Soft tissue
Uncertain differentiation
Undifferentiated / unclassified sarcoma

Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Undifferentiated / unclassified sarcoma
- Undifferentiated sarcoma shows no identifiable line of differentiation when analyzed by presently available technology (WHO 5th edition) (Surg Oncol Clin N Am 2022;31:321)
- Not included are dedifferentiated subtypes of specific soft tissue sarcomas, such as dedifferentiated liposarcoma, in which the high grade component is commonly undifferentiated
- Spindle cell, pleomorphic, epithelioid and round cells (WHO 5th edition)
- Most often high grade morphology
- Absence of any morphological and immunohistochemical features of specific differentiation
- Absence of distinctive molecular aberration
- ICD-O: 8805/3 - undifferentiated sarcoma
- ICD-11
- 2B5F.2 & XH73J4 - sarcoma, not elsewhere classified of other specific sites & giant cell sarcoma
- 2B5F.2 & XH0947 - sarcoma, not elsewhere classified of other specific sites & malignant fibrous histiocytoma
- 2B5F.2 & XH6HY6 - sarcoma, not elsewhere classified of other specific sites & undifferentiated sarcoma
- 2B5F.2 & XH85G7 - sarcoma, not elsewhere classified of other specific sites & small cell sarcoma
- Accounts for as many as 20% of all soft tissue sarcomas
- Tumor occurs most frequently in the soft tissues of extremities (50% in lower limbs, 20% in upper limbs) and occasionally in bone and viscera (WHO 5th edition) (Cancer Control 2021;28:10732748211036775)
- Peaks around the age of 60 years and is more common in men
- Tumors with pleomorphic morphology (undifferentiated pleomorphic sarcoma) occur mostly in older adults
- May be found in any location (WHO 5th edition)
- Most common in the somatic soft tissue
- Genetic alterations, such as mutations, deletions, epigenetic modifications, may be important for undifferentiated sarcoma development and progression; although they are nonspecific
- Recent investigation had classified TP53, ATRX, H3F3A, ZFHX3, CSMD3, PRPRT, TRIO, CLTC, PDGFRB, ALK, PTCH1, RET, ERBB4, JAK3, GATA1, PIK3CG, RARA and MYH9 as cancer driver genes (Front Genet 2023;14:1109491, J Pathol 2019;247:166)
- Numerical and structural variants underlying chromosomal aberrations are frequently observed in undifferentiated sarcoma, indicating the critical role of high chromosomal instability in the sarcomagenesis and progression (Front Genet 2023;14:1109491)
- Losses of 13q12-q14 or 13q21 were observed in a large proportion of tumors, suggesting that a gene localized in this region could act as a tumor suppressor gene (Cancer Genet Cytogenet 1999;111:134)
- Exact pathogenic mechanisms of undifferentiated sarcoma remain obscure
- Hedgehog signaling pathway plays a role in the proliferation and malignancy (Cancer Res 2012;72:1013)
- Hippo pathway may also be implicated in undifferentiated sarcoma tumor biology, as vestigial-like family member 3 (VGLL3) and YES1 associated transcriptional regulator (YAP1) cofactors were found to be highly amplified on a genome sequencing study (Genes Chromosomes Cancer 2010;49:1161)
- Radiation therapy associated undifferentiated sarcomas (Ann Surg Oncol 2015;22:3913)
- PRDM10 fusions are present in ~5% of undifferentiated sarcoma; all tumors were morphologically low grade and none of the patients developed metastases
- PRDM10 fusion positive sarcomas may constitute a clinically important subset of undifferentiated sarcoma (Clin Cancer Res 2015;21:864)
Images hosted on other servers:

Potential pathways for sarcomagenesis

Role of Skp2 and p16

Confluent network of pathways

Potential involvement of pathways
- Has no characteristic clinical features that distinguish it from other types of sarcomas, other than a frequently rapid growth rate (Int J Surg Case Rep 2023;105:108104)
- Diagnosis of exclusion (WHO 5th edition)
- Atypical spindle cell, pleomorphic, epithelioid and round cells
- High grade morphology in the majority of cases
- Absence of any morphological and immunohistochemical features of specific differentiation
- Complex and not specific cytogenetic abnormalities
- Undifferentiated round cell sarcoma can be diagnosed only if distinctive gene fusions have been ruled out; they are most frequent in young patients
- Computed tomography (CT) (Meyers: MRI of Bone and Soft Tissue Tumors and Tumorlike Lesions, 1st Edition, 2007, Manaster: Musculoskeletal Imaging, 2nd Edition, 2002)
- Density of undifferentiated pleomorphic sarcoma is typically similar to adjacent muscle, with heterogeneous lower density areas if hemorrhage, necrosis or myxoid material is abundant; the soft tissue component enhances
- Magnetic resonance imaging (MRI) (Meyers: MRI of Bone and Soft Tissue Tumors and Tumorlike Lesions, 1st Edition, 2007, Manaster: Musculoskeletal Imaging, 2nd Edition, 2002)
- MRI is the modality of choice for assessing soft tissue sarcomas, as it is best able to locally stage a tumor
- These tumors are typically relatively well circumscribed, located within or adjacent to muscle, exerting a positive mass effect on surrounding structures due to their (usual) large size at presentation
- T1
- Intermediate (to low) signal intensity, similar to adjacent muscle
- Heterogeneity if hemorrhage, calcification, necrosis, myxoid material present
- T2
- Intermediate to high signal intensity
- Heterogeneity if hemorrhage, calcification, necrosis, myxoid material present
Contributed by Borislav A. Alexiev, M.D.

T1 isointense mass
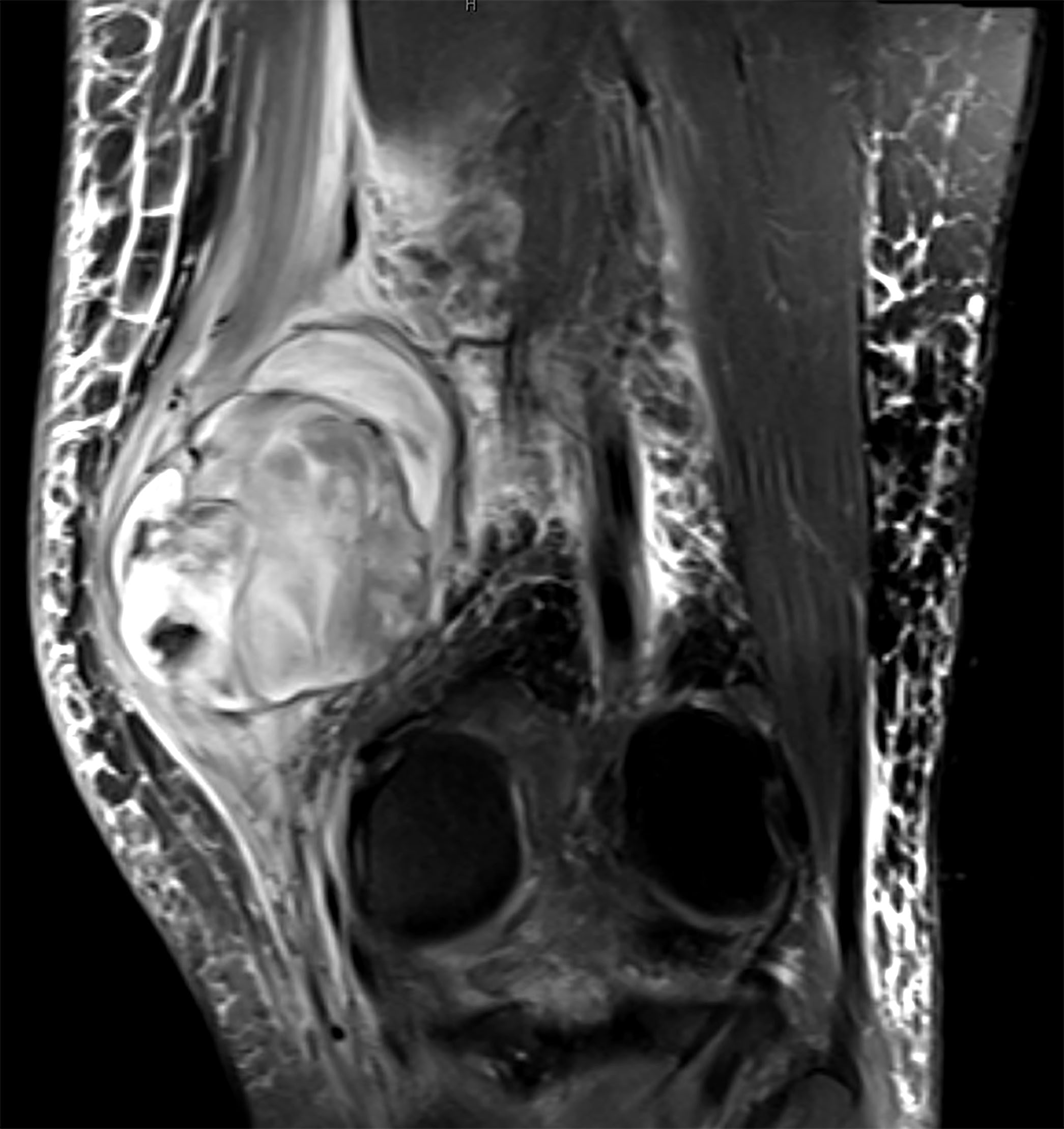
T2 hyperintense mass
- Deep tumor location and AJCC stage are the most important predictive prognostic factors (Pathol Int 2002;52:595)
- Other factors that indicate a poorer prognosis include inadequate surgical margin around the tumor, metastatic spread, large tumor size and older age
- Vast majority of undifferentiated sarcomas are high grade lesions, with a local recurrence rate of 19 - 31%, a metastatic rate of 31 - 35% and a 5 year survival of 65 - 70% (Mod Pathol 2014;27:S39)
- Only a minority of patients develop metastases after 5 years, with the common metastatic sites being lung (90%), bone (8%) and liver (1%); regional lymph node metastases are decidedly uncommon (Mod Pathol 2014;27:S39)
- Undifferentiated sarcoma arising in the limbs or trunk has a reported 5 year metastasis free survival rate of 83% (J Clin Oncol 2001;19:3045)
- Undifferentiated sarcoma with epithelioid morphology seems to be more aggressive; in a recent study, the 5 and 10 year disease specific survival rates were 43% and 42%, respectively (Oncologist 2011;16:512)
- 34 year old woman with lower back mass (Int J Surg Case Rep 2023;105:108104)
- 59 year old man with abdominal mass (Front Surg 2023;10:1166764)
- 62 year old woman with right thigh mass (Am J Case Rep 2019;20:318)
- 85 year old woman with rectal mass (World J Surg Oncol 2022;20:199)
- Surgery in combination with radiotherapy (sporadically combined with chemotherapy in case of high risk of development of metastasis) is the common therapy of choice for undifferentiated sarcoma, which is similar to the treatment of other soft tissue sarcomas (Eur J Surg Oncol 2022;48:985)
- Standard treatment option for patients who present with unresectable soft tissue sarcomas is use of chemotherapeutic agents (Cancer 2023;129:3417)
Images hosted on other servers

Lower back mass
- Generally circumscribed, multilobulated (Lindberg: Diagnostic Pathology - Soft Tissue Tumors, 2nd Edition, 2015)
- Heterogeneous cut surface with gray-tan firm and fleshy areas
- Necrosis and hemorrhage are common
Contributed by Borislav A. Alexiev, M.D.
