Skin nonmelanocytic tumor
Adnexal tumors
Sweat gland derived (apocrine & eccrine glands)
Syringoma
Authors: Aadil Ahmed, M.D., Bernadette M. Boac, M.D., Nicole D. Riddle, M.D., Sara C. Shalin, M.D., Ph.D.
Resident / Fellow Advisory Board: Caroline I. Mullins, M.D.
Editorial Board Member: Debra L. Zynger, M.D.


Last author update: 28 September 2021
Last staff update: 14 April 2023
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Syringoma skin[title] pathology
Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Ahmed A, Shalin SC. Syringoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skintumornonmelanocyticsyringoma.html. Accessed September 16th, 2025.
Definition / general
- Benign adnexal neoplasm of sweat gland (eccrine) origin
- Most common clinical presentation on lower eyelids of women
- Appears to derive from sweat duct ridge
- Malignant counterpart can be termed syringomatous carcinoma / sweat gland carcinoma
Essential features
- Often multiple 1 - 4 mm, firm papules
- Well circumscribed dermal lesion with comma shaped ductules lined by basaloid cells and with sclerotic stroma
ICD coding
- ICD-10: D23.9 - other benign neoplasm of skin, unspecified
Epidemiology
- F > M for all syringomas (J Am Acad Dermatol 2016;74:1234)
- Due to the asymptomatic nature of vulvar syringoma, it is believed to be underreported (Dermatology 1996;192:62)
- Typically occurs after puberty; most common during reproductive years (may be due to hormonal influence)
