tumid lupus erythematous
- This condition is strongly associated with systemic lupus erythematosus
Practice answer #1
D. The cutaneous findings represent tumid lupus erythematosus
Comment Here
Reference: Chronic cutaneous lupus
Comment Here
Reference: Chronic cutaneous lupus
Practice question #2
A 32 year old woman presents with hyperpigmented plaques on the conchal bowl and a scarring alopecia. Skin biopsy revealed an atrophic epidermis, basement membrane thickening with vacuolar interface change and increased mucin in dermis. There is a superficial and deep and perieccrine lymphocytic infiltrate. Which of the following is the best diagnosis?
- Discoid lupus erythematosus
- Lichen planopilaris
- Lymphocytic Infiltrate of Jessner
- Polymorphous light eruption
- Rosacea
Practice answer #2
