Small intestine & ampulla
Benign tumors / tumor-like conditions
Brunner gland lesions
Authors: Mohamed Yakoub, M.D., Divya Sharma, M.D.
Editorial Board Member: Claudio Luchini, M.D., Ph.D.
Deputy Editor-in-Chief: Aaron R. Huber, D.O.


Last author update: 3 August 2023
Last staff update: 9 September 2025
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Brunner gland hyperplasia
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Sample pathology report | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Yakoub M, Sharma D. Brunner gland lesions. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/smallbowelbrunnersgland.html. Accessed September 17th, 2025.
Definition / general
- Brunner gland hyperplasia (BGH) is defined as benign hyperplastic proliferation of mature Brunner glands, commonly in the duodenal bulb
Essential features
- BGH clinical findings can be nonspecific; endoscopies show a polypoid / pedunculated mass that varies in size
- Histologic features show proliferation of Brunner glands that extends to the submucosa
- Smooth muscle proliferation and mature adipose tissue favors Brunner gland hamartoma
Terminology
- Brunner gland hamartoma, Brunner gland adenoma and Brunneroma: > 0.5 cm with dilated glands and smooth muscle proliferation (Adv Ther 2021;38:2779, Rev Esp Enferm Dig 2022;114:124)
ICD coding
- ICD-11: DA53.Y - other specified duodenal polyp
Epidemiology
- BGH represents < 1% of all gastrointestinal tumors and ~5% of benign duodenal tumors (Int J Clin Exp Pathol 2015;8:7565)
- More prevalent from 50 - 70 years old (World J Gastroenterol 2004;10:2616)
- Risk factors (World J Gastroenterol 2004;10:2616)
- High gastric acid secretion
- Helicobacter pylori infection
- Chronic pancreatitis
Sites
- Most common in proximal duodenum (57% in duodenal bulb) (Gastrointest Endosc 1998;47:403)
Pathophysiology
- Poorly understood
- Hypothesized to be embryonic dysplasia of the duodenum (Brunner gland hamartoma) (JNMA J Nepal Med Assoc 2019;57:50)
- High gastric acid secretion can cause BGH, increasing alkaline mucous secretion (Scand J Gastroenterol 1990;25:165)
- Relationship between H. pylori infection and BHG is not clearly understood
Etiology
- Majority of cases have unclear etiology
- High acid environment in the duodenum, H. pylori and chronic pancreatitis may cause duodenal mucosal injury and trigger a repair process that includes foveolar metaplasia and BGH (BMC Gastroenterol 2014;14:14)
Clinical features
- Majority of patients are asymptomatic
- Nonspecific symptoms (J Surg Case Rep 2018;2018:rjy305)
- Dyspepsia, nausea and vomiting
- Abdominal pain and distension
- Rare cases present with gastrointestinal bleeding and iron deficiency anemia (especially in hamartomas and large lesions) (Endosc Ultrasound 2015;4:266)
- Few cases present with intestinal obstructions (lesions > 2 cm) (Am J Gastroenterol 1995;90:290)
- Ampullary lesions can present with biliary obstruction (Endoscopy 2000;32:998)
Diagnosis
- Upper GI endoscopy (EGD)
- Some lesions (especially in posterior wall of duodenum) can be missed on EGD
- Sensitivity of EGD is 72 - 89% (Eur J Radiol 1993;16:115)
- Evaluates extent, size and origin of the lesion
- Duodenal nodule that can be covered by normal mucosa (Gastrointest Endosc 2006;64:464)
- Can mimic lipoma, endocrine tumor or gastrointestinal stromal tumor (GIST) (Trop Gastroenterol 2010;31:121)
- Radiology (barium Xray and abdominal CT)
- More sensitive for larger lesions (J Comput Assist Tomogr 2010;34:543)
- See Radiology description
Radiology description
- Barium Xray
- Sessile or pedunculated polypoid filling lesions (large Brunner gland hamartomas) (Gastroenterol Hepatol (N Y) 2008;4:473)
- Multiple small filling defects and cobblestone pattern (diffuse nodular BGH) (AJR Am J Roentgenol 2006;187:715)
- CT (Dig Liver Dis 2021;53:134)
- Mass in the duodenum with central low attenuation
- Shows the relationship with adjacent organs
Radiology images
Images hosted on other servers:

Duodenum showing cobblestone pattern
Prognostic factors
- Overall good prognosis for most lesions
- Very rare cases of BGH have been reported showing dysplasia or invasive carcinoma (2% and 0.3%, respectively) (Am J Surg Pathol 2005;29:1442, J Gastroenterol 2002;37:293)
Case reports
- 22 year old woman presented with duodenal intussusception due to BGH (Ann Surg 1959;150:160)
- 33 year old woman with large BGH presented with bleeding (Case Rep Surg 2021;2021:8861308)
- 57 year old man with pyloric obstruction due to Brunner gland hamartoma (J Surg Case Rep 2020;2020:rjaa191)
- 60 year old man with BGH mimicking malignant pathology (Int J Surg Case Rep 2021;81:105827)
Treatment
- Endoscopic or surgical resection
- Pancreaticoduodenectomy has been reported for giant hamartomas and diffuse nodular BGH (J Korean Med Sci 2008;23:540)
Clinical images
Contributed by Hany Al Khedr, M.D.