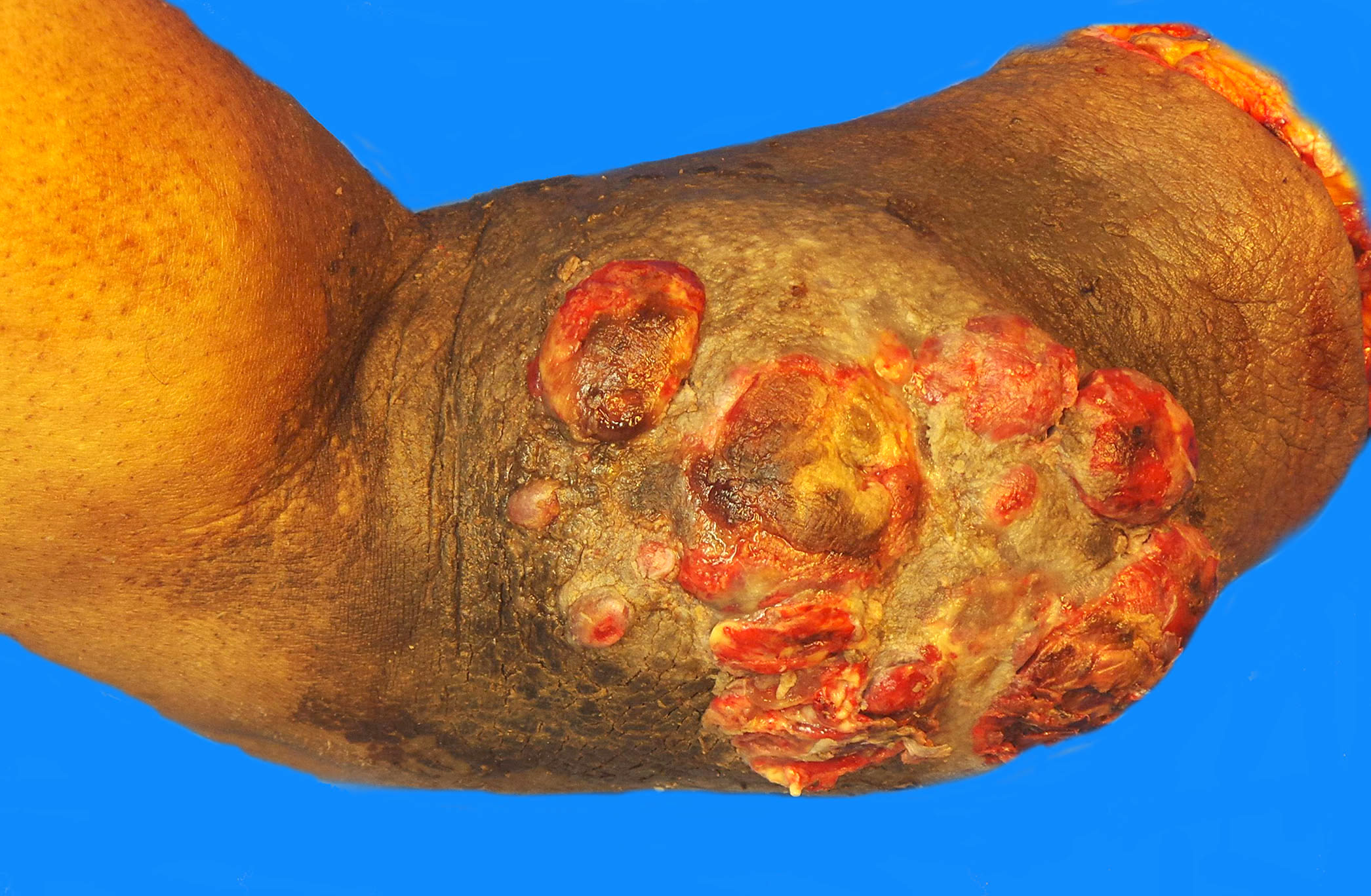
Ulcerated mass
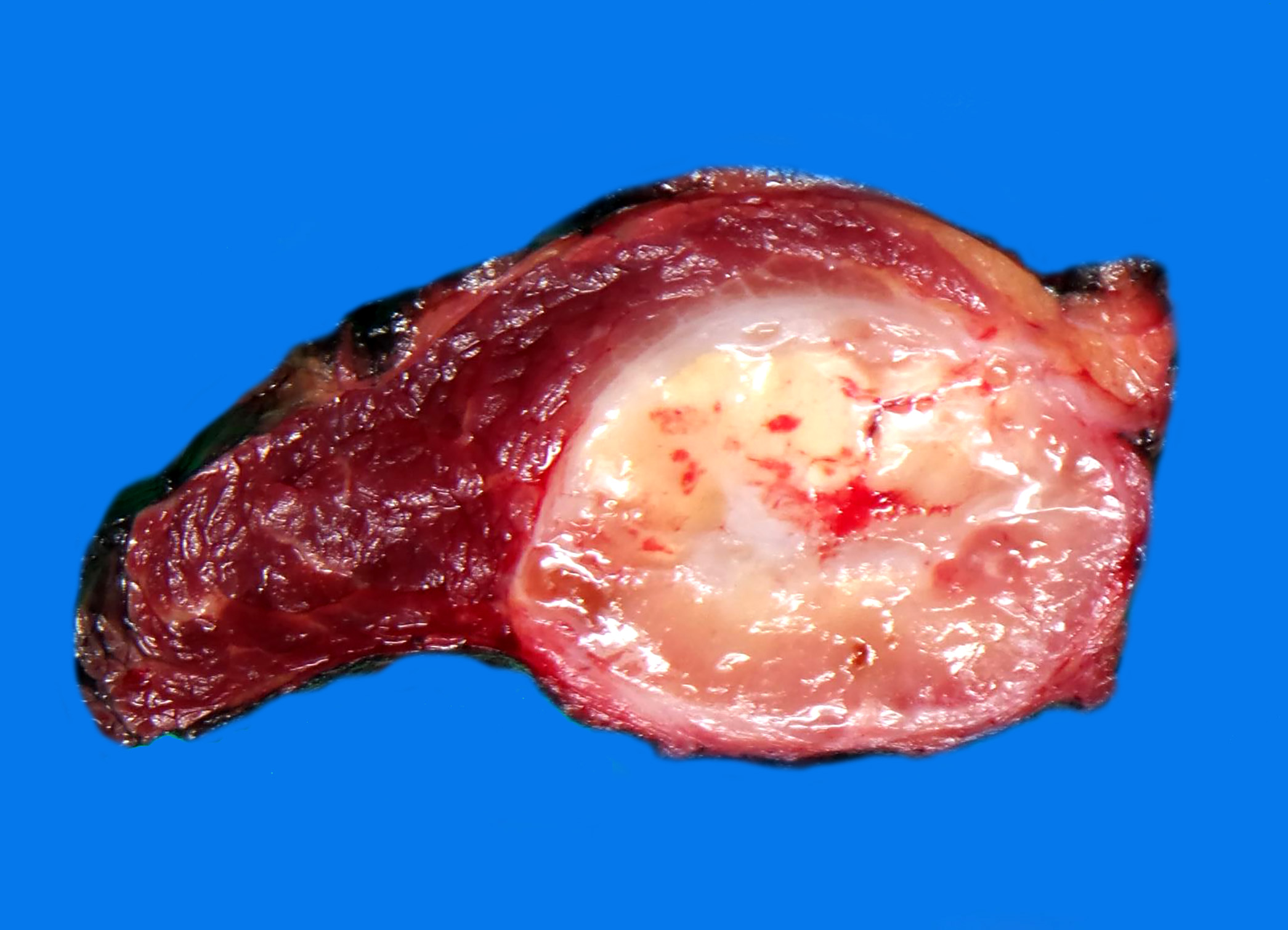
Intramuscular mass
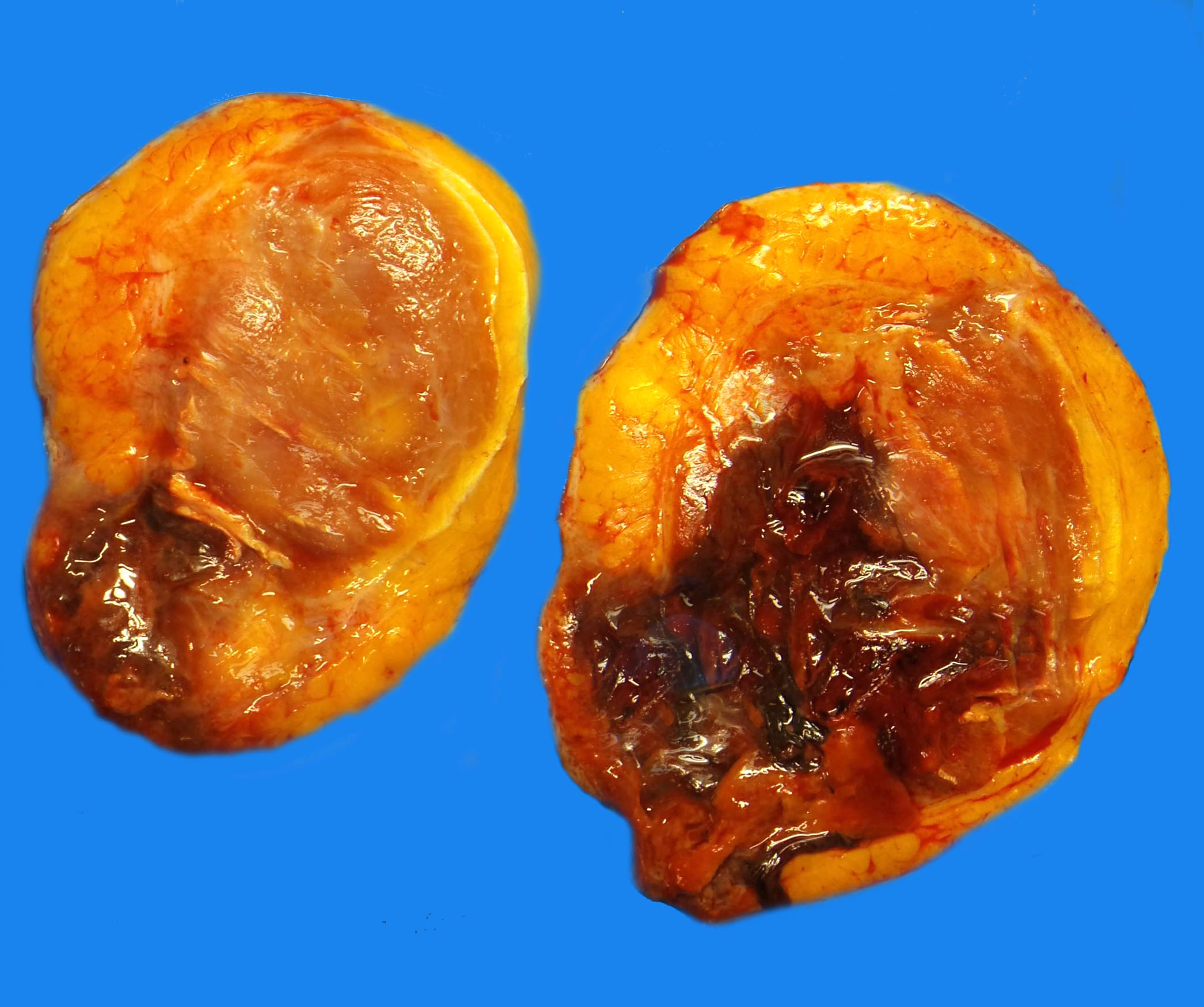
Necrotic mass
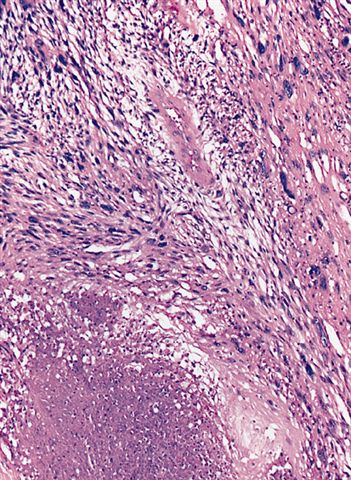
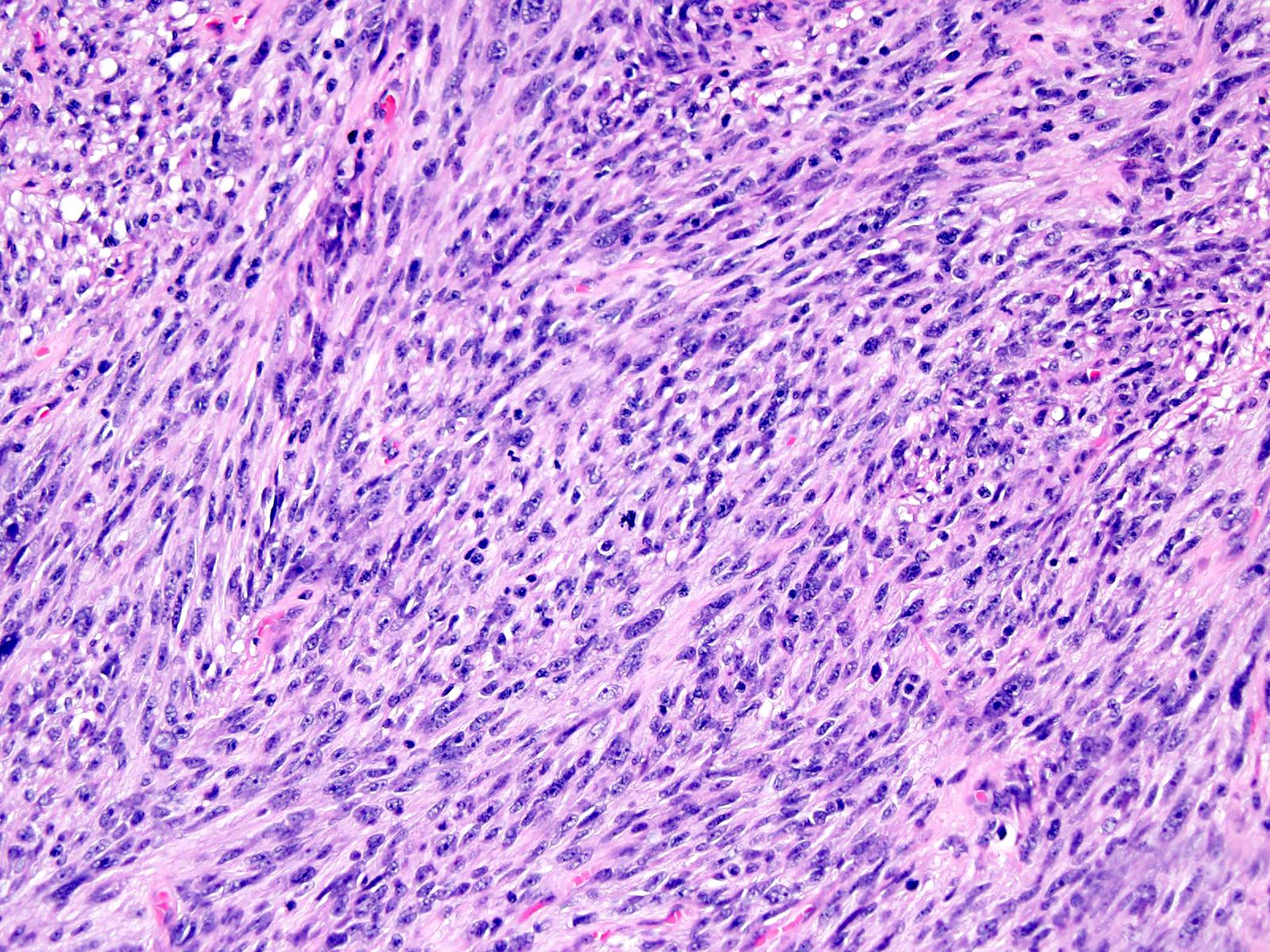
- Storiform, fascicular or patternless arrangement of highly atypical spindled, epithelioid or pleomorphic cells (Lindberg: Diagnostic Pathology - Soft Tissue Tumors, 2nd Edition, 2015)
- Abundant mitoses
- Coagulative necrosis is common
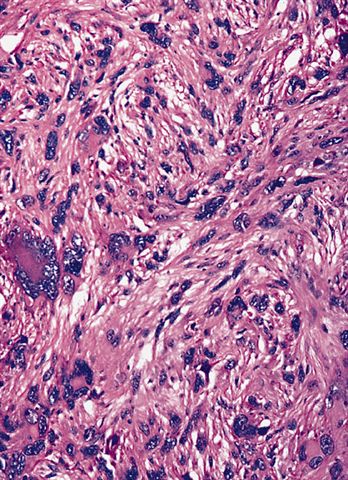
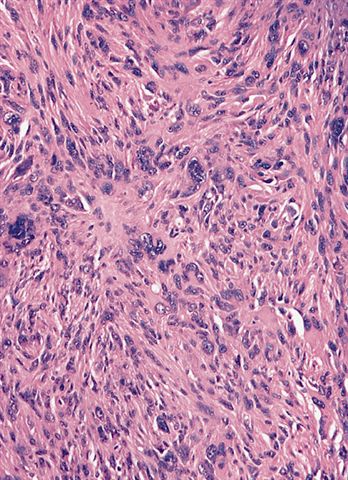
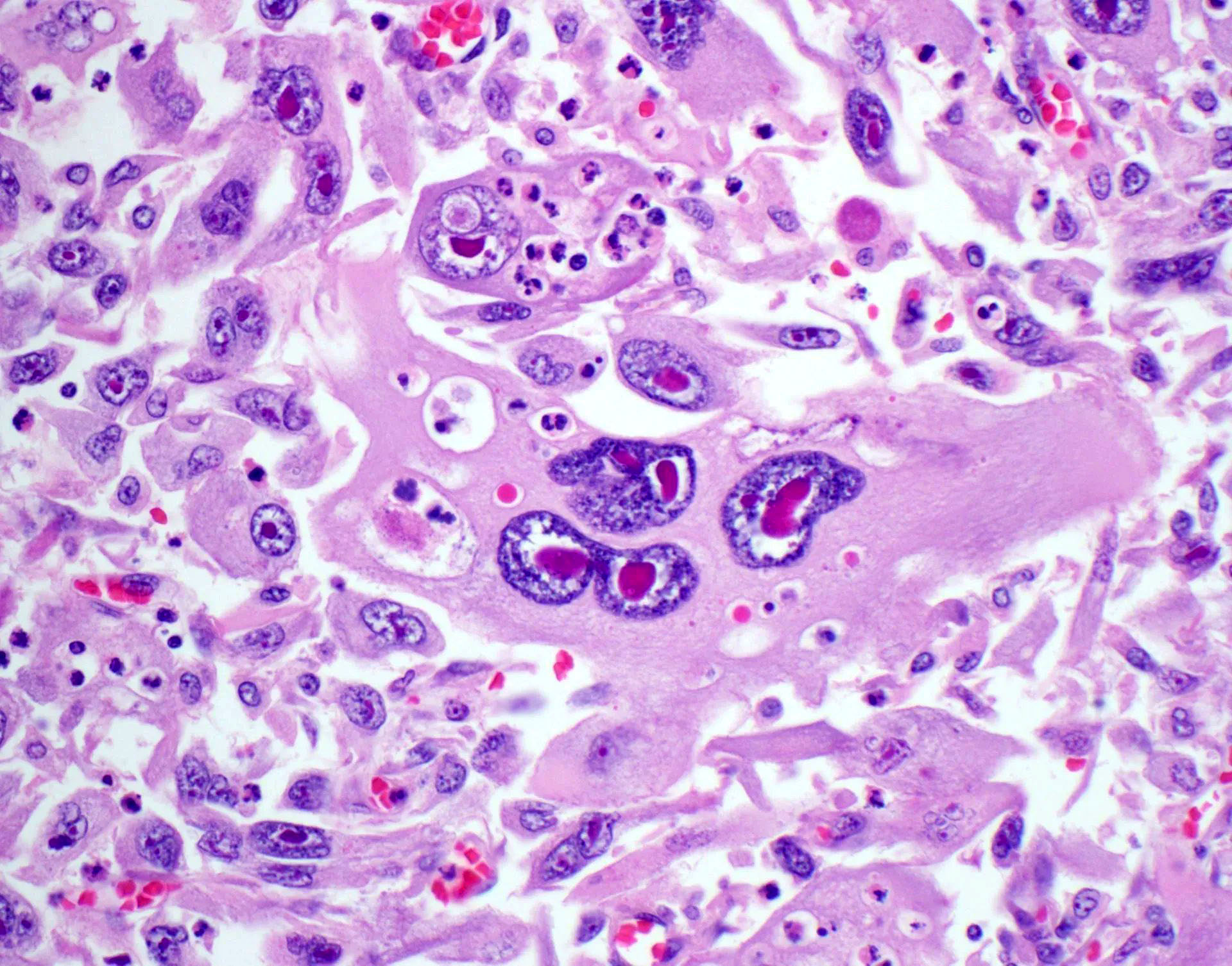