- More common in people of Asian decent
- Increased incidence in Japanese women and these syndromes:
- Down (J Am Acad Dermatol 1987;16:310)
- Ehlers-Danlos
- Marfan (J Low Genit Tract Dis 2016;20:e55)
- Nicoloau-Balus
- Brook-Spiegler
- Possible familial association (up to 20%)
Sites
- Dependent on clinical variant (for example, localized versus eruptive) (J Am Acad Dermatol 2016;74:1234)
- Localized variant: periorbital > vulvar / penile > scalp > axillary > facial > forearm / hand (J Am Acad Dermatol 2016;74:1234)
- Eruptive variant: anterior trunk > neck > axillae (Indian J Dermatol 2013;58:326)
- Most common site < 15 years old: neck and anterior trunk (Indian J Dermatol 2013;58:326)
Pathophysiology
- Represents adenoma of acrosyringium, the intraepidermal eccrine sweat duct (Arch Dermatol 1967;96:500)
- Poorly understood at this time (J Am Acad Dermatol 2016;74:1234)
Etiology
- Uncertain, possible hormonal influence (Dermatol Online J 2017;23:1)
- Clear cell variant has an association with diabetes (Am J Dermatopathol 1984;6:131)
Clinical features
- Generally asymptomatic but often presents with pruritus (J Am Acad Dermatol 2003;48:735)
- Multiple, small 1 - 4 mm, firm, flesh colored lesions (Dermatol Online J 2017;23:1)
- Typically bilateral and symmetric (J Low Genit Tract Dis 2016;20:e55)
- Exacerbation of pruritus during menstruation and summer months (J Am Acad Dermatol 2003;48:735)
