Soft tissue
Peripheral nerve
Other benign
Neuroma
Resident / Fellow Advisory Board: Josephine Kam Tai Dermawan, M.D., Ph.D.
Deputy Editor-in-Chief: Borislav A. Alexiev, M.D.


Last author update: 19 October 2022
Last staff update: 20 October 2022
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Neuroma soft tissue
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Videos | Sample pathology report | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1Cite this page: Anjum S, Ahmed R, Ud Din N. Neuroma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/softtissueneuroma.html. Accessed September 18th, 2025.
Definition / general
- Benign, nonneoplastic, normal, chronic, reparative, proliferative response composed of disorganized nerve fiber bundles, fibrous stroma, Schwann cells, perineural cells, axons and endoneurial fibroblasts (Medicine (Baltimore) 2019;98:e15142, Acta Biomed 2020;91:122, J Orthop Case Rep 2019;9:10, Plast Reconstr Surg Glob Open 2020;8:e2792, World J Clin Cases 2020;8:3821, J Orthop Case Rep 2020;10:28, Plast Reconstr Surg Glob Open 2018;6:e1952, StatPearls: Neuroma [Accessed 21 September 2022])
- Secondary nerve damage occurring after trauma (acute or chronic) or surgery (Acta Biomed 2020;91:122, World J Clin Cases 2020;8:3821, Plast Reconstr Surg Glob Open 2018;6:e1952, Medicine (Baltimore) 2019;98:e15142, Plast Reconstr Surg Glob Open 2020;8:e2545, StatPearls: Neuroma [Accessed 21 September 2022])
Essential features
- Benign, circumscribed, often painful lesion developing after trauma or surgical amputation of the limb
- Composed of disorganized spindle cell proliferation of nerve components
Terminology
- Traumatic neuroma / amputation neuroma / stump neuroma (Acta Biomed 2020;91:122, Plast Reconstr Surg Glob Open 2018;6:e1952, Medicine (Baltimore) 2019;98:e15142, Plast Reconstr Surg Glob Open 2020;8:e2545, StatPearls: Neuroma [Accessed 21 September 2022])
ICD coding
- ICD-10: T87.30 - neuroma of amputation stump, unspecified extremity
Epidemiology
- No predilection for a specific age, gender, or geographic location
- Usually associated with history of trauma, amputation or chronic friction
Sites
- Commonly affects lower extremities and head and neck (Medicine (Baltimore) 2019;98:e15142, Acta Biomed 2020;91:122)
- Other uncommon sites are ulnar nerve, radial nerve, brachial plexus (Acta Biomed 2020;91:122)
Pathophysiology
- Injury to perineurium and subsequent neuroinflammation, followed by disorganization of the neurogenic tissue due to a multidirectional proliferation of cells in an abortive attempt to repair the injured nerve (Acta Biomed 2020;91:122, J Orthop Case Rep 2019;9:10, Plast Reconstr Surg Glob Open 2020;8:e2792, J Orthop Case Rep 2020;10:28, Plast Reconstr Surg Glob Open 2018;6:e1952, StatPearls: Neuroma [Accessed 21 September 2022])
- Associated pain may be due to traction, compression, sensitive nerve endings, ischemia, ectopic foci of ion channels, increasing levels of nerve growth factor, alpha smooth muscle actin, cannabinoid CB2 receptor and unmyelinated fiber and changes in peripheral and central sensitization (Medicine (Baltimore) 2019;98:e15142, J Orthop Case Rep 2019;9:10)
Etiology
- Trauma, amputation or chronic friction (Acta Biomed 2020;91:122, World J Clin Cases 2020;8:3821, Plast Reconstr Surg Glob Open 2018;6:e1952, StatPearls: Neuroma [Accessed 21 September 2022])
- Terminal neuroma is a normal pattern of nerve healing and is asymptomatic (Acta Biomed 2020;91:122, J Orthop Case Rep 2019;9:10)
- Spindle neuroma results from chronic stimulation, friction and microtrauma (Acta Biomed 2020;91:122, J Orthop Case Rep 2019;9:10)
Clinical features
- Sharp / burning pain, paresthesia, numbness, cold intolerance, electrical sensitivity with no signs of inflammation (Plast Reconstr Surg Glob Open 2018;6:e1952, Plast Reconstr Surg Glob Open 2020;8:e2545, Acta Biomed 2020;91:122, Plast Reconstr Surg Glob Open 2020;8:e2792, J Orthop Case Rep 2020;10:28, StatPearls: Neuroma [Accessed 21 September 2022])