- Storiform, fascicular or patternless arrangement of highly atypical spindled, epithelioid, round or pleomorphic cells (Lindberg: Diagnostic Pathology - Soft Tissue Tumors, 2nd Edition, 2015, Ultrastruct Pathol 2008;32:31, Mod Pathol 2014;27:S39)
- Undifferentiated round cell sarcoma can be diagnosed only if distinctive gene fusions have been ruled out
- Fascicular or patternless architecture
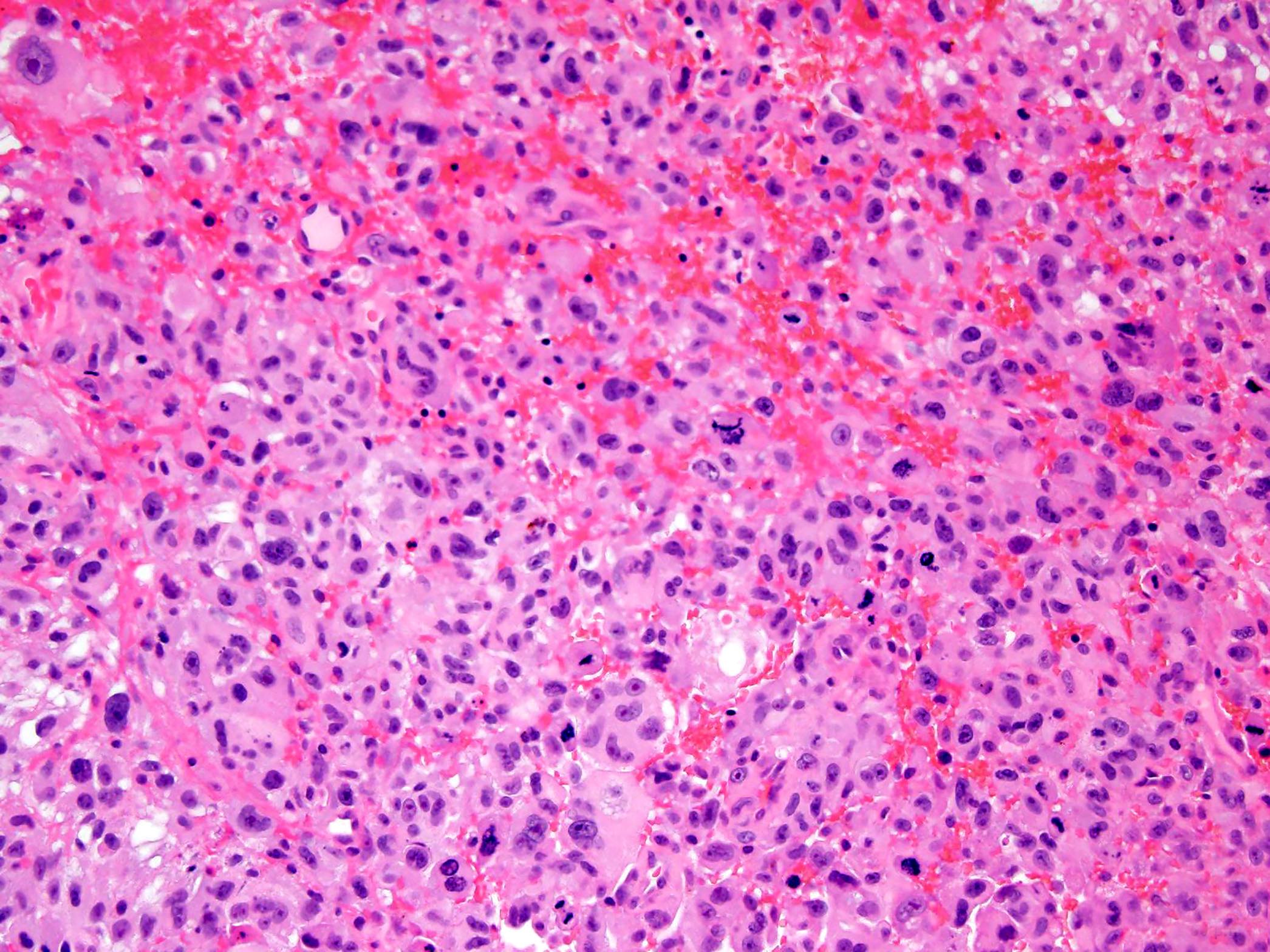
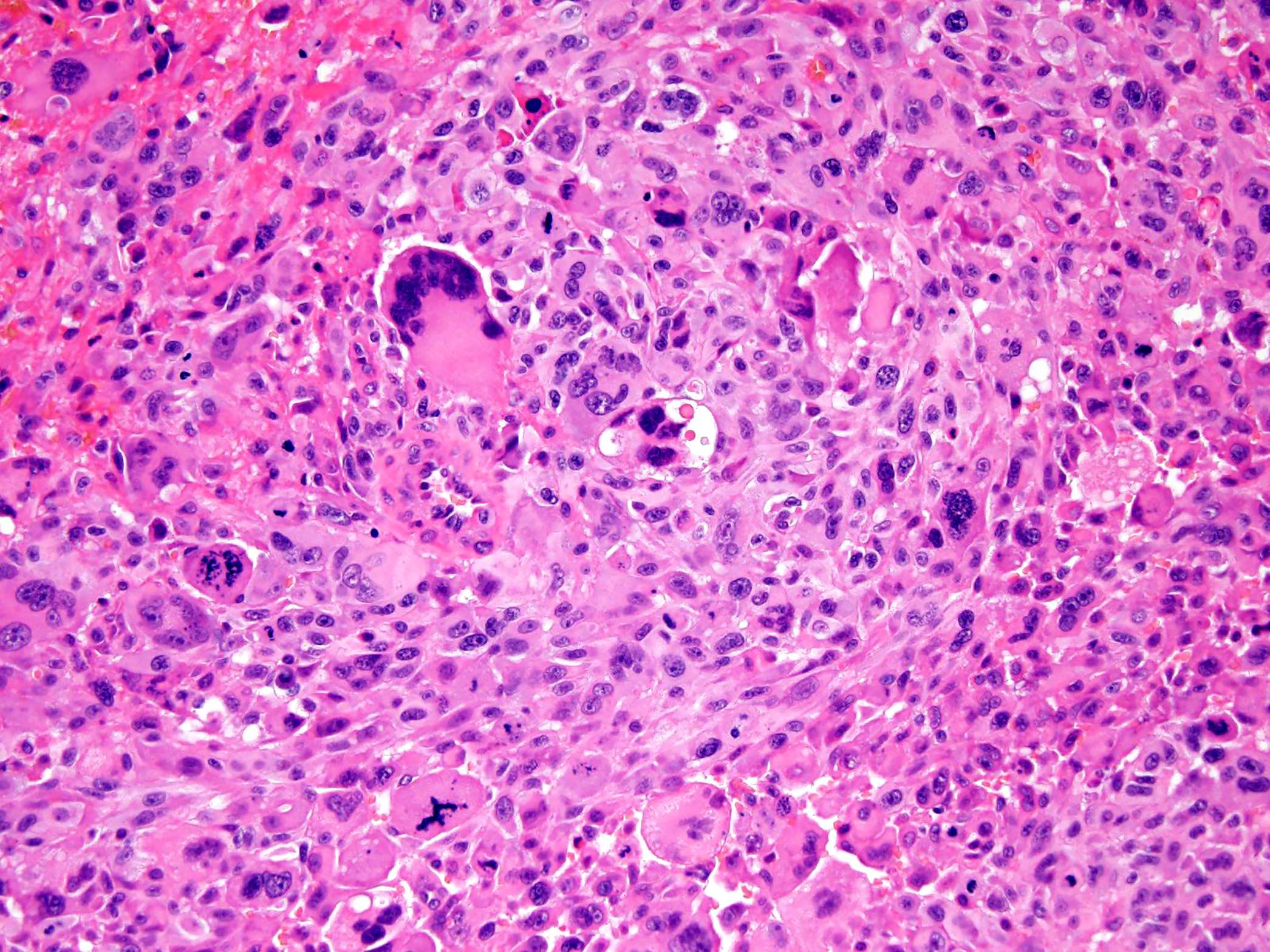
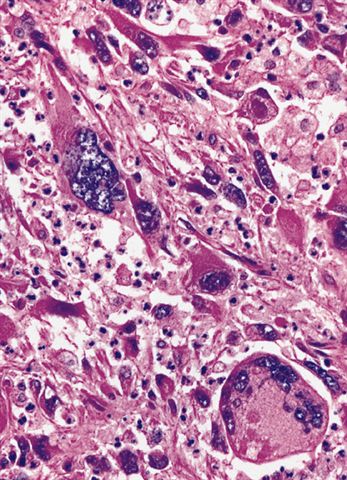
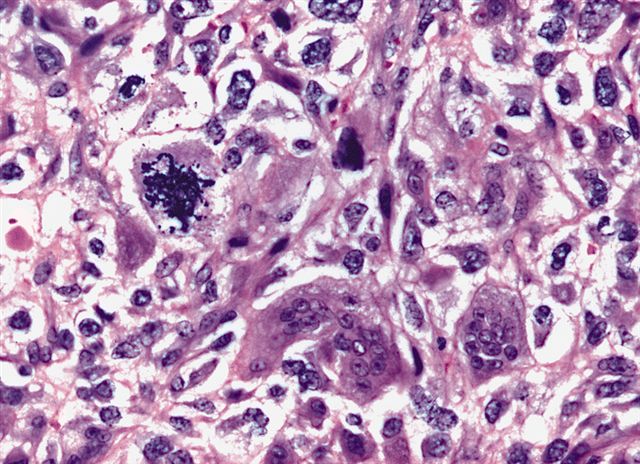
- Frequent bizarre multinucleated tumor giant cells