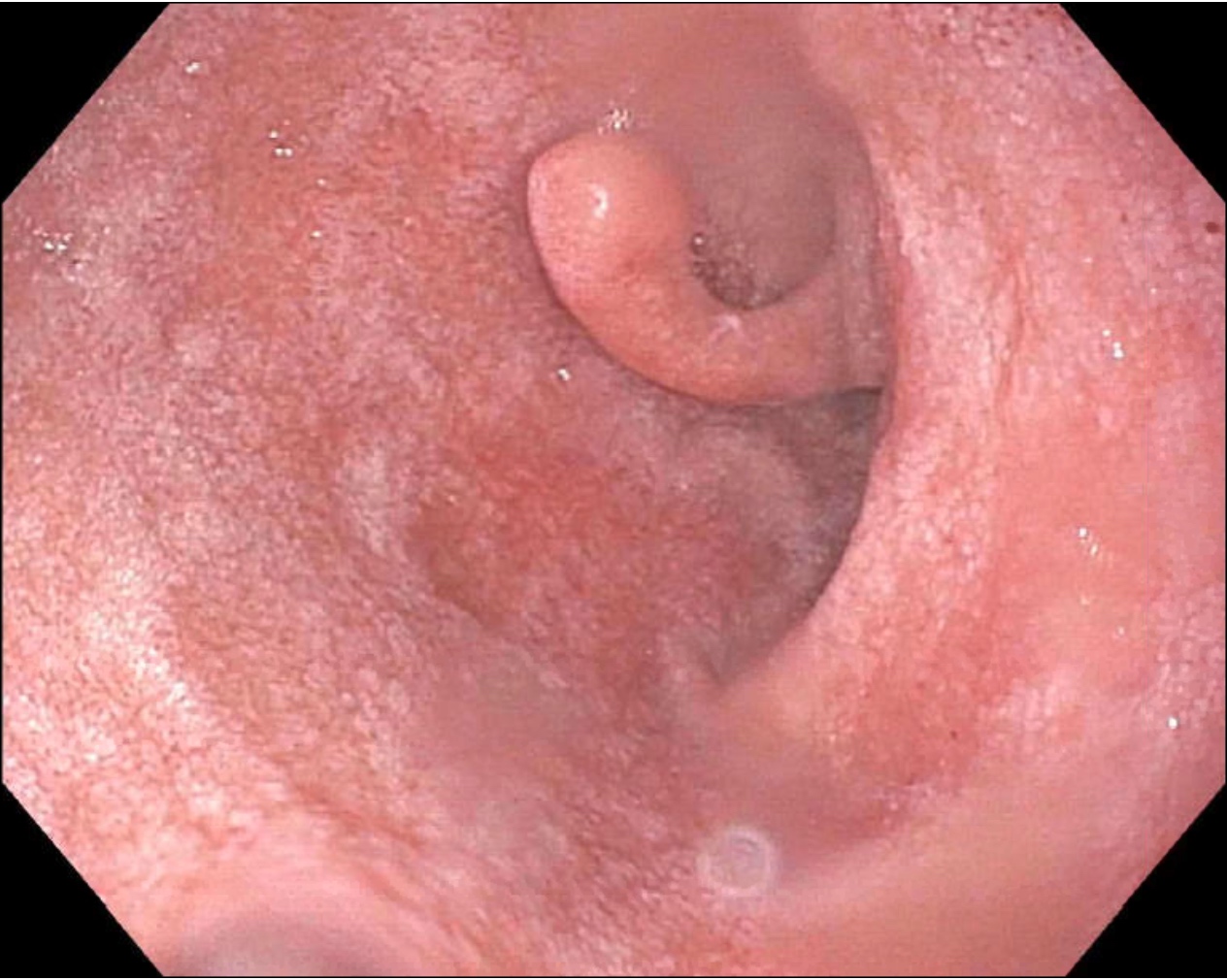
Duodenal bulb polyp endoscopy
Microscopic (histologic) description
- Brunner gland hyperplasia
- Closely packed clusters of cuboidal cells with basal round to flat nuclei and foamy cytoplasm with neutral mucin
- Features of peptic duodenitis, foveolar metaplasia or mucosal injury can be seen (Scand J Gastroenterol 1990;25:165)