- Presents 1 - 12 months after trauma / surgery (Acta Biomed 2020;91:122, Open Orthop J 2009;3:125, J Orthop Case Rep 2019;9:10, J Orthop Case Rep 2020;10:28, Plast Reconstr Surg Glob Open 2018;6:e1952)
Diagnosis
- Careful history (Plast Reconstr Surg Glob Open 2018;6:e1952, StatPearls: Neuroma [Accessed 21 September 2022])
- Physical examination will reveal a well defined palpable firm lump
- Positive Tinel sign (Acta Biomed 2020;91:122, J Orthop Case Rep 2020;10:28, Plast Reconstr Surg Glob Open 2018;6:e1952, Plast Reconstr Surg Glob Open 2020;8:e2545, StatPearls: Neuroma [Accessed 21 September 2022])
- Block test with lidocaine can be performed (shown to be positive) (J Orthop Case Rep 2020;10:28)
Laboratory
- There are no laboratory tests that aid in diagnosis (World J Clin Cases 2020;8:3821, StatPearls: Neuroma [Accessed 21 September 2022])
Radiology description
- Ultrasound: circumscribed, marginated, homogeneously hypoechoic fusiform mass with echogenic strands inside; bulbous end morphology; and in continuity with a normal nerve proximally (Acta Biomed 2020;91:122)
- MRI: well defined, ovoid lesion with an intermediate signal intensity on T1 weighted images; intermediate - high signal intensity with fascicular pattern on fast spin echo (FSE) T2 weighted images (Acta Biomed 2020;91:122)
Radiology images
Images hosted on other servers:


2 oval, well circumscribed parallel nodules

Sciatic neuroma: T1 sagittal plane, T2 coronal plane


Homogeneous hypoechoic fusiform mass in continuity with nerve

MRI: well defined ovoid subcutaneous mass
Prognostic factors
- Good prognosis; spread or metastasis is extremely rare (StatPearls: Neuroma [Accessed 21 September 2022])
Case reports
- 20 year old man with neuroma pain after anterior tibial tuberosity exostectomy (J Orthop Case Rep 2019;9:10)
- 34 year old man with postamputation neuroma in a patient with epithelioid sarcoma (Acta Biomed 2020;91:122)
- 58 and 71 year old women with traumatic neuroma in mastectomy scar (Medicine (Baltimore) 2019;98:e15142)
- 67 year old man with late presentation of recurrent symptomatic amputation neuroma (J Orthop Case Rep 2020;10:28)
- 72 year old man with traumatic neuroma of the remnant cystic duct (World J Clin Cases 2020;8:3821)
Treatment
- Nonsurgical management: pain medications, oral gamma aminobutyric acid analogs, physical therapy modalities, transcutaneous electrical nerve stimulation and oral antidepressant medications
- Local anesthetic and corticosteroid injections, transcutaneous electrical nerve stimulation (Plast Reconstr Surg Glob Open 2018;6:e1952, J Orthop Case Rep 2019;9:10, Plast Reconstr Surg Glob Open 2020;8:e2792, J Orthop Case Rep 2020;10:28, StatPearls: Neuroma [Accessed 21 September 2022])
- Surgical options include capping with silicone, epineural grafts, suture ligature, transposition into muscle, bone, vein graft, and traction neurectomy nerve to nerve anastomosis (Plast Reconstr Surg Glob Open 2020;8:e2792, J Orthop Case Rep 2020;10:28)
Clinical images
Images hosted on other servers:

Circumscribed subepithelial lesion

Bulbous portion of sciatic nerve

Fusiform portion of nerve
Gross description
- Regular circumscribed nodule (Medicine (Baltimore) 2019;98:e15142, World J Clin Cases 2020;8:3821)
Gross images
Images hosted on other servers:

Resected hard duodenal wall lesion
Microscopic (histologic) description
- Circumscribed, unencapsulated spindle cell proliferation arranged in short bundles comprised of axons, Schwann cells, endoneurial cells and perineurial cells (World J Clin Cases 2020;8:3821, Acta Biomed 2020;91:122, StatPearls: Neuroma [Accessed 21 September 2022])
- Peripheral palisading is not present (World J Clin Cases 2020;8:3821)
- Prominent scar tissue with dense collagen may be present (Acta Biomed 2020;91:122, StatPearls: Neuroma [Accessed 21 September 2022])
- Dystrophic calcifications are rarely present (Acta Biomed 2020;91:122)
Microscopic (histologic) images
Contributed by Nasir Ud Din, M.B.B.S.