- Amphophilic or palely eosinophilic cytoplasm
- Hyperchromatic or vesicular nuclei
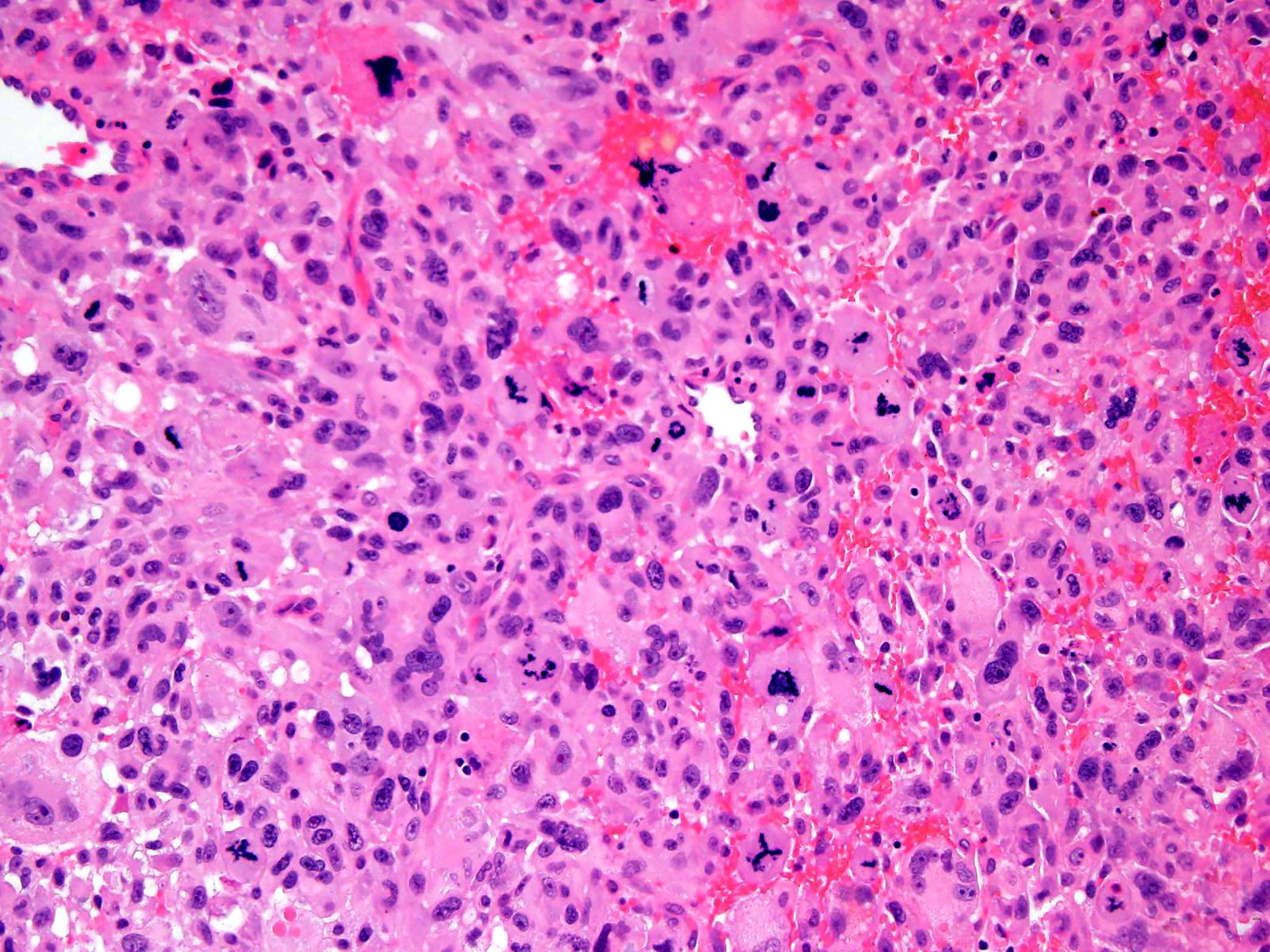
- Abundant mitoses
- Coagulative necrosis is common
Contributed by Borislav A. Alexiev, M.D., Nikhil Sangle, M.D. (Case #387), AFIP and @JMGardnerMD on Twitter
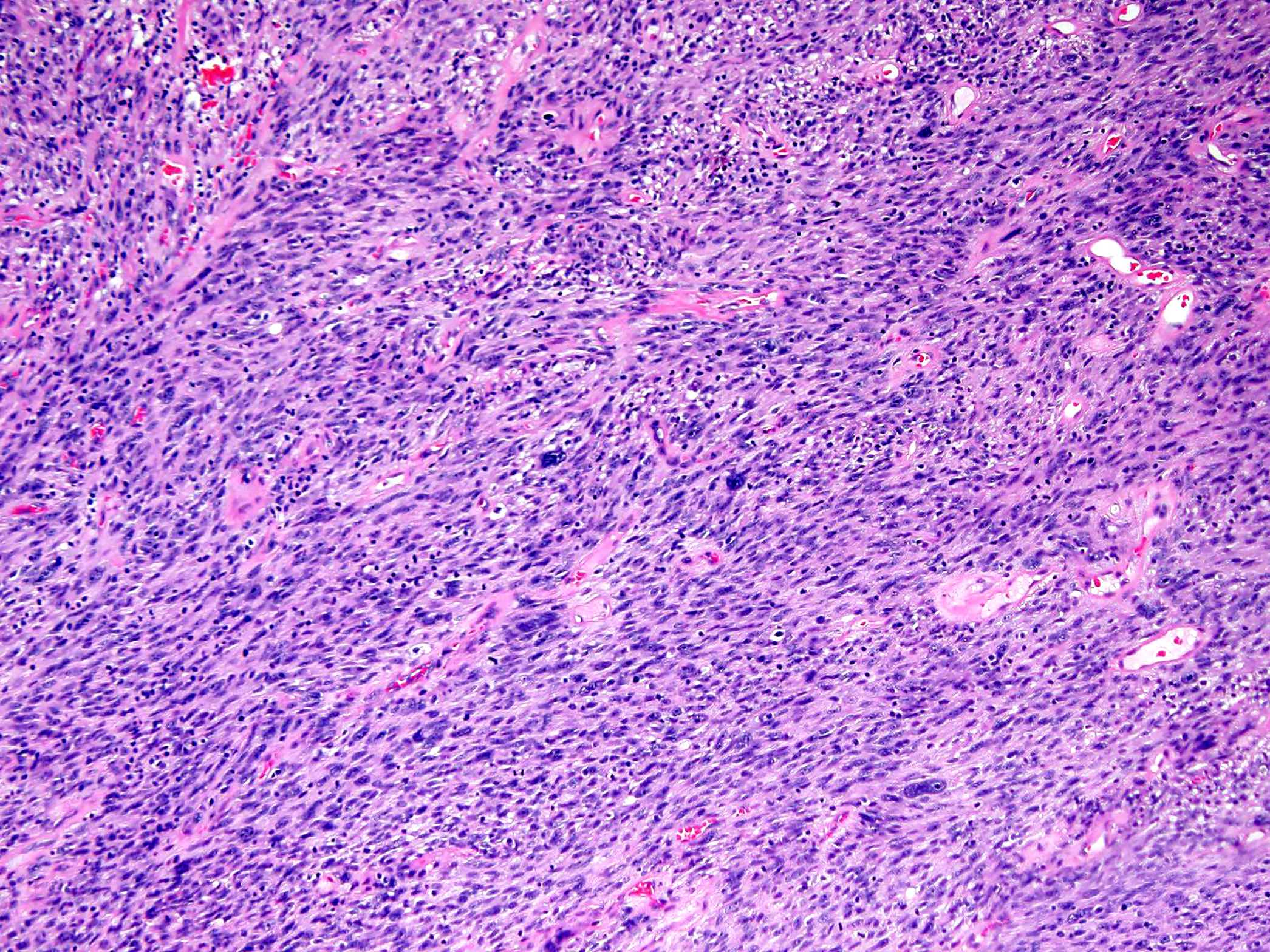
Fascicular growth pattern
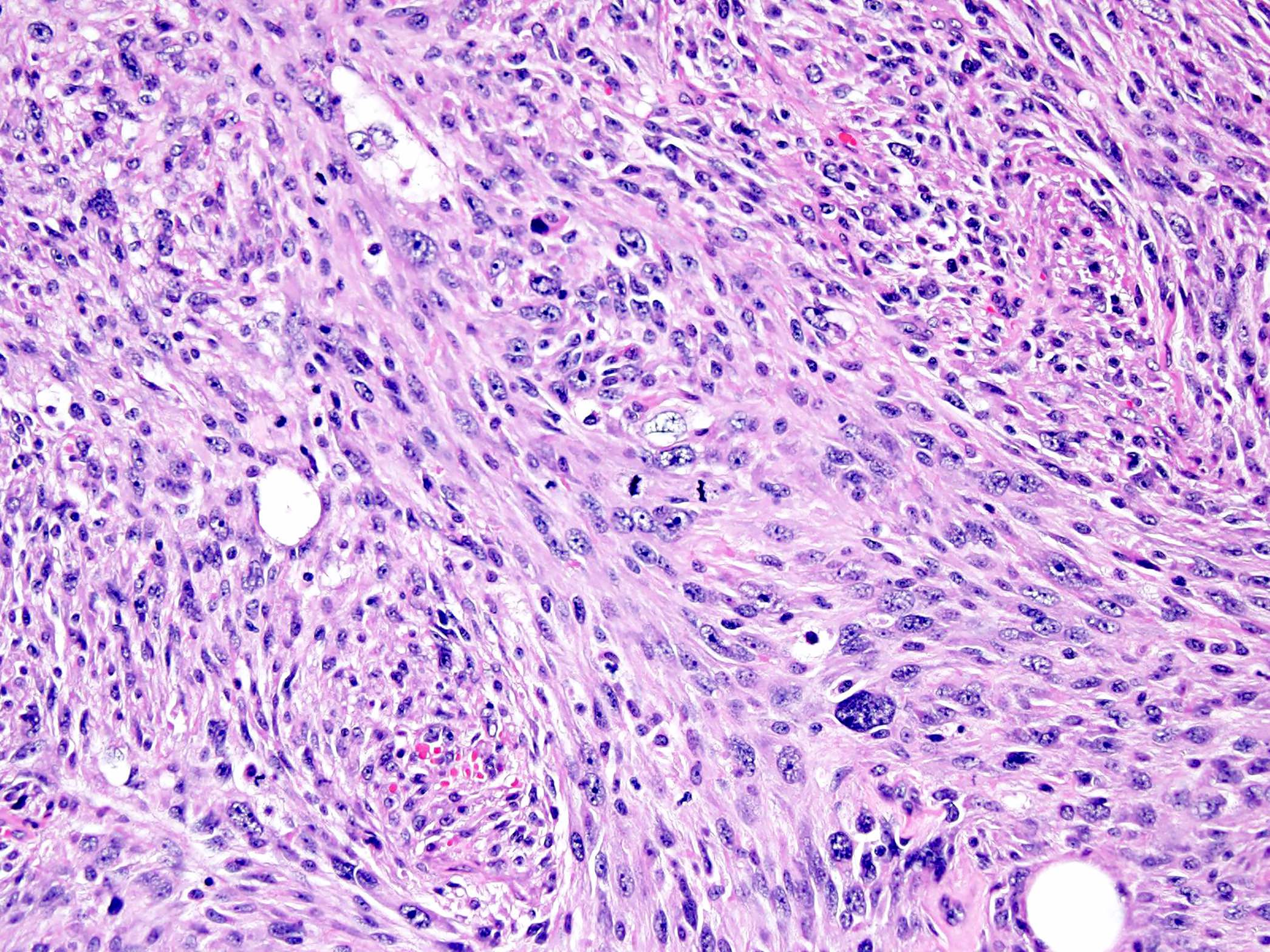
Spindle cells
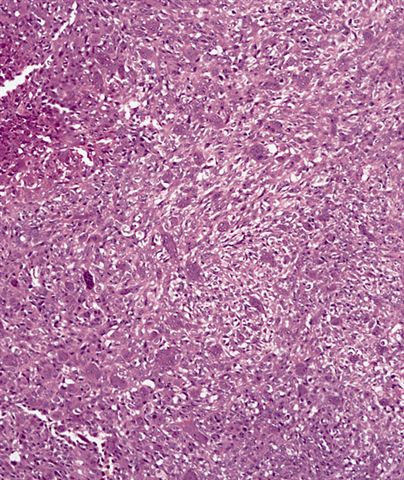
Epithelioid cells
Pleomorphic cells
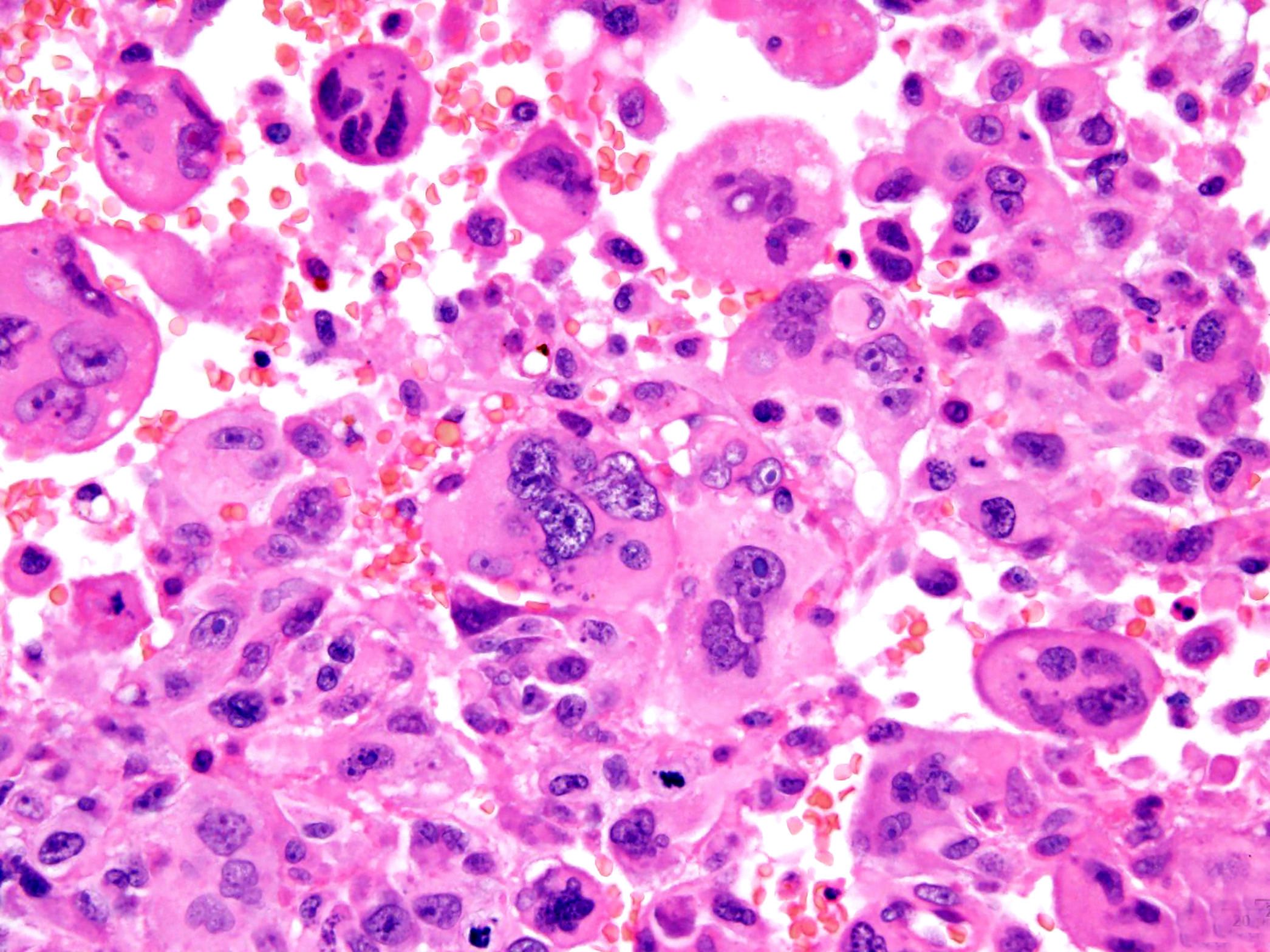
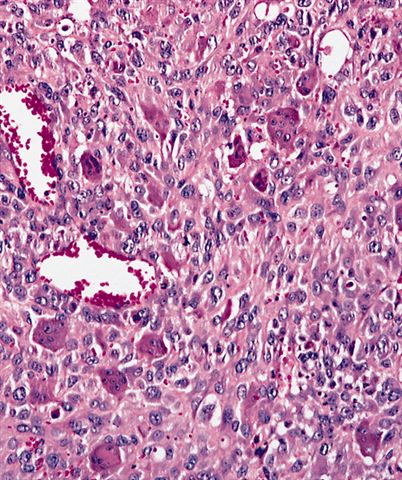
Bizarre multinucleated tumor cells
High mitotic activity