- Brunner gland hamartoma
- Typically, larger size: > 0.5 cm
- Smooth muscle and adipose tissue, intermixed with proliferating Brunner glands and cystically dilated ducts
- Brunner glands can be intermingled with mature adipose tissue / adipocytes
- Brunner gland adenoma
- Similar morphology to Brunner gland hyperplasia or hamartoma, with cytological atypia, nuclear enlargement and mitosis (Int J Clin Exp Pathol 2015;8:7565)
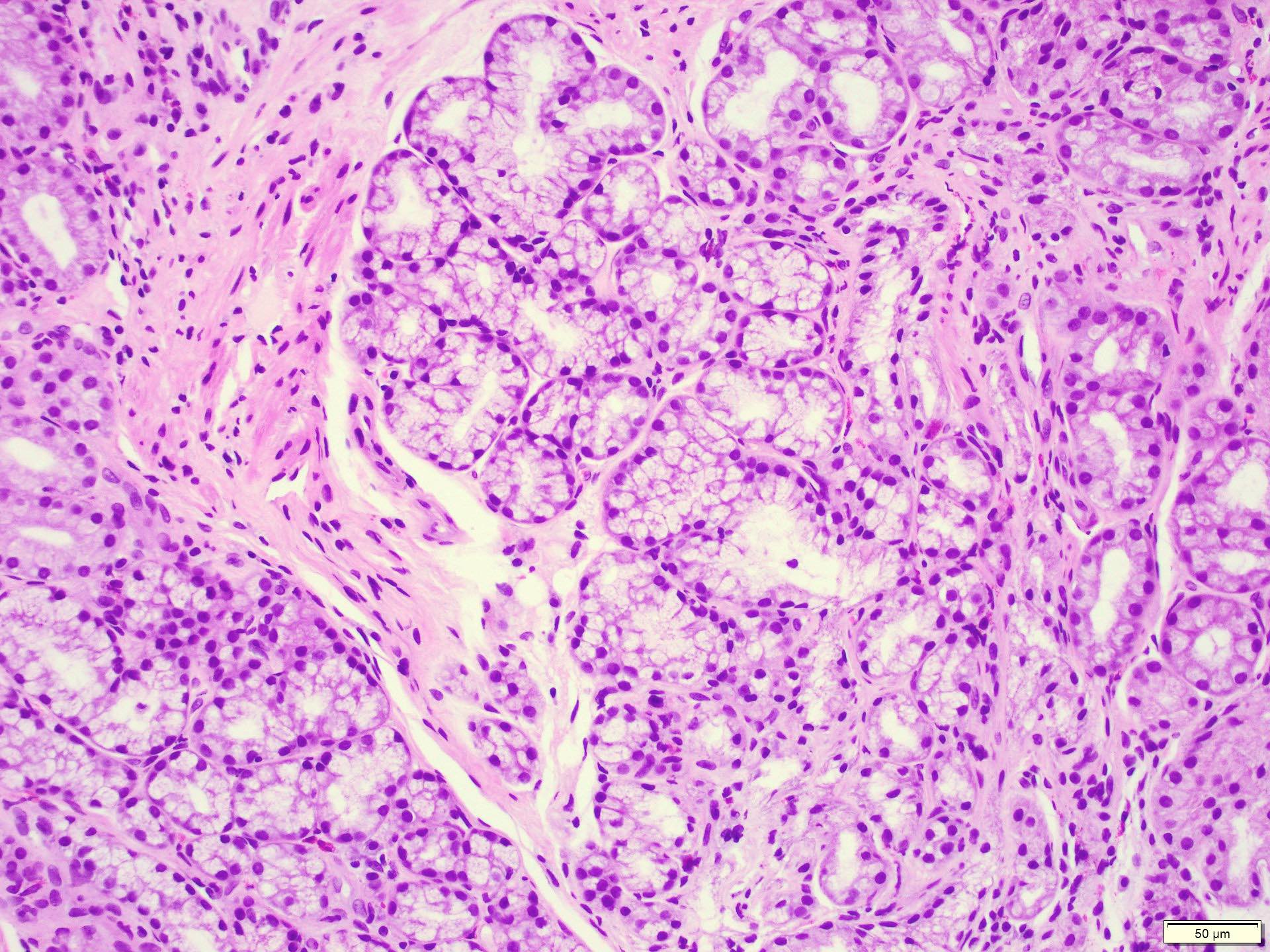
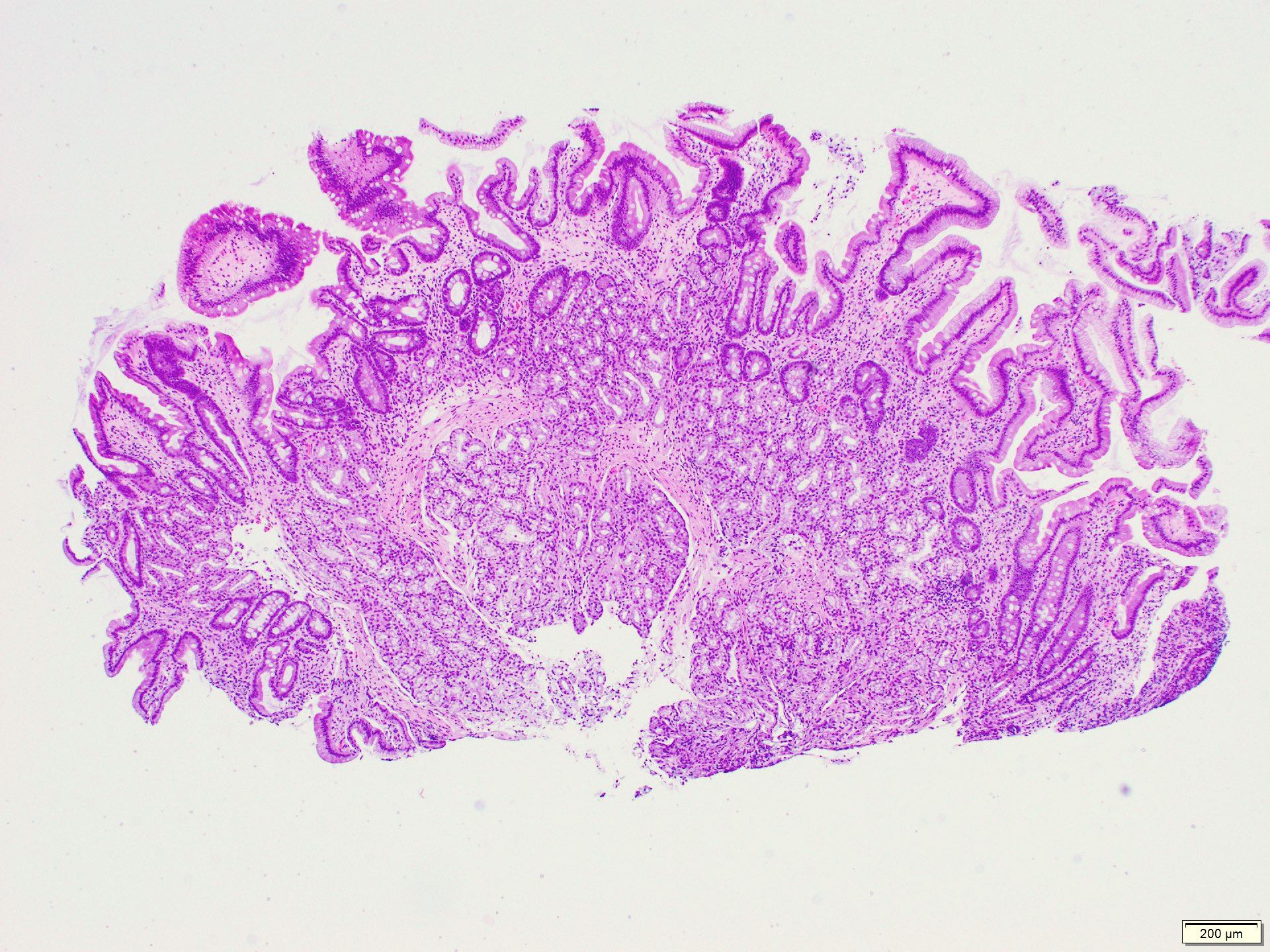
Microscopic (histologic) images
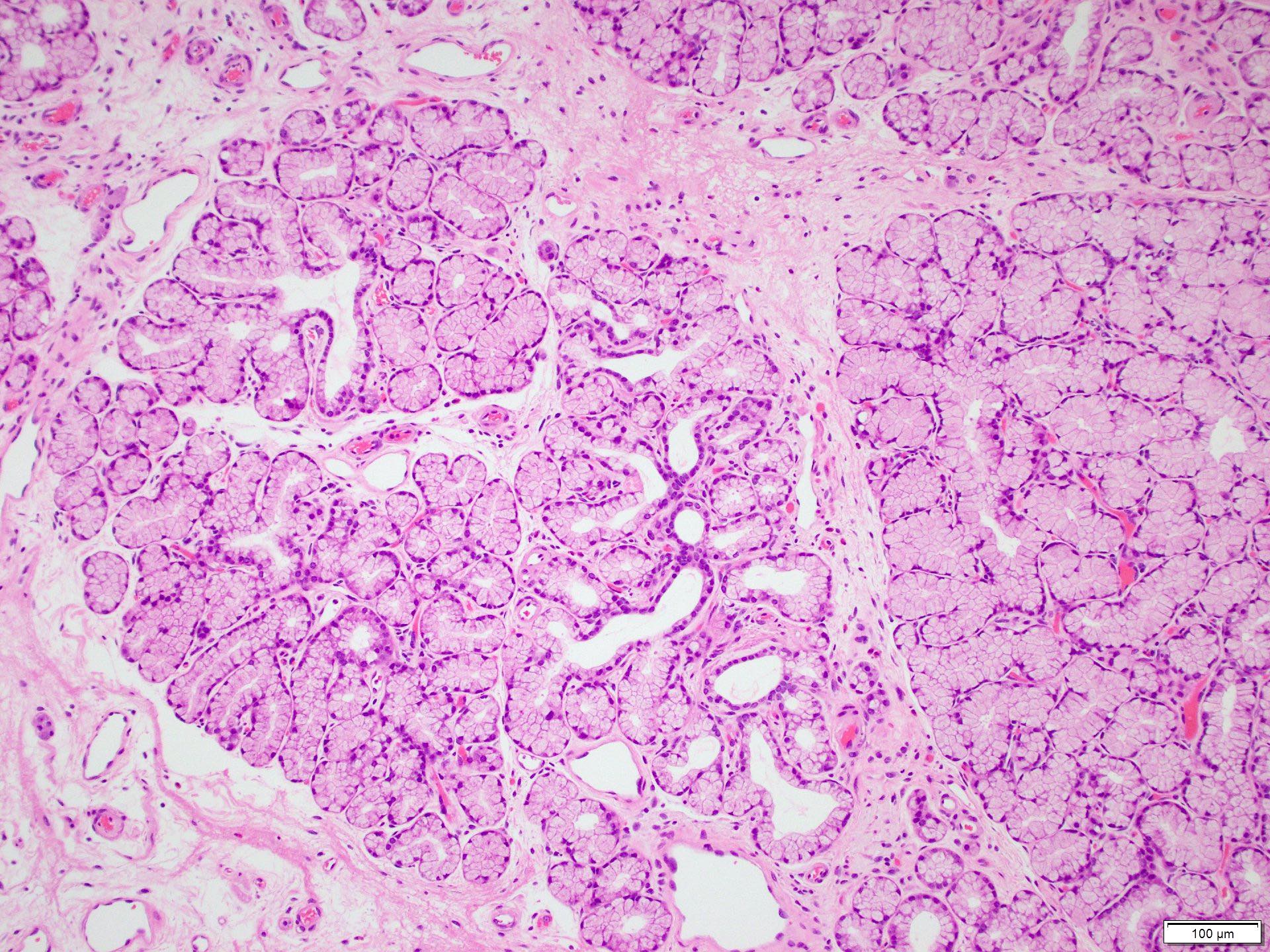
Contributed by Divya Sharma, M.D.