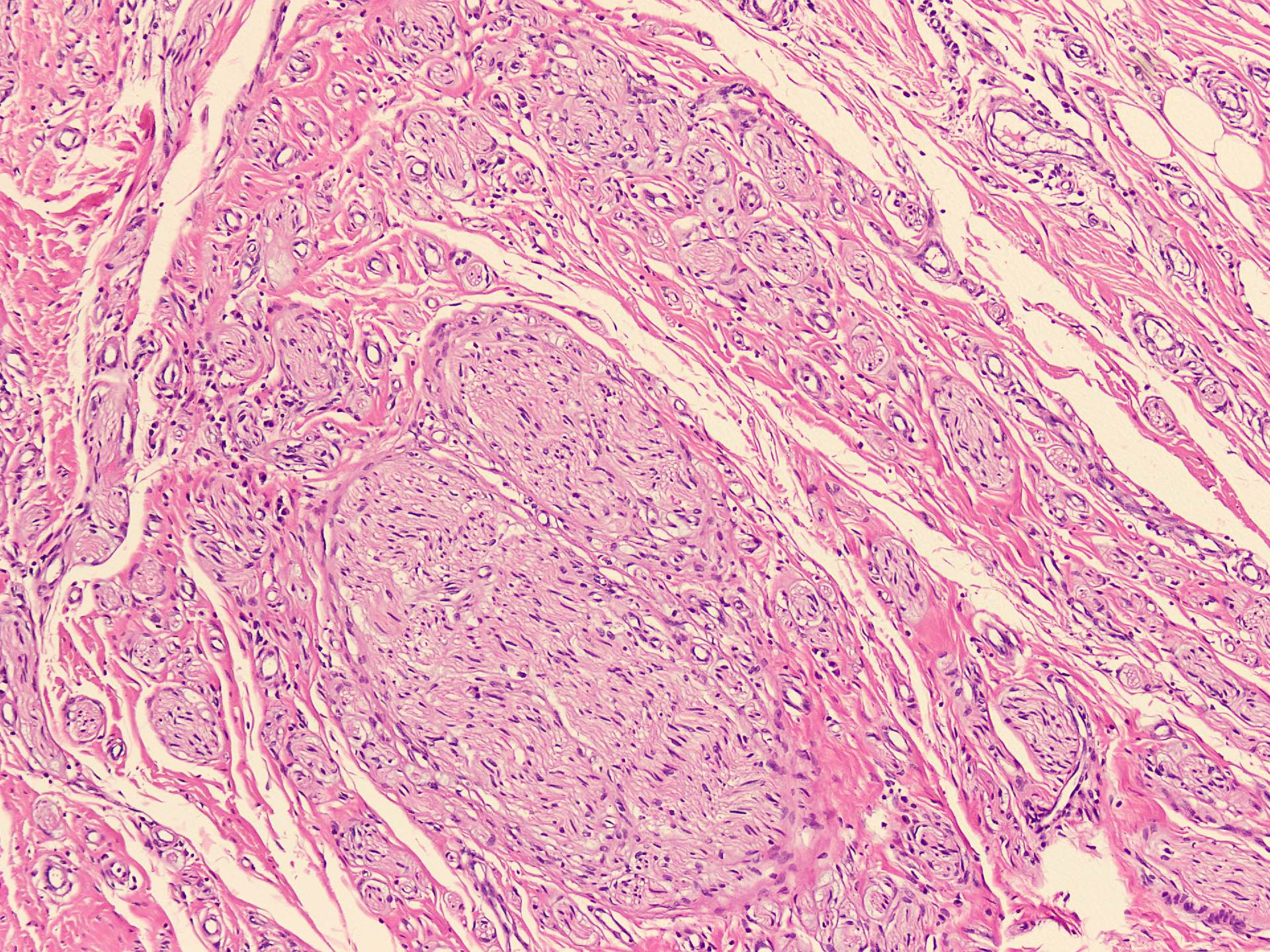
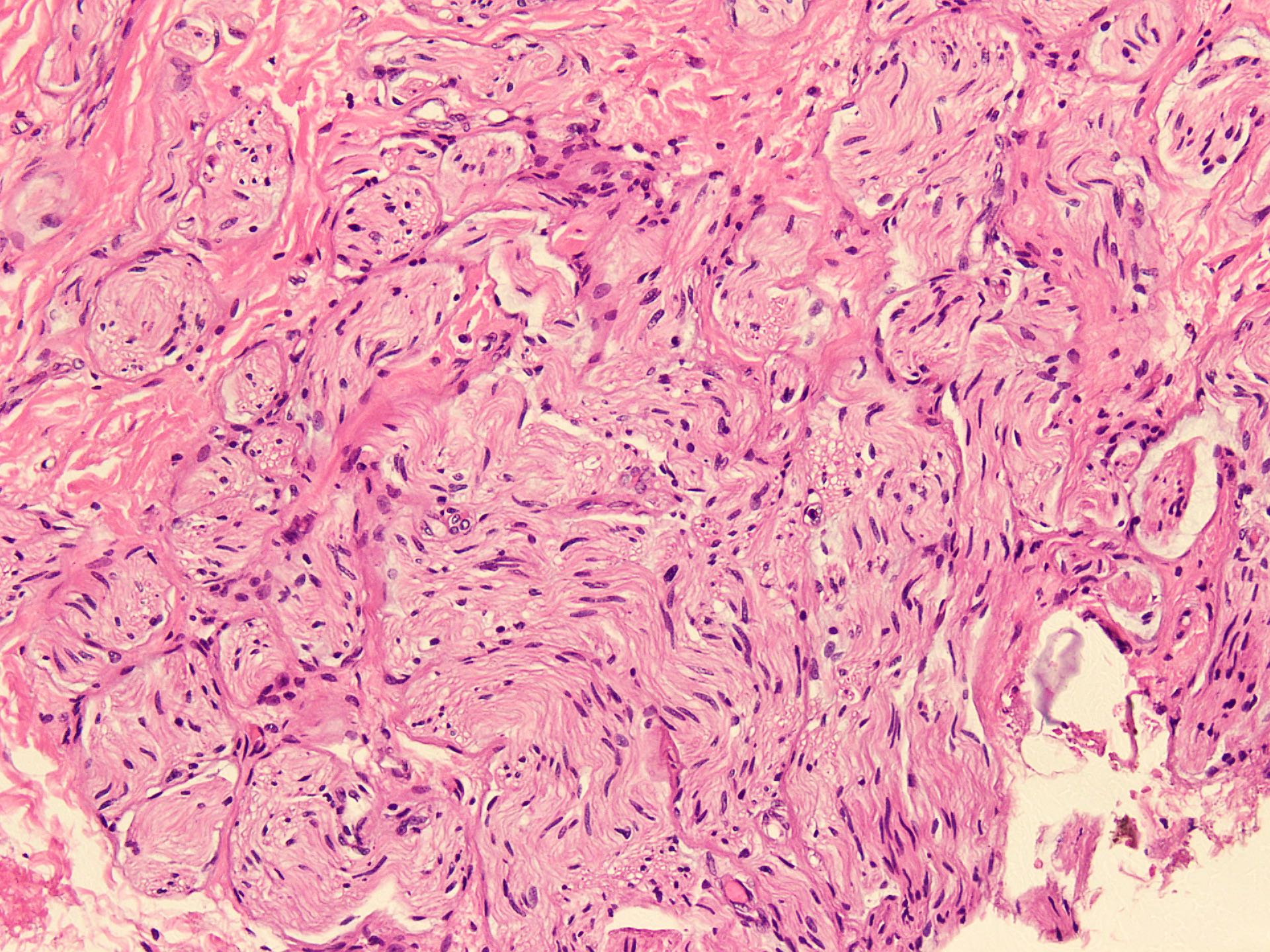