Bizarre nuclei

Abundant eosinophilic cytoplasm
Characteristic giant cells
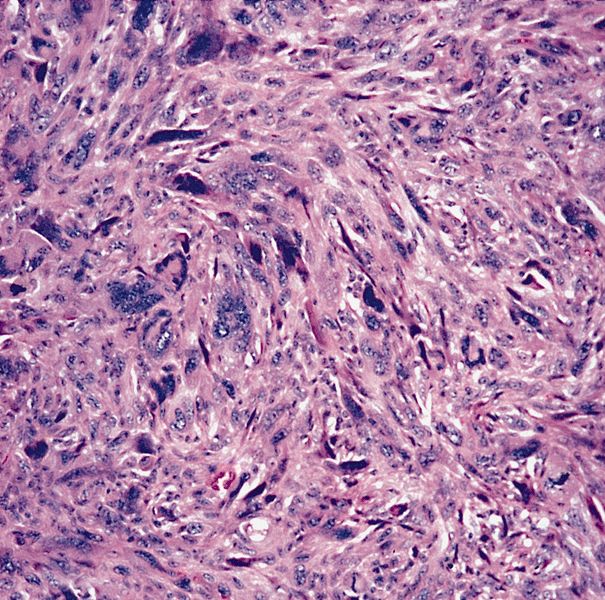
Mixture of fibroblasts and histiocyte-like cells
Vague storiform pattern
Strap-like cells
Numerous mitotic figures
Frequent tumor cell necrosis
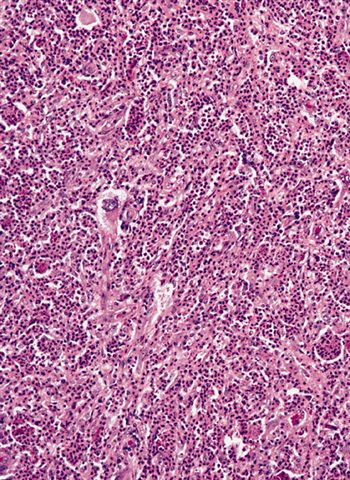
Acute inflammatory and histiocyte-like cells
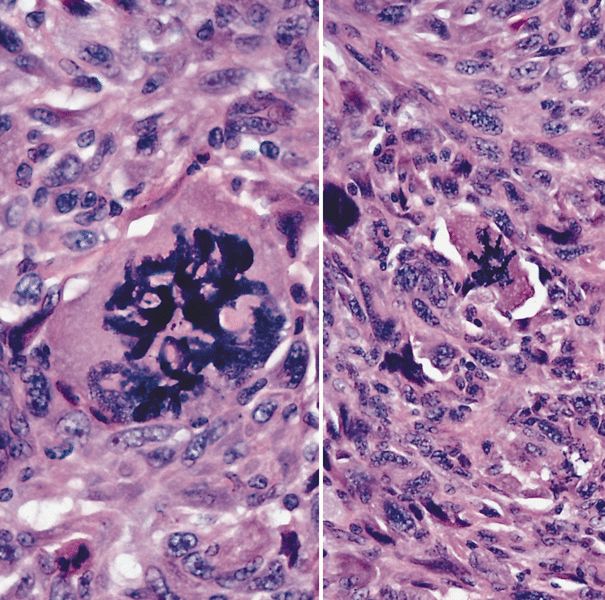
Osteoclast-like giant cells with uniform nuclei in undifferentiated pleomorphic sarcoma
Undifferentiated / unclassified sarcoma
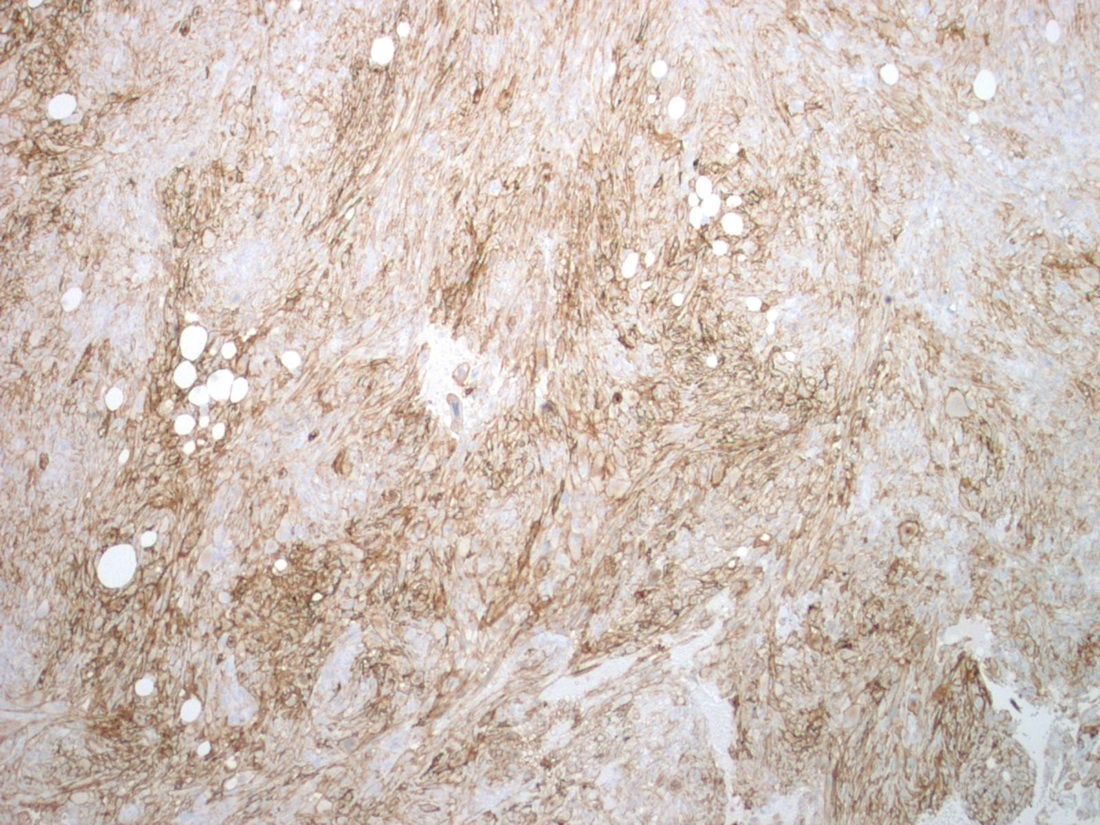
CD10+

CD68+

Vimentin+

CK-
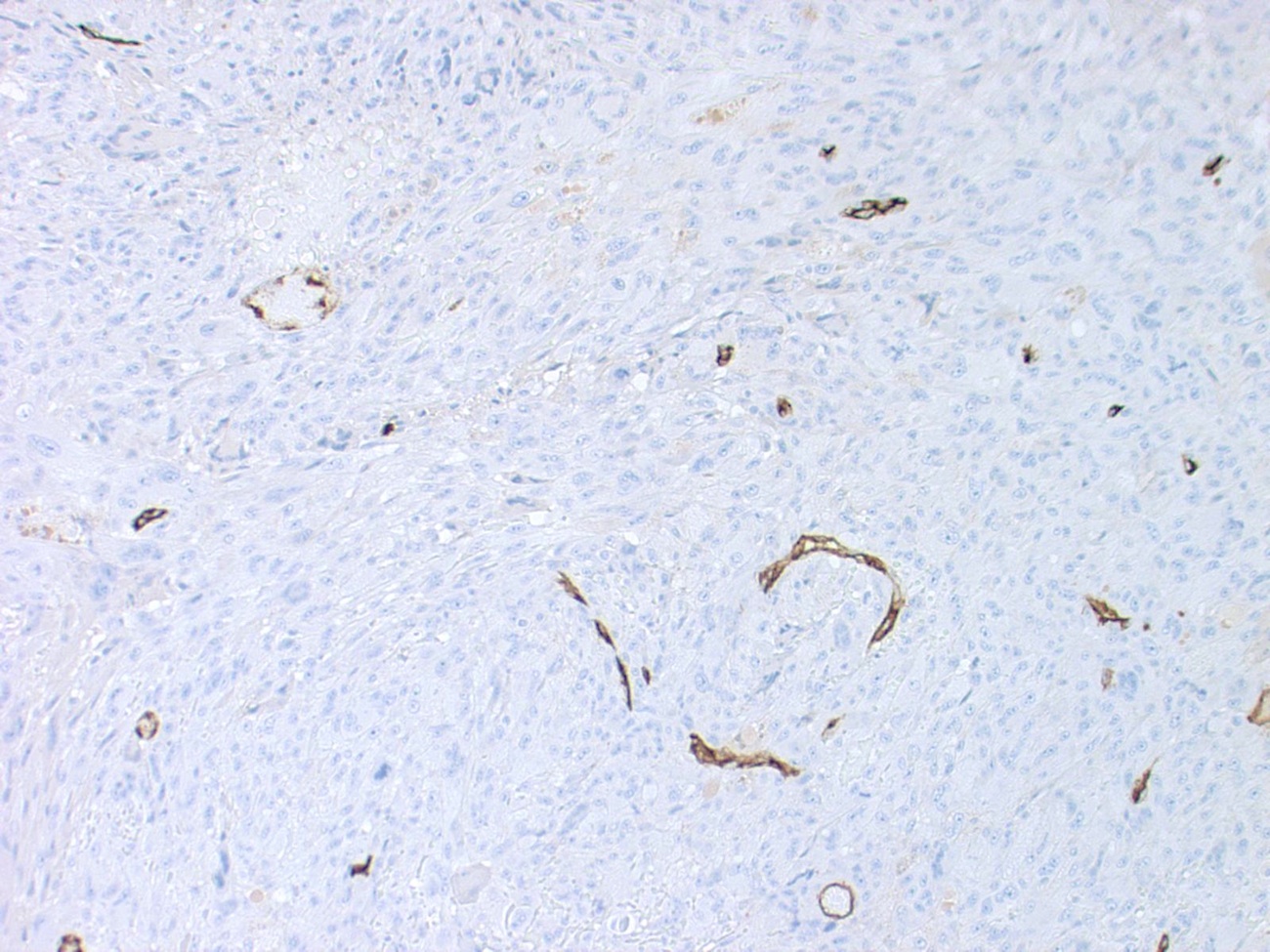