- Oral contraceptive pills and pregnancy may also worsen symptoms (Invest Clin 2015;56:60)
- Concomitant extragenital lesions are common (J Am Acad Dermatol 2003;48:735)
- Clinical variants (J Am Acad Dermatol 1987;16:310):
- Localized
- Generalized
- Multifocal
- Eruptive
- Down syndrome
- Familial
Diagnosis
- On face, in particular, can be clinically suspected
- Biopsy required for confirmation
Prognostic factors
- Benign, nonprogressive lesions but can be cosmetically bothersome if multiple
- Recurrence, scarring and dyspigmentation after treatment
Case reports
- 19 year old woman with numerous asymptomatic papules on vulva (Int J Gynaecol Obstet 2007;99:65)
- 24 year old woman with vulvar syringoma exacerbated during pregnancy (Pathol Oncol Res 2003;9:196)
- 35 year old woman with a 20 year history of vulvar lesions (Acta Neurol Scand 1990;82:109)
- 44 year old woman with asymptomatic vulvar lesions (Dermatol Online J 2018;24:1)
- 46 year old woman with 2 year history of vulvar papules associated with vulvar itching and burning (J Clin Diagn Res 2014;8:FD06)
- 3 women clinically diagnosed with genital warts, mimicking uncommon conditions, including syringoma (Iran J Public Health 2019;48:1161)
Treatment
- Treatment necessary only for cosmetic reasons or quality of life
- Excision or cryotherapy / laser therapy is most common
- Does not respond to topical steroids
- Microinsulated needle radiofrequency for better cosmetic results (Dermatol Ther 2019;32:e12912)