Unencapsulated bundles of spindle cells
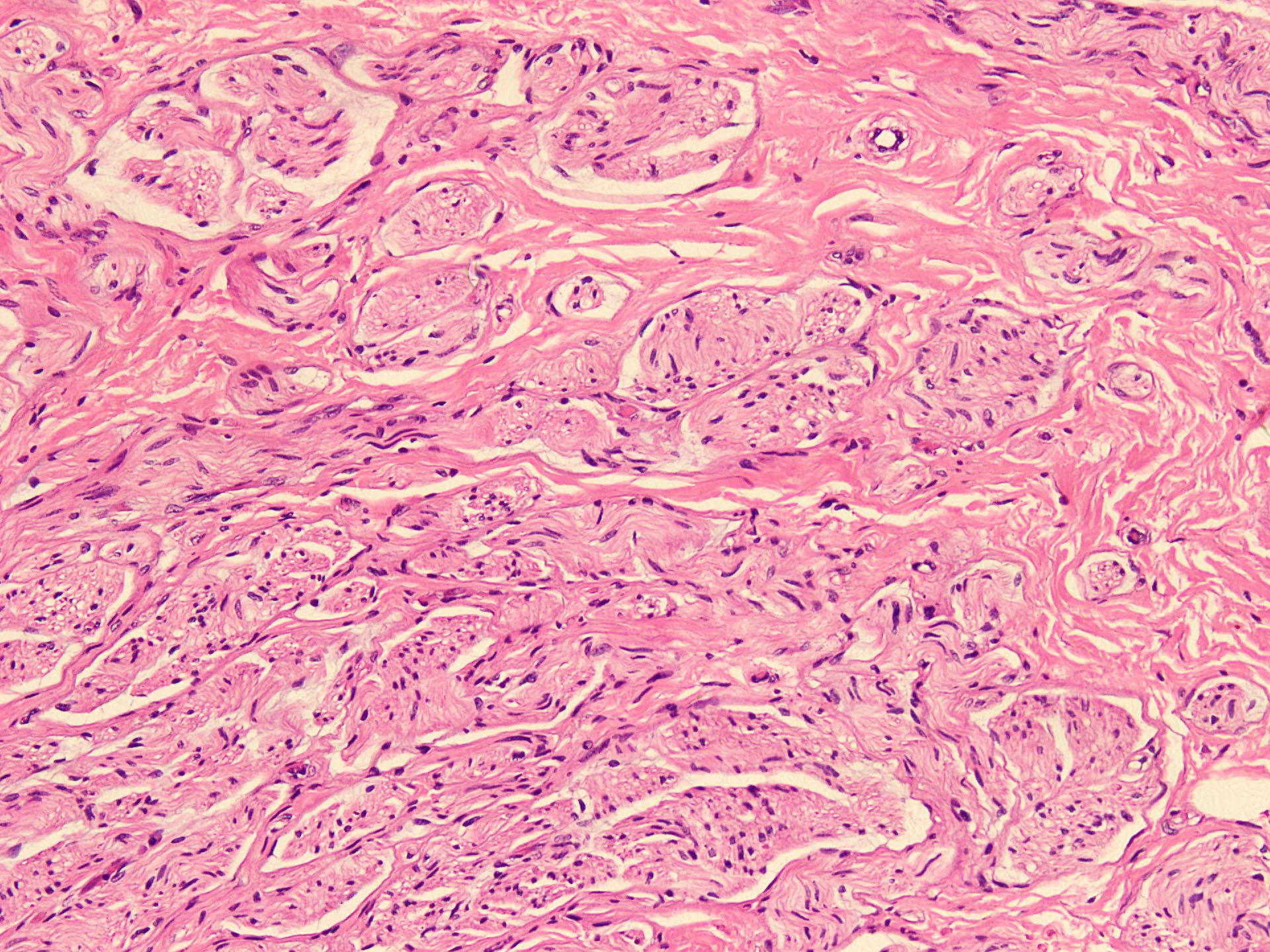
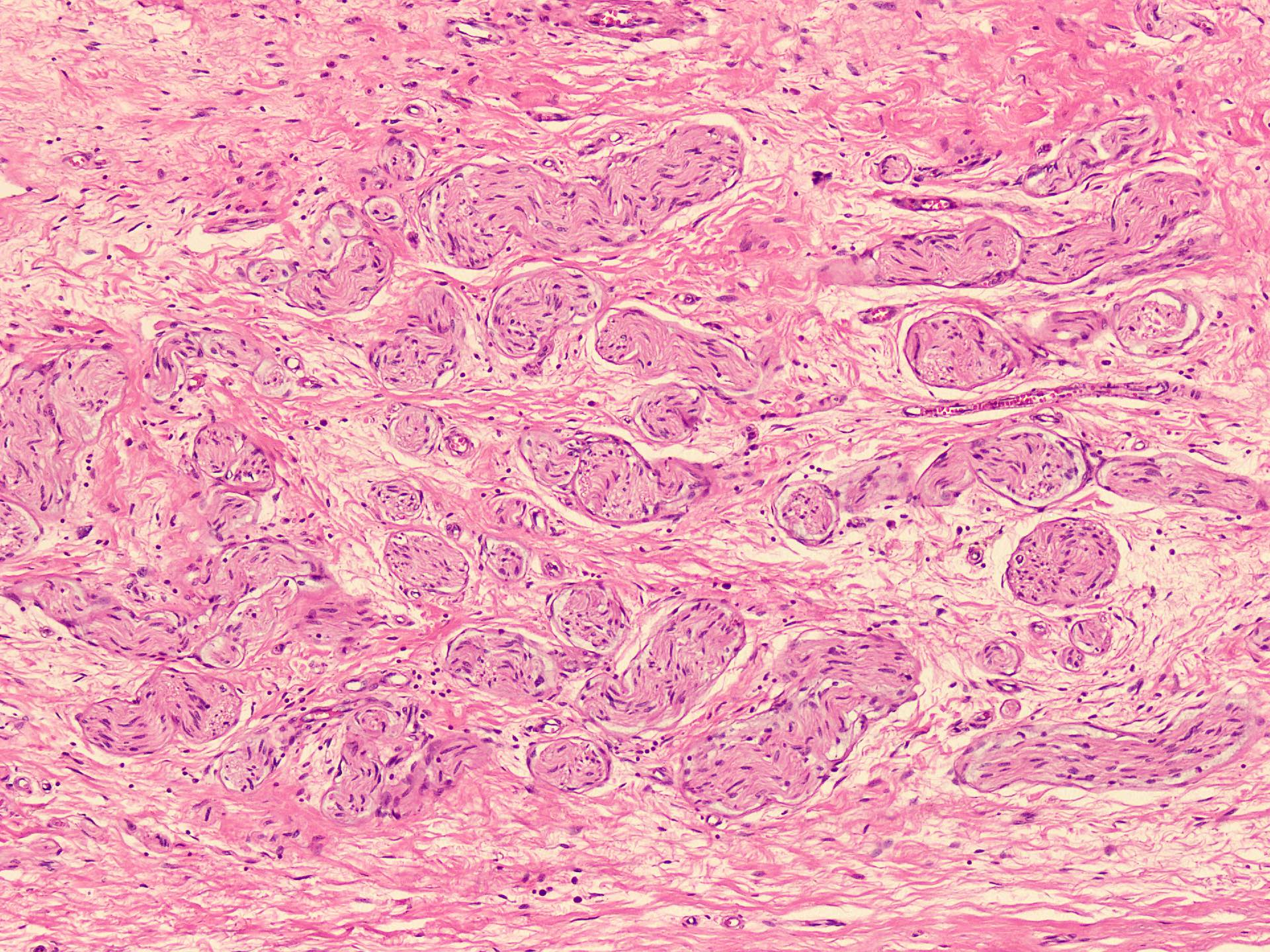