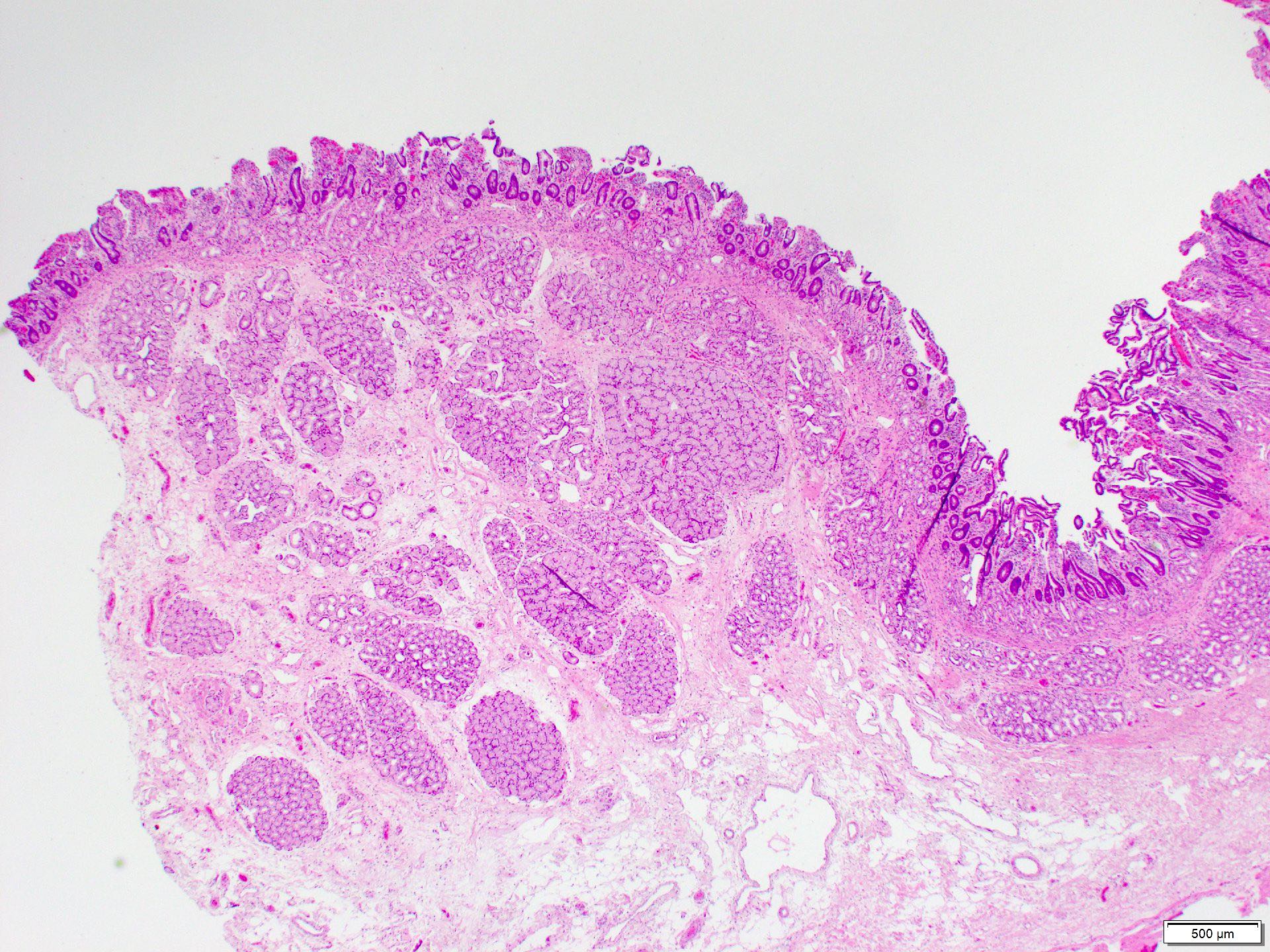
Brunner glands in submucosa
Glands within fibrous stroma
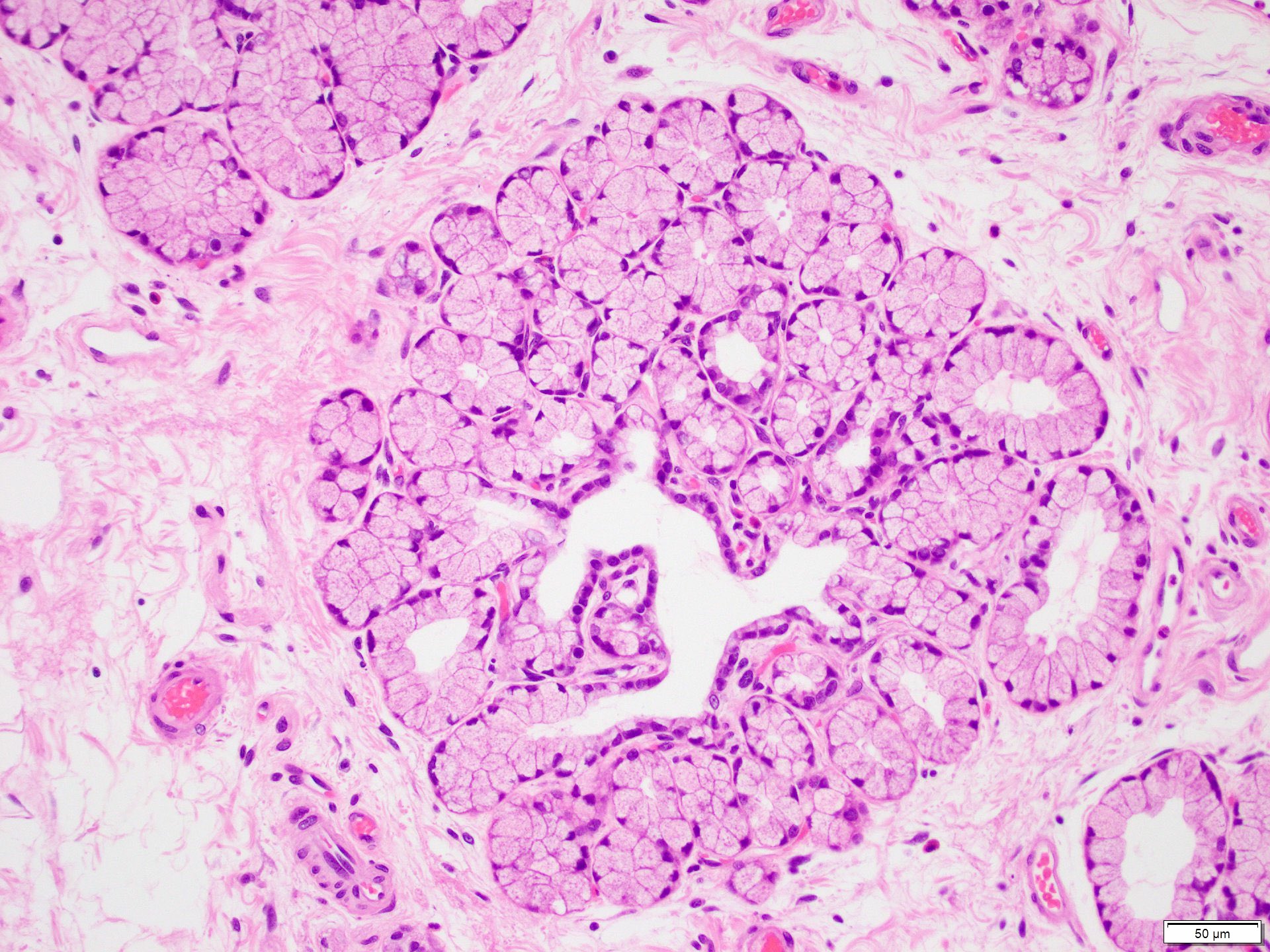
Bland cuboidal cells
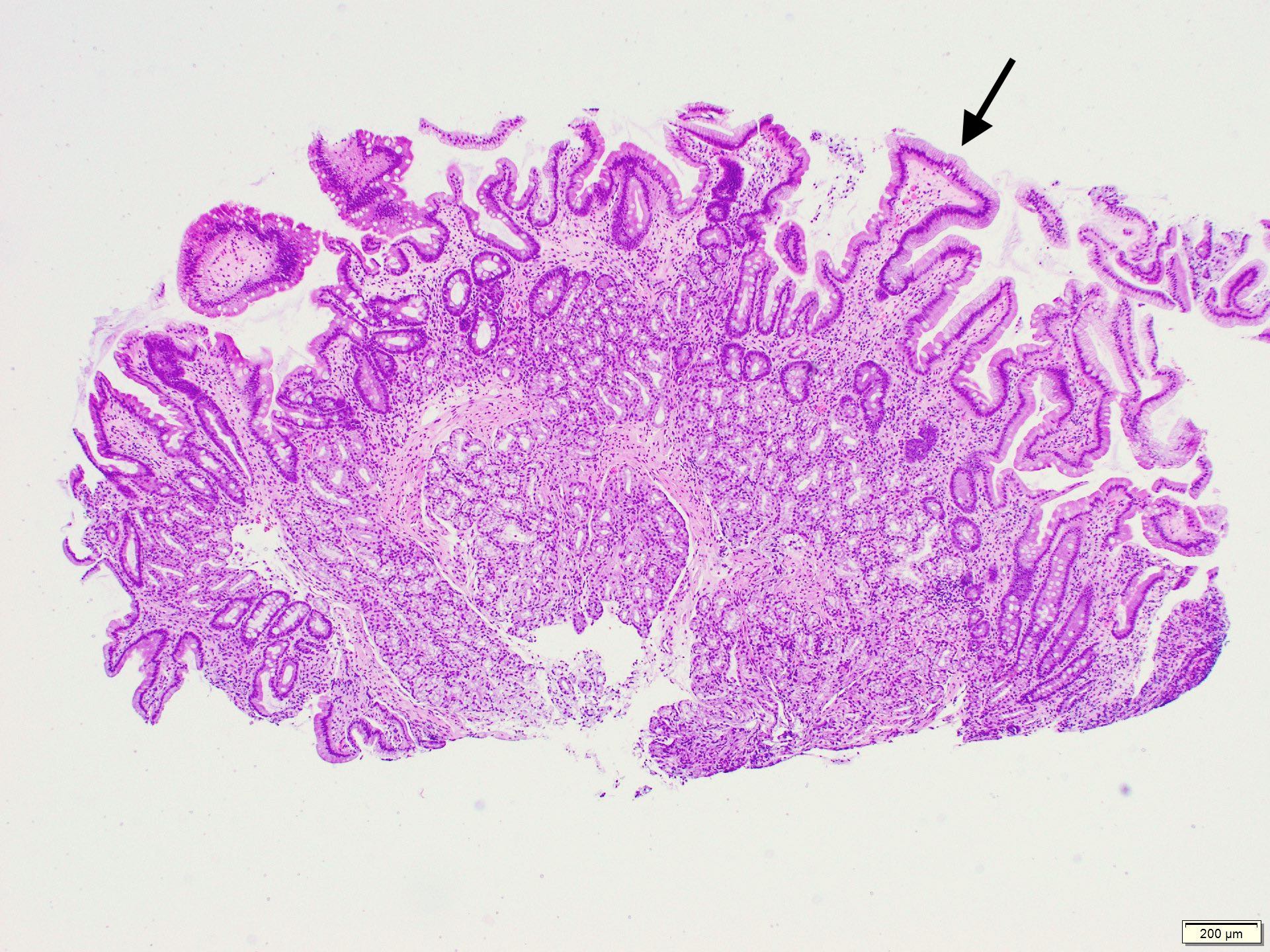
Foveolar metaplasia
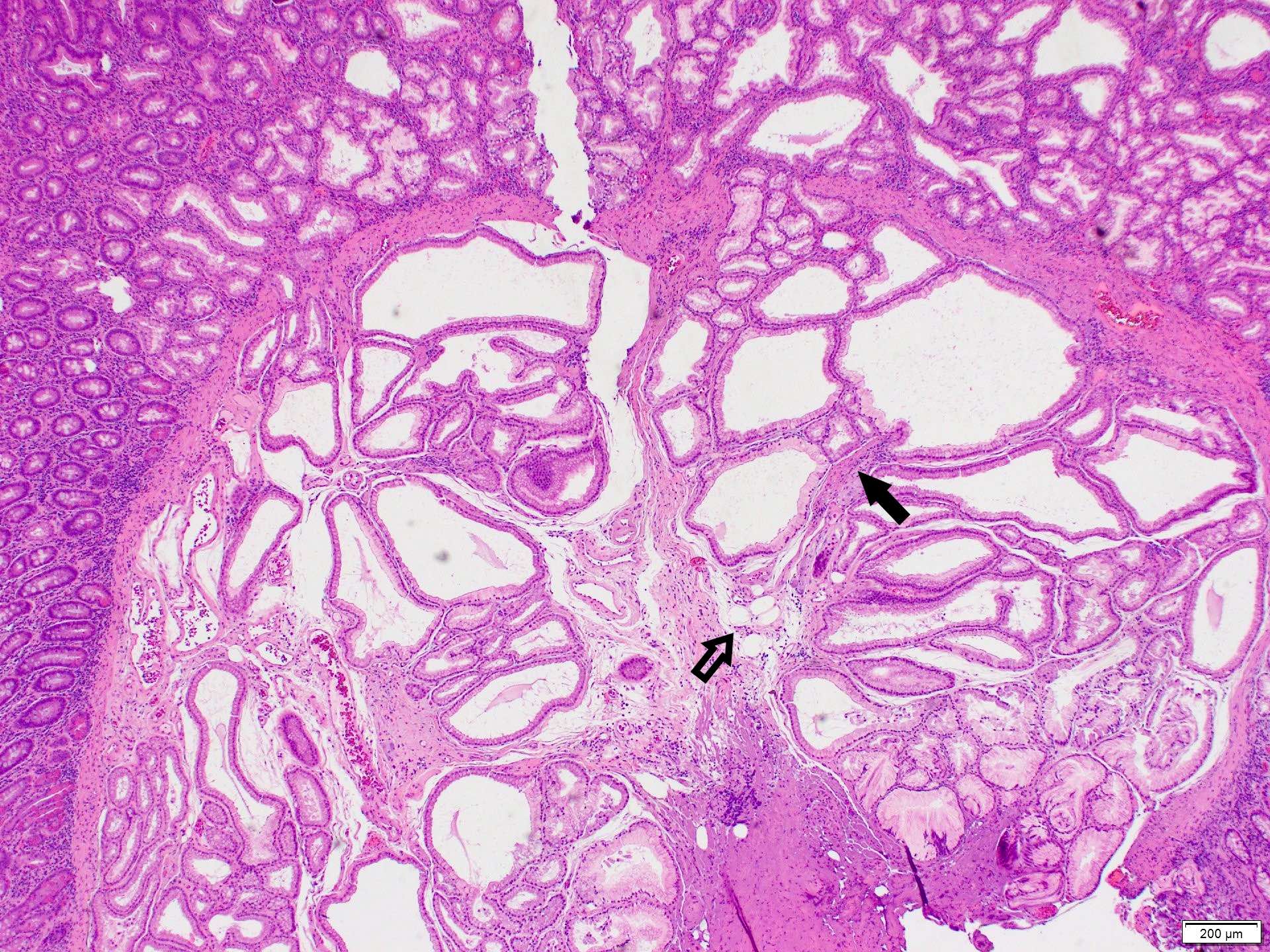
Dilated ducts
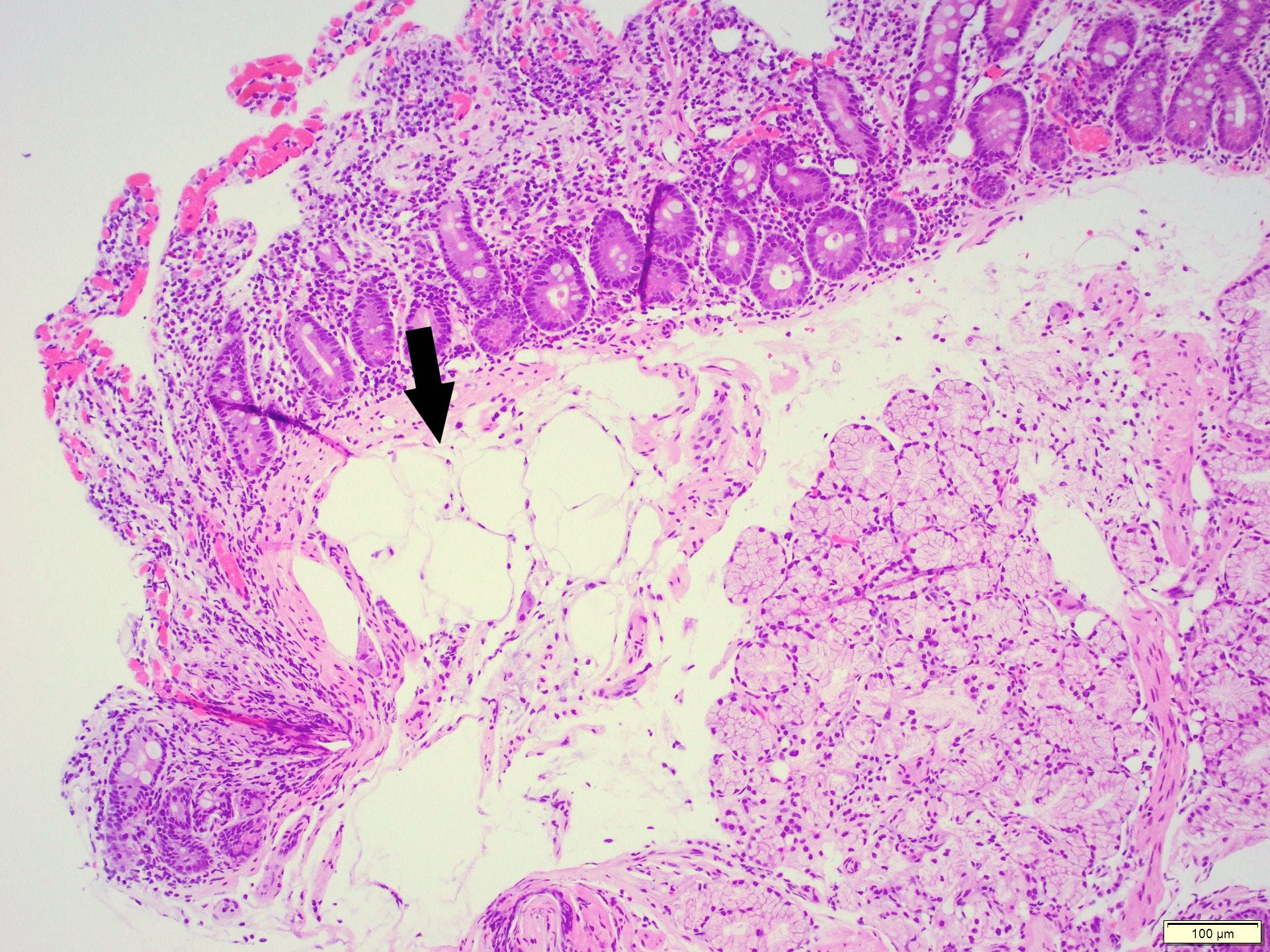
Mature adipocytes
Fibrous septa
Positive stains
Sample pathology report
- Duodenum, polyp, biopsy:
- Polypoid duodenal mucosa with prominent Brunner glands consistent with Brunner gland hyperplasia
- Negative for dysplasia or malignancy
Differential diagnosis
- Gastric heterotopia:
- Commonly in first and second parts of duodenum
- Gastric oxyntic glands with foveolar epithelium on the surface
- Pancreatic heterotopia:
- Variable mixture of elements of normal pancreatic tissue including acini, ducts or islet cells
- Neuroendocrine tumors:
- Commonly in first and second parts of duodenum, including the ampulla