CD34-
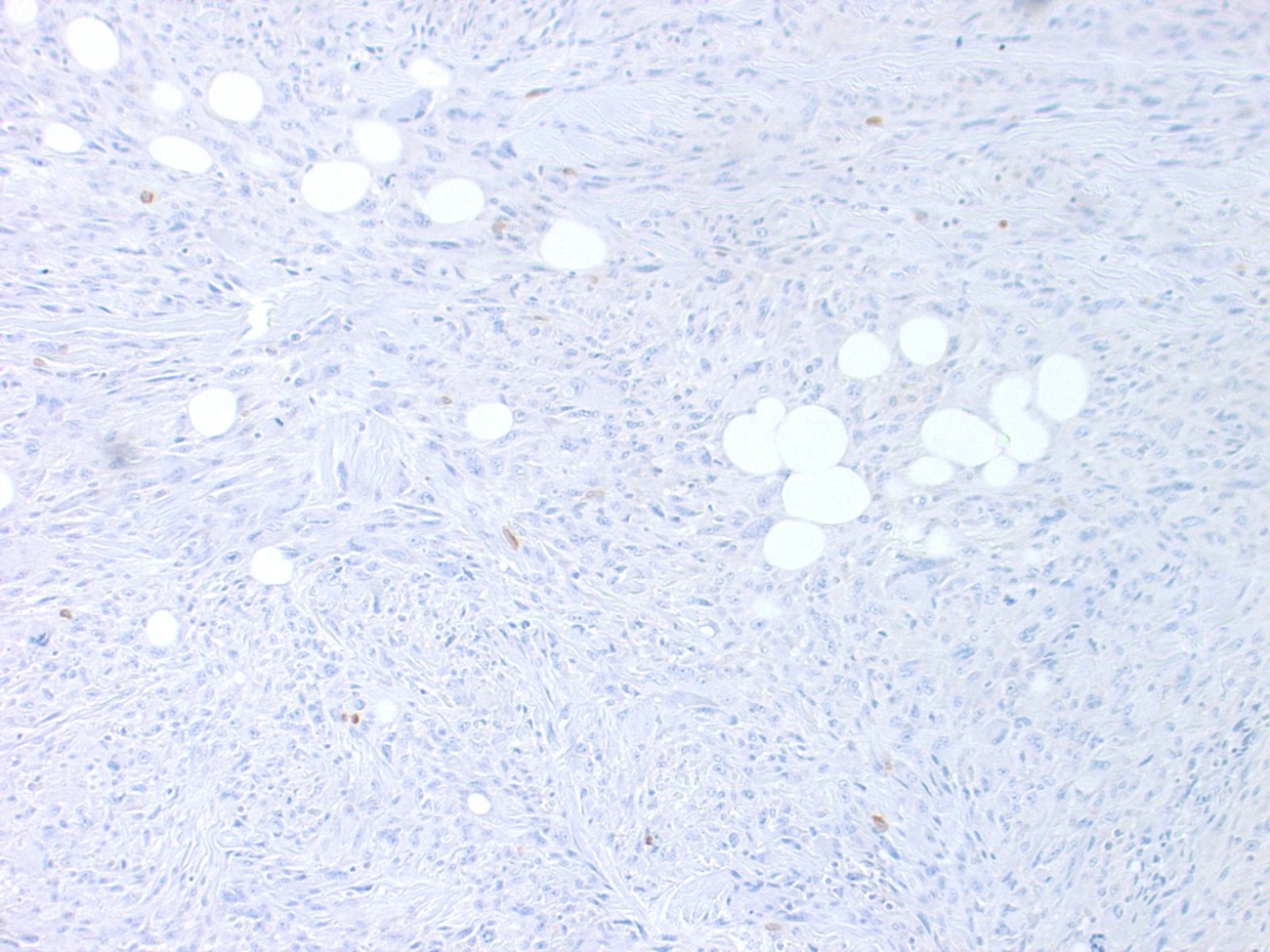
Desmin-
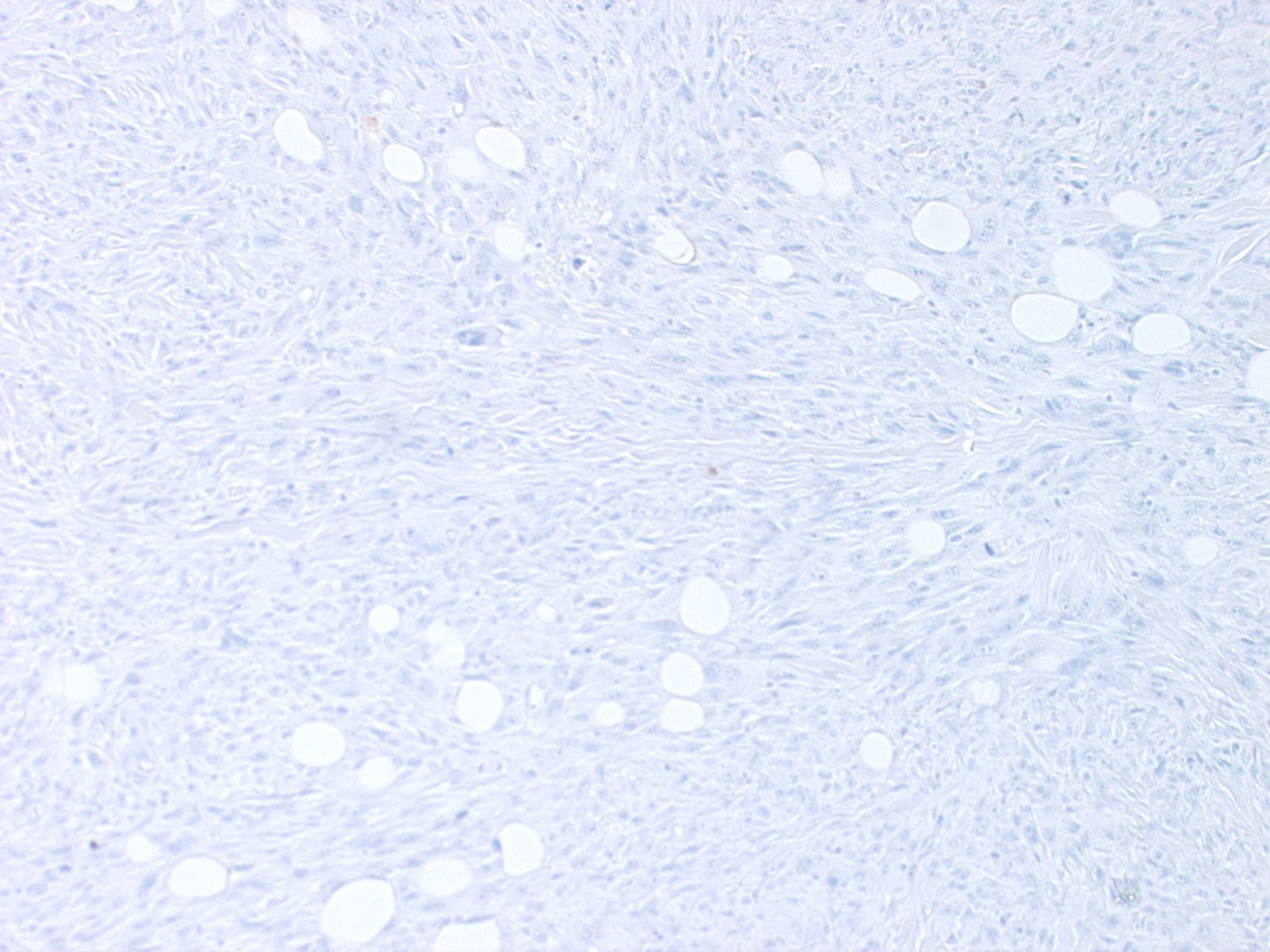
S100-
- Main advantages of soft tissue fine needle aspiration cytology (FNAC) are good sensitivity and specificity, low morbidity, speed of diagnosis and low cost / benefit ratio
- The most important disadvantages stem from limited experience in cytological diagnosis of soft tissue tumors and a lack of standardized and uniform reporting system for soft tissue FNAC (Cytopathology 2020;31:271)
- FNAC is of utility not only in primary lesions but also for metastatic tumors and for the documentation of locally recurrent soft tissue neoplasms (Diagn Cytopathol 2022;50:463, Cancer 1997;81:228)
- Although making an initial diagnosis of sarcoma by fine needle aspiration biopsy is reliable, specific subtyping of sarcomas as undifferentiated sarcoma is more problematic
- Cellular smears
- Patterns range from single cells to large storiform fragments
- Spindled, plasmacytoid, round and pleomorphic cell shapes are found; pleomorphic cells are often multinucleated
- Anisonucleosis, nuclear hyperchromasia, frequent mitoses
- Nuclear membrane irregularities, nucleoli are often prominent
Contributed by Borislav A. Alexiev, M.D.