- Carbon dioxide laser ablation may leave a scar and hyperpigmentation (Dermatol Ther 2019;32:e12912)
- Topical atropine to alleviate pruritus and reduce size of lesion (J Am Acad Dermatol 2003;48:735)
- Reference: Calonje: McKee's Pathology of the Skin, 5th Edition, 2019
Clinical images





Gross description
- 1 - 4 mm, firm, skin colored papule with or without eruption
Gross images
- See Clinical images
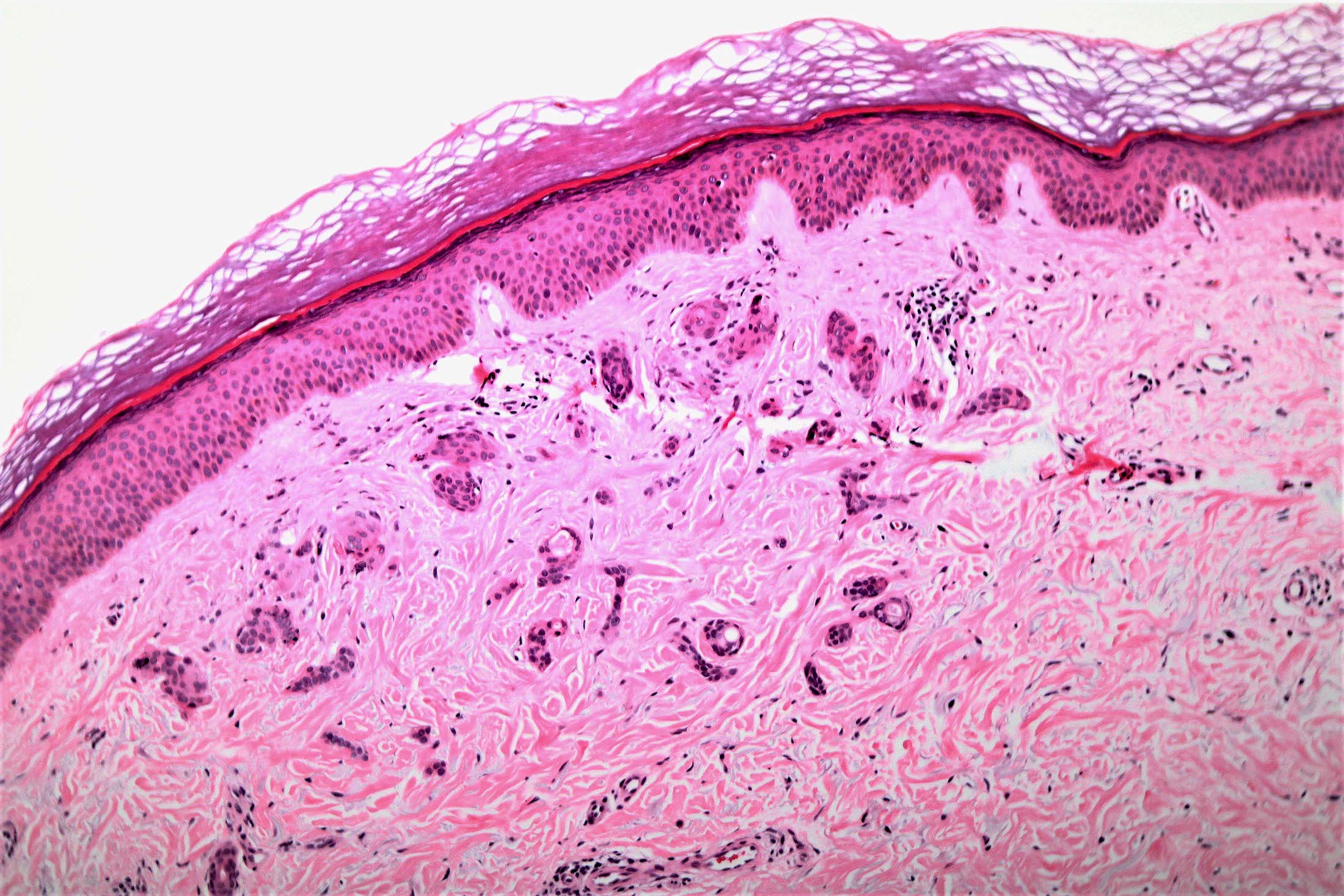
Microscopic (histologic) description
- Well circumscribed proliferation with 2 components:
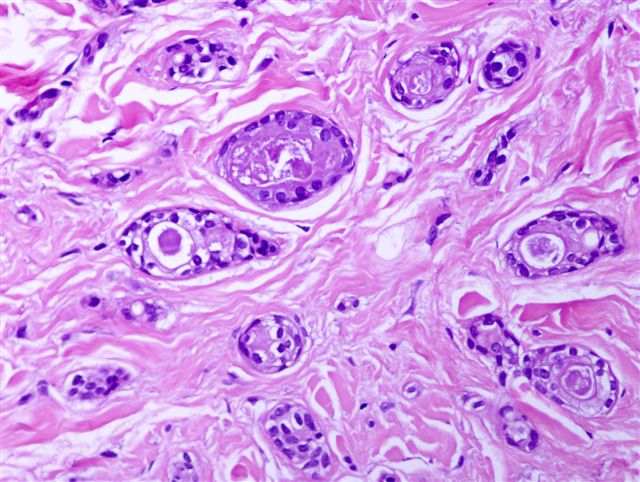
- Epithelial cells forming ductules, nests, cysts and cords
- Cells are basaloid, cuboidal and double layered (in ductules) with an eosinophilic cuticle
- Ducts are often described as comma or tadpole shaped or in a paisley pattern (Hong Kong Med J 2018;24:200)
- May have cell clearing glycogen (clear cell syringoma), more common in diabetics (J Am Acad Dermatol 1987;16:310)
- Some small cysts may have squamous lining
- Variable luminal proteinaceous debris / keratin debris
- Stromal fibrosis / sclerosis
- Epithelial cells forming ductules, nests, cysts and cords
- Usually in superficial reticular dermis, rarely deep dermal extension
- No cytologic atypia
- Very rare mitoses
- Reference: Calonje: McKee's Pathology of the Skin, 5th Edition, 2019
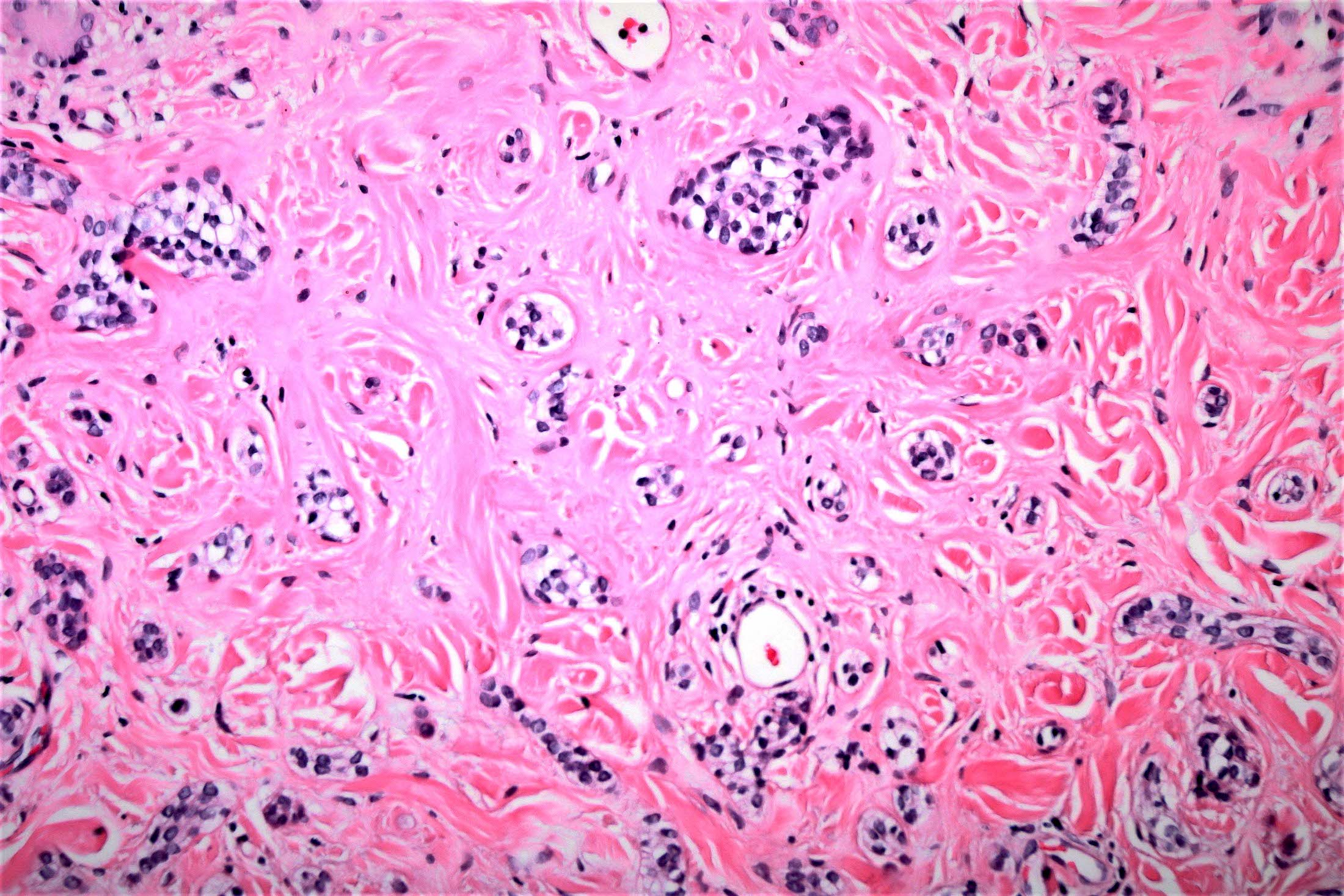
Microscopic (histologic) images
Contributed by Aadil Ahmed, M.D., Sara C. Shalin, M.D., Ph.D. and Nicole Riddle, M.D.