- Nests of uniform cells with round to oval nuclei with salt and pepper chromatin
- Tumor cells are positive for chromogranin A and synaptophysin
- Duodenal adenoma:
- Common in the ampullary area
- Tubular or villous architecture with dysplasia of the surface epithelium
- Gastrointestinal stromal tumor (GIST):
- Leiomyoma:
- Incidental finding
- Can be merged with muscularis mucosa
- Positive for smooth muscle actin and desmin
- Lipoma:
- Rare, submucosal
- May be ulcerated
- Needs to be distinguished from fat rich Brunner gland hamartoma
Additional references
Practice question #1
A 52 year old man with history of dyspepsia and abdominal pain. The upper GI endoscopy showed a 0.5 cm polyp in the duodenal bulb. Which of the following is a possible etiology of the findings depicted in the image above?
- Gastric atrophy
- Immunosuppression
- Increased duodenal acidic environment
- Inflammatory bowel disease
Practice answer #1
C. Increased duodenal acidic environment. The biopsy findings show Brunner gland hyperplasia with focal foveolar metaplasia. A possible etiology of Brunner gland hyperplasia is increased gastric acidity with compensatory increased alkaline secretion by Brunner glands in the duodenum. Answer D is incorrect due to a lack of chronic inflammation and mucosal injury. Answer B is incorrect due to lack of additional findings associated with immunosuppression like infectious agents or inflammation. Answer A is incorrect as Brunner gland hyperplasia is usually associated with gastric increased acid secretion, not gastric atrophy.
Comment Here
Reference: Brunner gland hyperplasia
Comment Here
Reference: Brunner gland hyperplasia
Practice question #2
The figure above is from a duodenal biopsy in a patient with duodenal polyp on upper GI endoscopy. Which of the following, if present, favors a diagnosis of Brunner gland hamartoma over Brunner gland hyperplasia?
- Lesion size < 0.5 cm
- Presence of foveolar metaplasia
- Smooth muscle proliferation
- Superficial lesion limited to the mucosa
Practice answer #2
C. Smooth muscle proliferation. Brunner gland hamartoma is typically a larger lesion (> 0.5 cm), composed of proliferation of Brunner glands, smooth muscle and mature adipose tissue. Brunner gland hyperplasia usually presents as a small lesion (< 0.5 cm) showing only hyperplastic Brunner glands with or without foveolar metaplasia. Answer D is incorrect as both Brunner gland hamartoma and hyperplasia can extend to the submucosa. Answer A is incorrect as Brunner gland hamartoma is usually > 0.5 cm in size. Answer B is incorrect as foveolar metaplasia is mostly associated with Brunner gland hyperplasia.
Comment Here
Reference: Brunner gland hyperplasia
Comment Here
Reference: Brunner gland hyperplasia