Variable sized bundles of nerve components
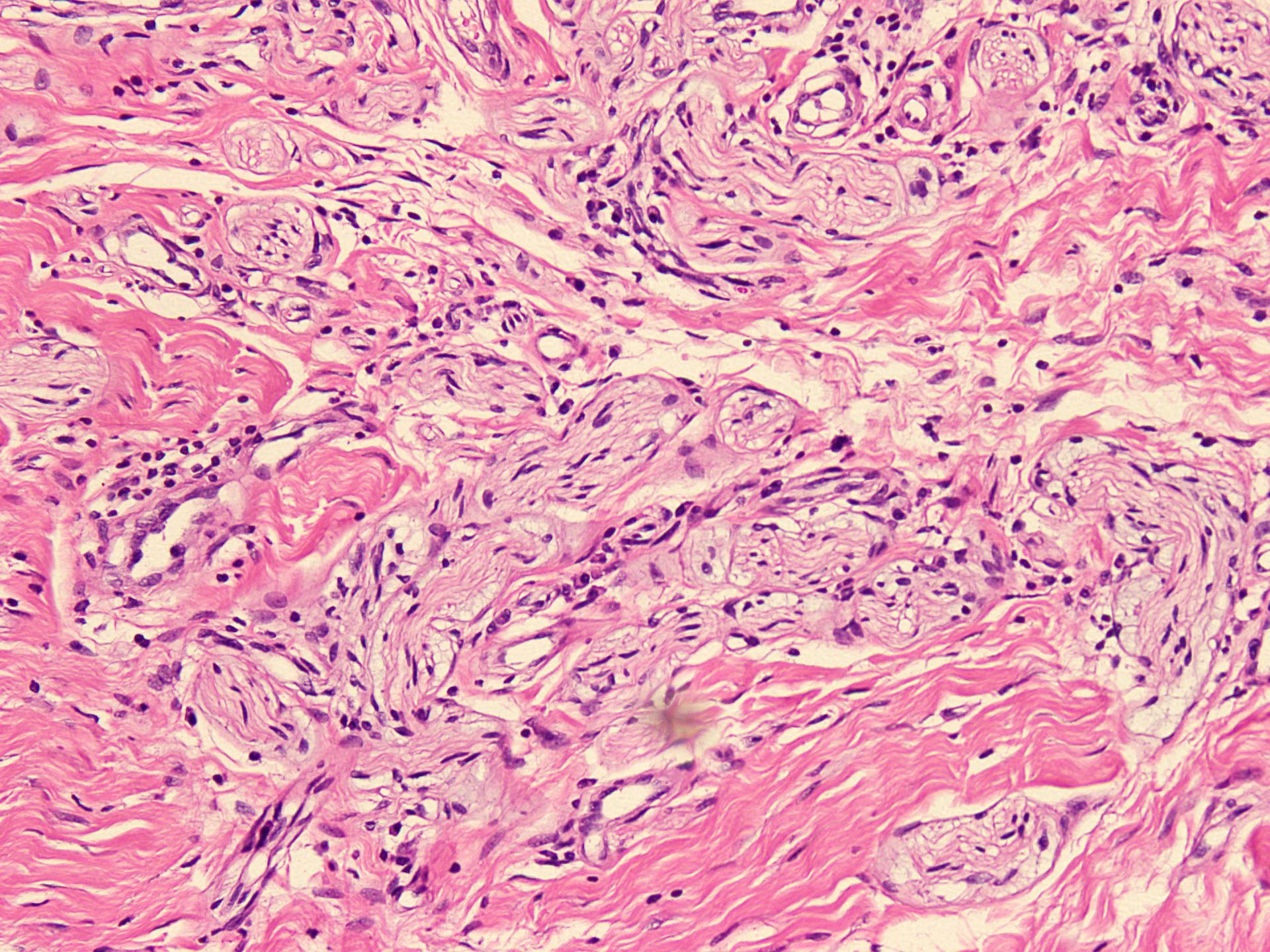
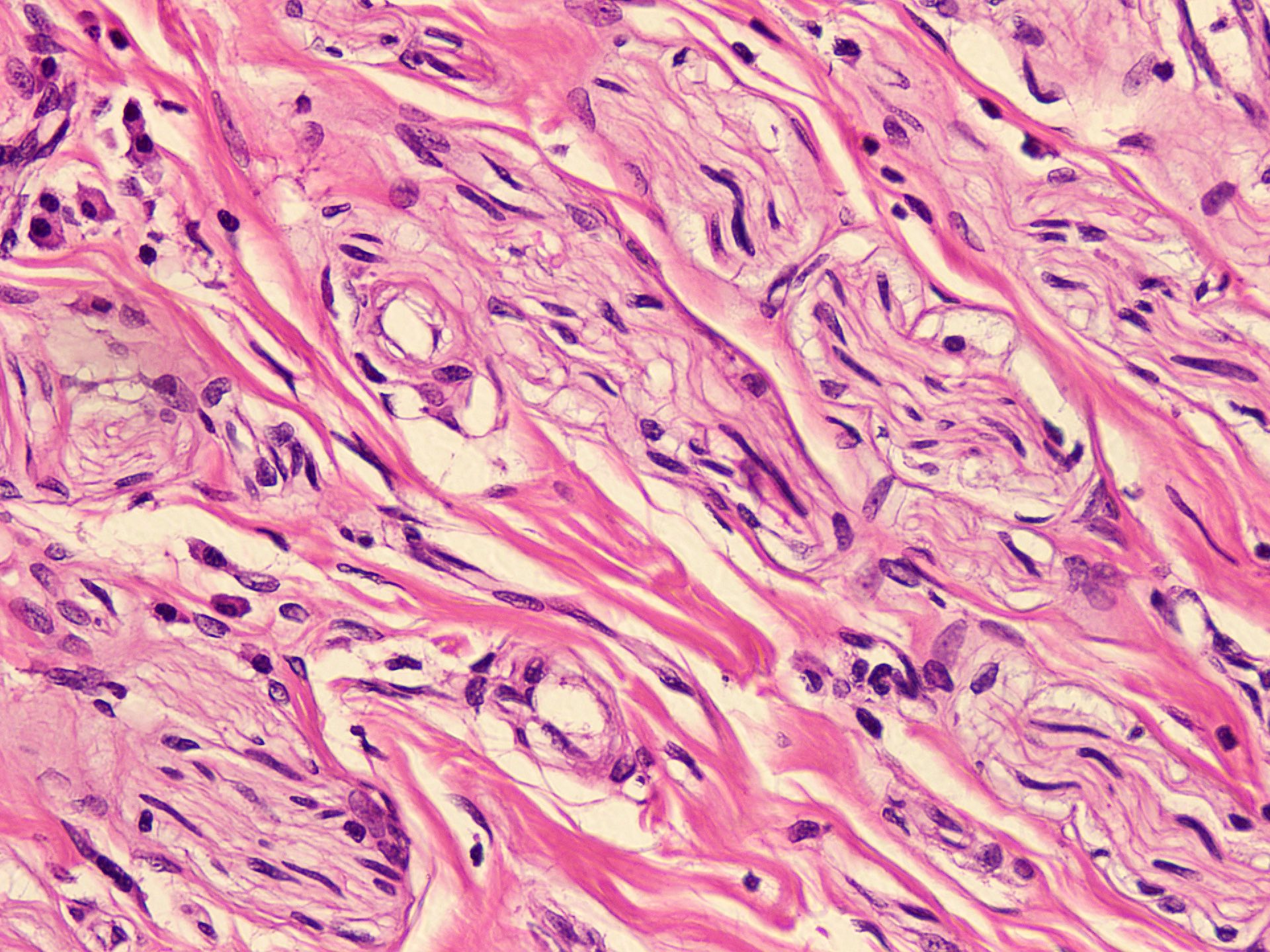