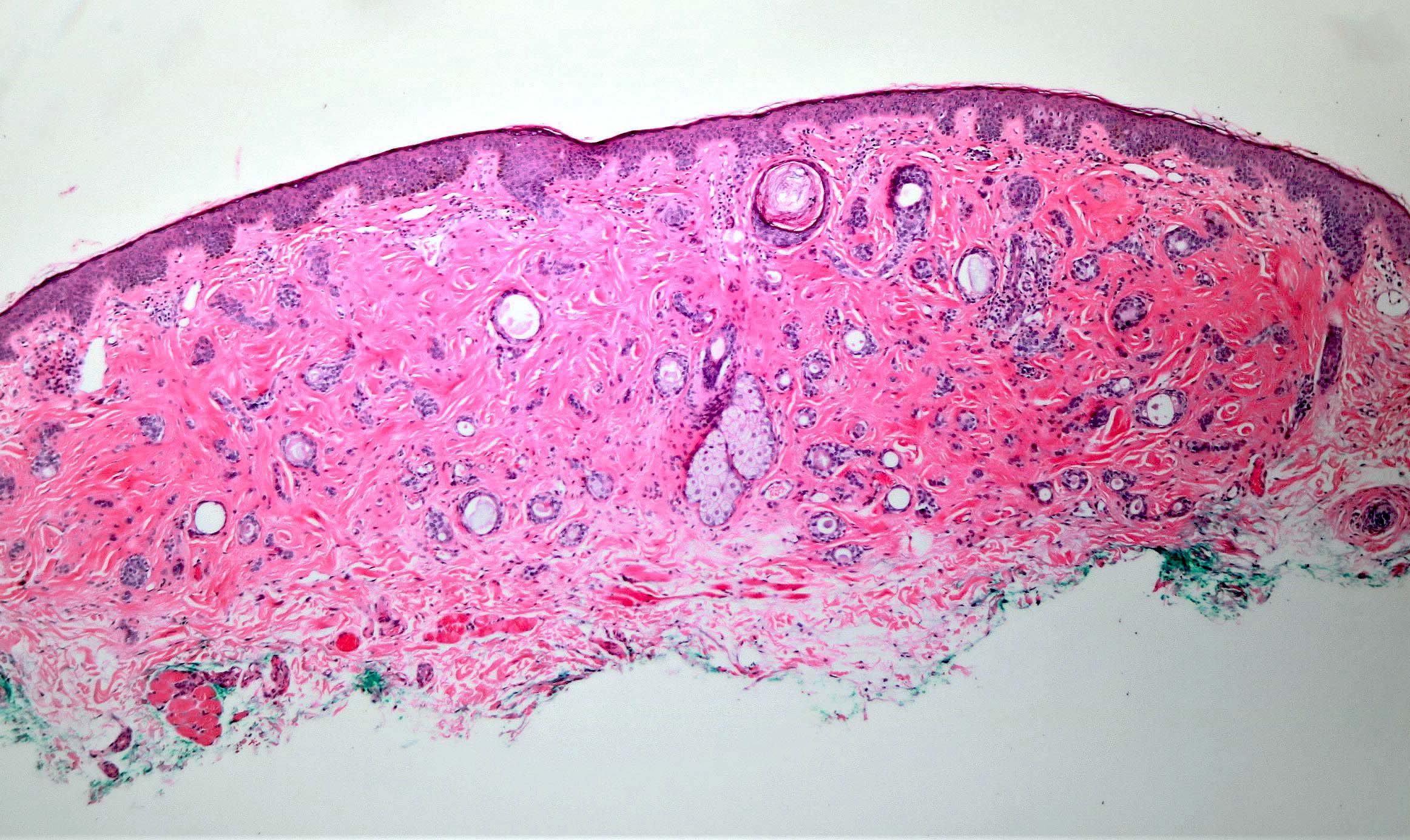
Well circumscribed syringoma
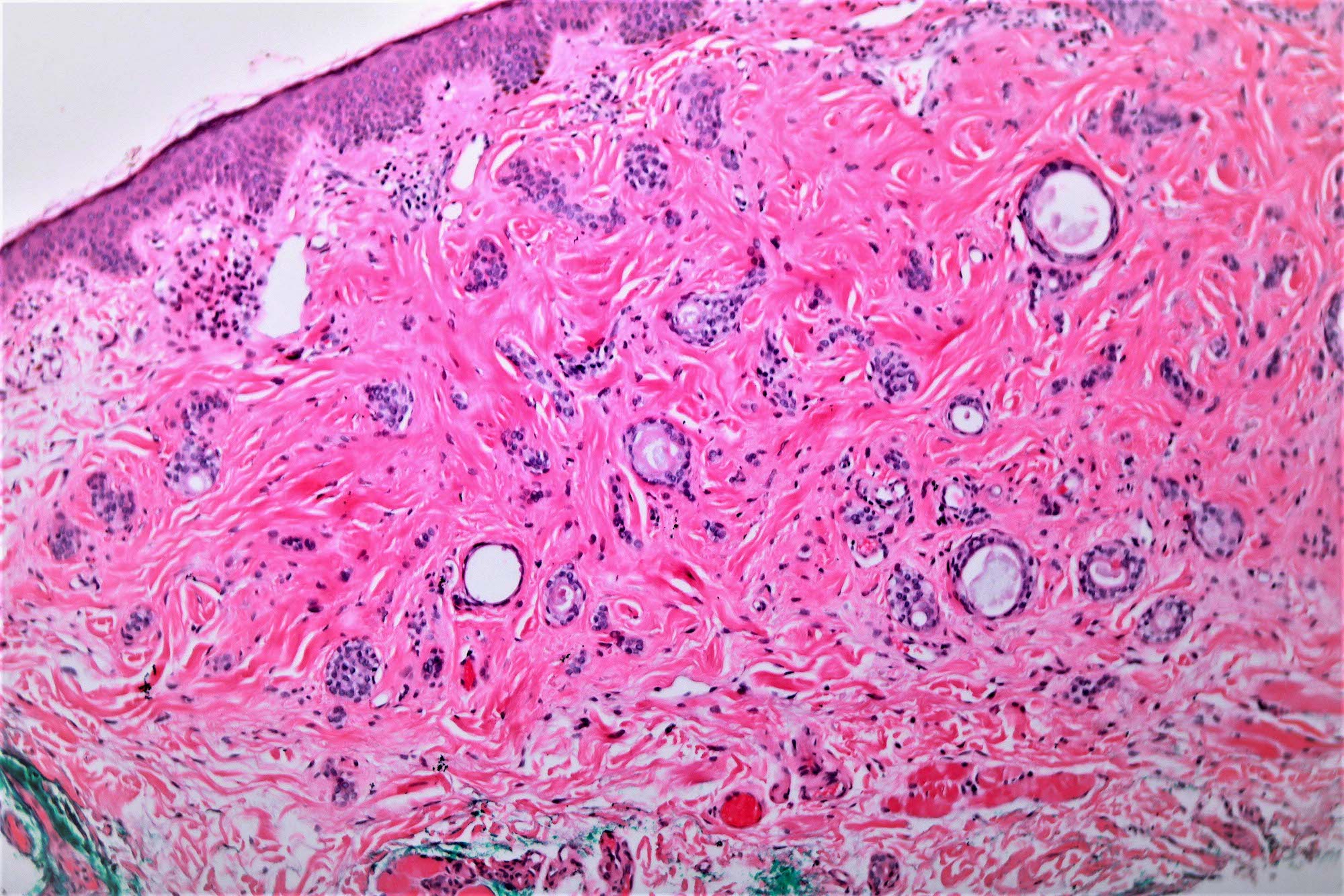
Comma shaped ductules and nests
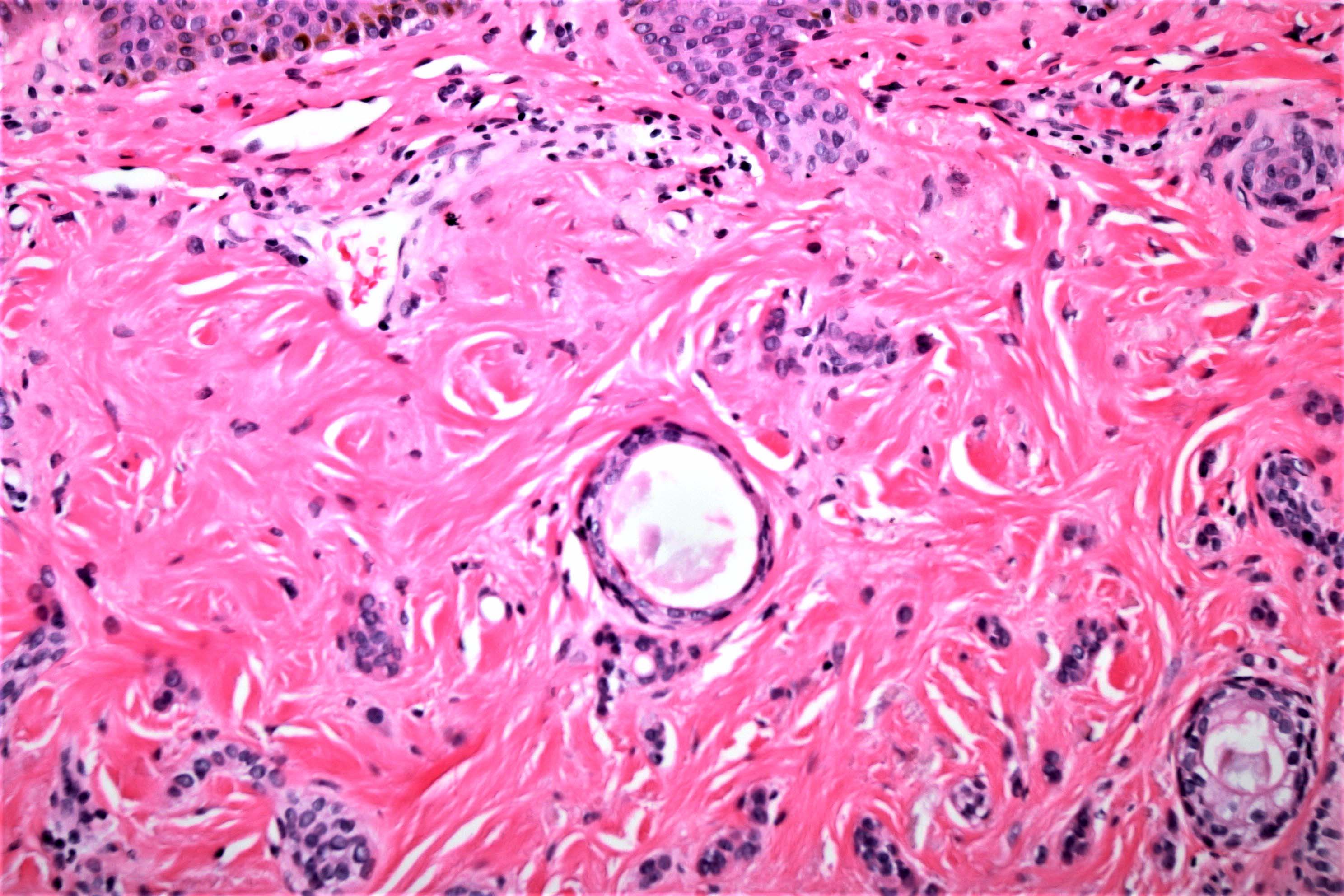
Basaloid proliferation

Paisley or tadpole shaped pattern

Clear cell change
Clear cell syringoma

Conventional and clear cell components
Incidental syringoma
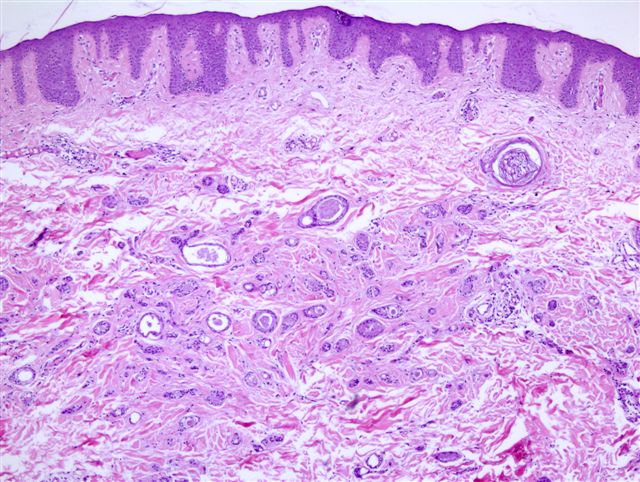
Superficial reticular dermis
Basaloidesque cells
Cytology description
- Basaloid cells, possibly in clusters
- May be clear cells in clear cell variant
- No cytologic atypia
- Very rare mitoses
- Reference: Calonje: McKee's Pathology of the Skin, 5th Edition, 2019
Positive stains
- CEA: luminal surface of sweat ductal cells (Int J Dermatol 2012;51:817)
- EMA: peripheral cells of dermal and intraepidermal ducts; solid strands (Int J Dermatol 2012;51:817)
- CK5: outer cells of dermal ducts; solid strands (Int J Dermatol 2012;51:817)