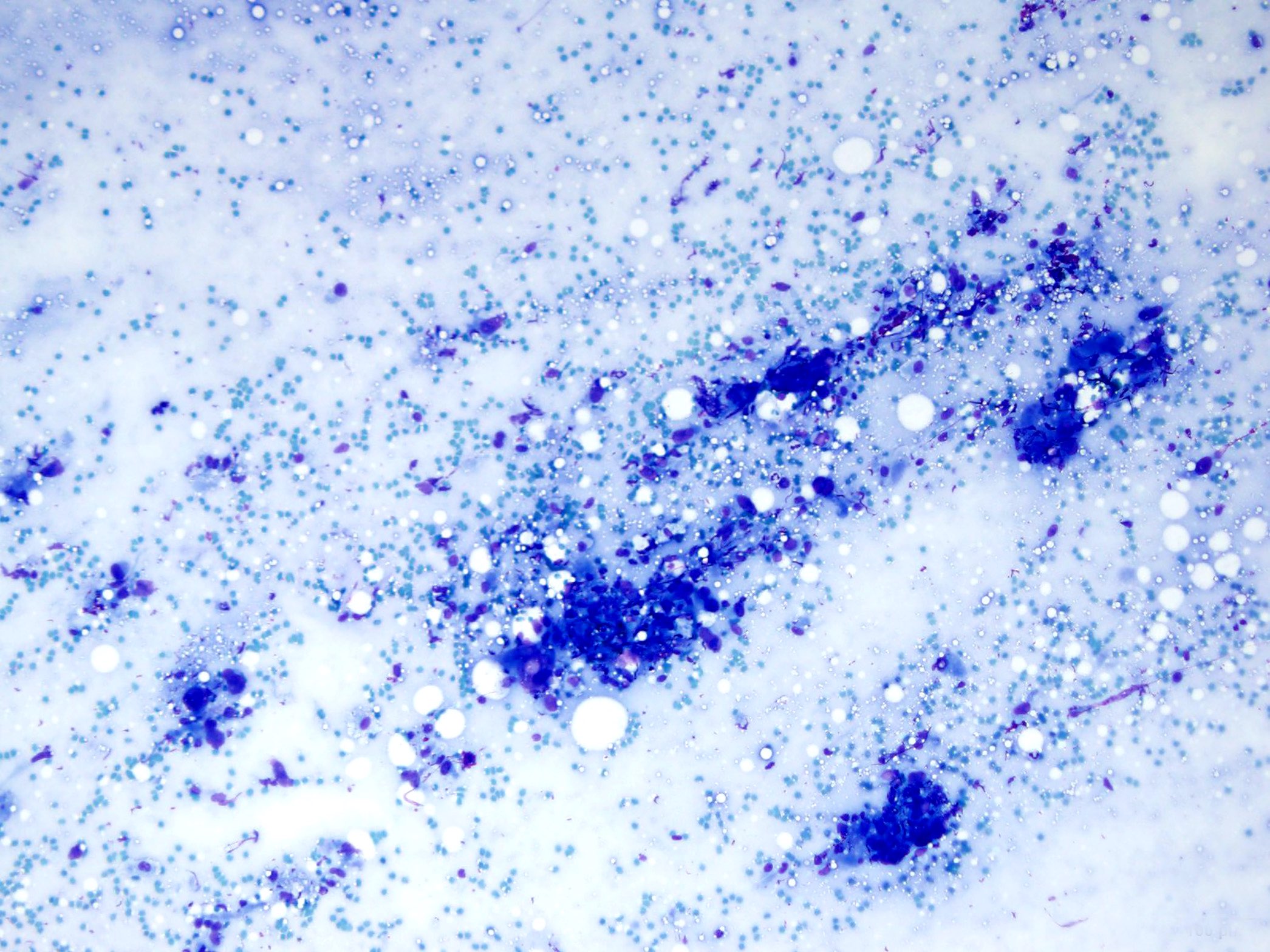
Cellular smear
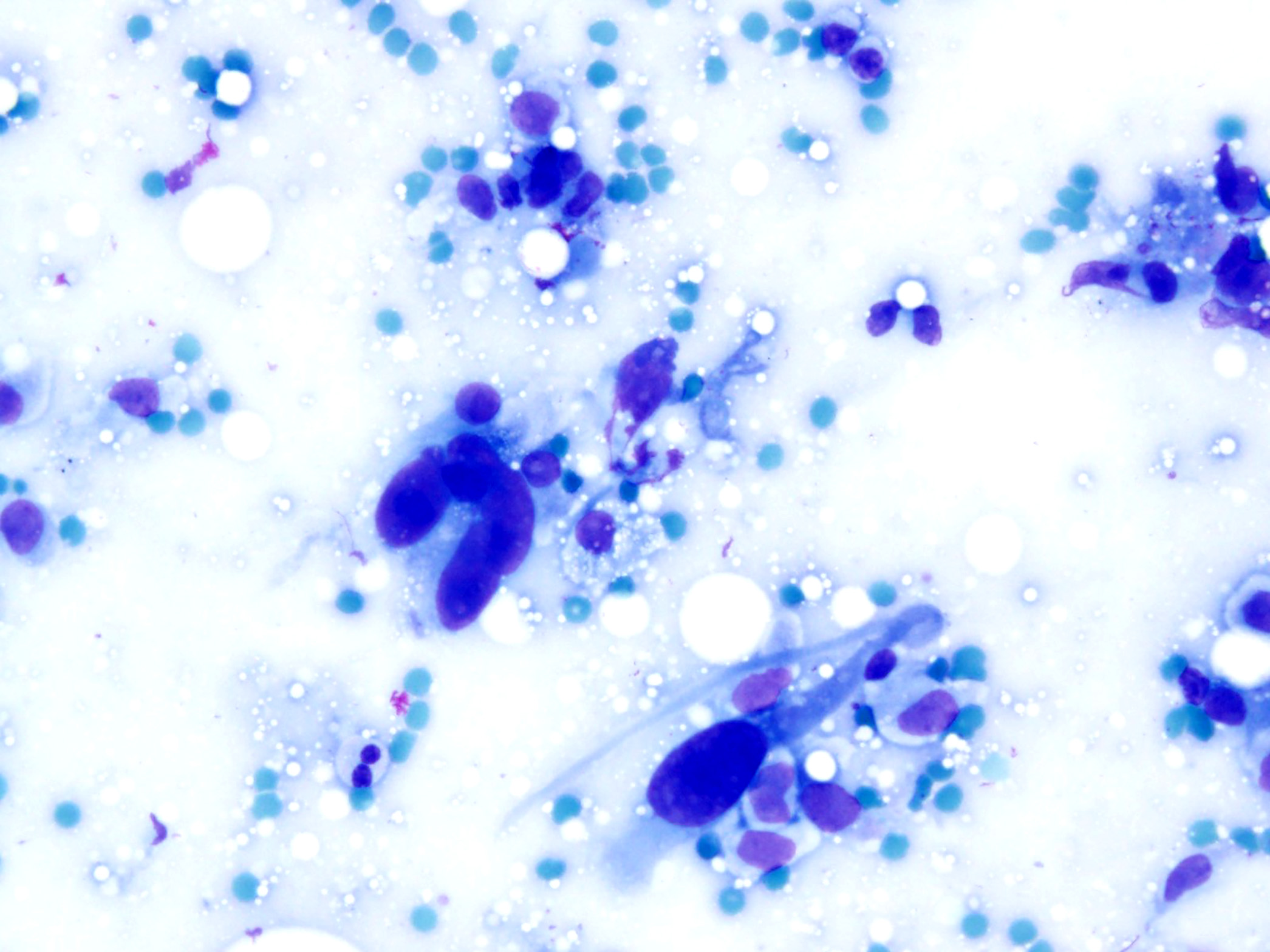
Nuclear atypia
- Role of immunohistochemistry in the diagnosis of undifferentiated sarcoma has traditionally been an ancillary one, primarily serving as a means to exclude other pleomorphic tumors (Mod Pathol 2014;27:S39)
- Can variably express CD34, smooth muscle actin (SMA) and CD68
- Focal expression of these markers is not specific and does not point toward evidence of a specific line of differentiation (Semin Diagn Pathol 2021;38:170)
- No identifiable line of differentiation when analyzed by presently available technologies (Semin Diagn Pathol 2021;38:170, Mod Pathol 2014;27:S39, Virchows Arch 2007;451:949)
- Immunohistochemistry has progressively supplanted electron microscopy as the method of choice to characterize the phenotype of neoplastic cells in soft tissue tumors and in solving most differential diagnoses (Ultrastruct Pathol 2008;32:51)
- Occasionally, in tumors with smooth muscle, skeletal muscle, adipocytic, vascular endothelial and Schwann cell differentiation, electron microscopy may help in the differential diagnosis
- Numerical and structural variants underlying chromosomal aberrations are frequently observed in undifferentiated sarcoma (Front Genet 2023;14:1109491)
- Losses of 13q12-q14 or 13q21 were observed in a large proportion of tumors, suggesting that a gene localized in this region could act as a tumor suppressor gene (Cancer Genet Cytogenet 1999;111:134)
- Comprehensive, integrated genomics shows that undifferentiated sarcoma and myxofibrosarcoma are largely indistinguishable across the multiplatform molecular landscape (Front Genet 2023;14:1109491)
- PRDM10 fusions are present in ~5% of undifferentiated sarcoma (Clin Cancer Res 2015;21:864)
- Soft tissue, left thigh, excision:
- Undifferentiated pleomorphic sarcoma, FNCLCC grade 3 (see comment)
- Comment: H&E stained tissue sections show a patternless arrangement of highly atypical spindled and polygonal cells with eosinophilic cytoplasm. There is a marked nuclear pleomorphism, including bizarre nuclei and multinucleation. Abundant mitoses with atypical forms (> 20 mitoses/10 high power fields) and focal coagulative necrosis (~20%) are seen.
- Immunohistochemical stains for vimentin and CD68 are positive in tumor cells, while all of the following are negative: keratin AE1 / AE3, MelanA, SOX10, desmin, h-caldesmon, ALK1, CD30, MyoD1 and myogenin. H3K27me3 expression is retained. FISH is negative for MDM2 amplification. The findings support the diagnosis of undifferentiated sarcoma.
- Dedifferentiated liposarcoma:
- Relatively common in retroperitoneum
- True undifferentiated sarcomas are very rare in retroperitoneum
- May have a component of well differentiated liposarcoma
- MDM2 amplification by FISH (Am J Clin Pathol 2014;141:334)
- Relatively common in retroperitoneum
- Pleomorphic leiomyosarcoma:
- Morphologic features characteristic of classic leiomyosarcoma are present
- Positive for muscle markers (SMA, desmin, h-caldesmon) (Am J Surg Pathol 2001;25:1030)
- Pleomorphic rhabdomyosarcoma:
- Rhabdoid cells with eosinophilic cytoplasm
- Positive for MyoD1 and myogenin (Mod Pathol 2001;14:595)
- High grade myxofibrosarcoma:
- High grade lesions also focally show features of lower grade neoplasm, with prominent myxoid matrix and numerous curvilinear capillaries
- Approximately half of cases occur in dermal / subcutaneous tissue (WHO 5th edition)
- High grade malignant peripheral nerve sheath tumor (MPNST):
- Sarcomatoid carcinoma:
- Can be excluded through clinical history and anatomic location
- Expression of epithelial markers, such as keratin AE1 / AE3 and p63 (Int J Clin Exp Pathol 2008;1:524)
- Malignant melanoma:
- Can be excluded through clinical history and anatomic location
- Expression of melanoma markers, such as MelanA, HMB45 and SOX10 (J Cutan Pathol 2008;35:433)
- Anaplastic large cell lymphoma:
Which of the following is true for undifferentiated soft tissue sarcomas?
- Areas with prominent myxoid matrix and numerous curvilinear capillaries are common
- Complex and nonspecific cytogenetic abnormalities
- Most arise in the retroperitoneum
- Tumor cells often display cross striations
- Usually are tumors of children
Comment Here
Reference: Undifferentiated / unclassified sarcoma
- Chicken wire calcifications
- Lipoblasts
- Neoplastic bone formation
- Nuclear pleomorphism
- Tumor cells often display cross striations
Comment Here
Reference: Undifferentiated / unclassified sarcoma