Negative stains
- Estrogen receptor / ER and progesterone receptor / PR; however, some studies show PR > ER positivity (J Cutan Pathol 1995;22:442)
- SOX10 (Appl Immunohistochem Mol Morphol 2019;27:114)
Electron microscopy description
- Eccrine origin
Molecular / cytogenetics description
- Multiple syringomas may be inherited in autosomal dominant fashion; linked to chromosome 16q22 (Br J Dermatol 2010;162:1083)
Sample pathology report
- Skin, eyelid, biopsy:
- Syringoma
- Microscopic description: Histologic sections show skin with an unremarkable epidermis. Within the superficial dermis, a circumscribed proliferation of multiple ductular structures lined by 2 layers of epithelial cells is present coursing within densely fibrotic stroma. There is minimal cytologic atypia and mitoses are not abundant.
Differential diagnosis
- Microcystic adnexal carcinoma:
- Histologically similar but practically nonexistent in vulva
- Poorly circumscribed, deeply infiltrative, with frequent perineural invasion (J Low Genit Tract Dis 2016;20:e55)
- Desmoplastic trichoepithelioma:
- Practically nonexistent in vulva
- Usually single lesion with keratinous cysts next to strands of basaloid cells and no eosinophil cuticle (Oncol Lett 2015;10:2468)
- Morpheaform basal cell carcinoma:
- Histologically similar with strand-like growth pattern
- Sclerotic stroma with deeply infiltrative, basaloid cells (Arch Pathol Lab Med 2017;141:1490)
Practice question #1
Which of these characteristics is typical of this well circumscribed, dermal lesion?
- Associated with Turner syndrome
- May recur after excision
- Often multiple 1 - 4 mm, firm, flesh colored papules
- Painful lesions
- Strongly SOX10 immunoreactive
Practice answer #1
C. Often multiple 1 - 4 mm, firm, flesh colored papules. The image shows a syringoma. These lesions are often multiple 1 - 4 mm, firm, flesh colored papules. They are typically asymptomatic but may present with pruritus. Various cell components are immunoreactive for CEA, EMA and CK5 but not for SOX10. They have benign behavior and excision is adequate. They are associated with Ehlers-Danlos, Marfan and Down syndromes.
Comment Here
Reference: Syringoma
Comment Here
Reference: Syringoma
Practice question #2
Clear cell change seen in syringomas is due to
- Clearing artifact
- Globulin
- Glycogen
- Lipids
- Mucin
Practice answer #2
C. Glycogen. The ductal cells in syringoma can infrequently exhibit clear cell change in focal areas that is due to accumulation of glycogen. Rarely, all cells are glycogen rich, termed clear cell variant and commonly associated with diabetes mellitus.
Comment Here
Reference: Syringoma
Comment Here
Reference: Syringoma