Bundles of spindle cells
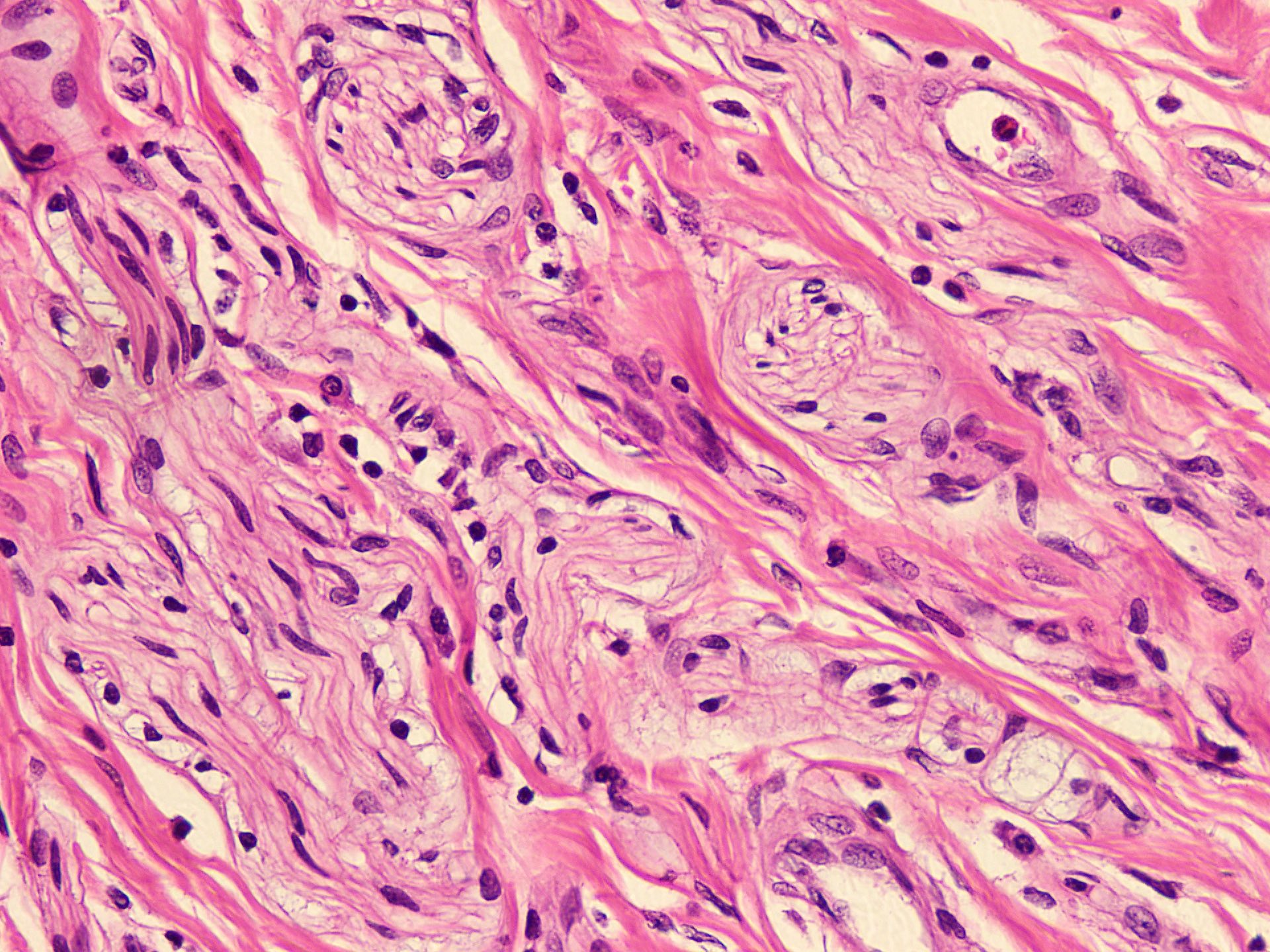
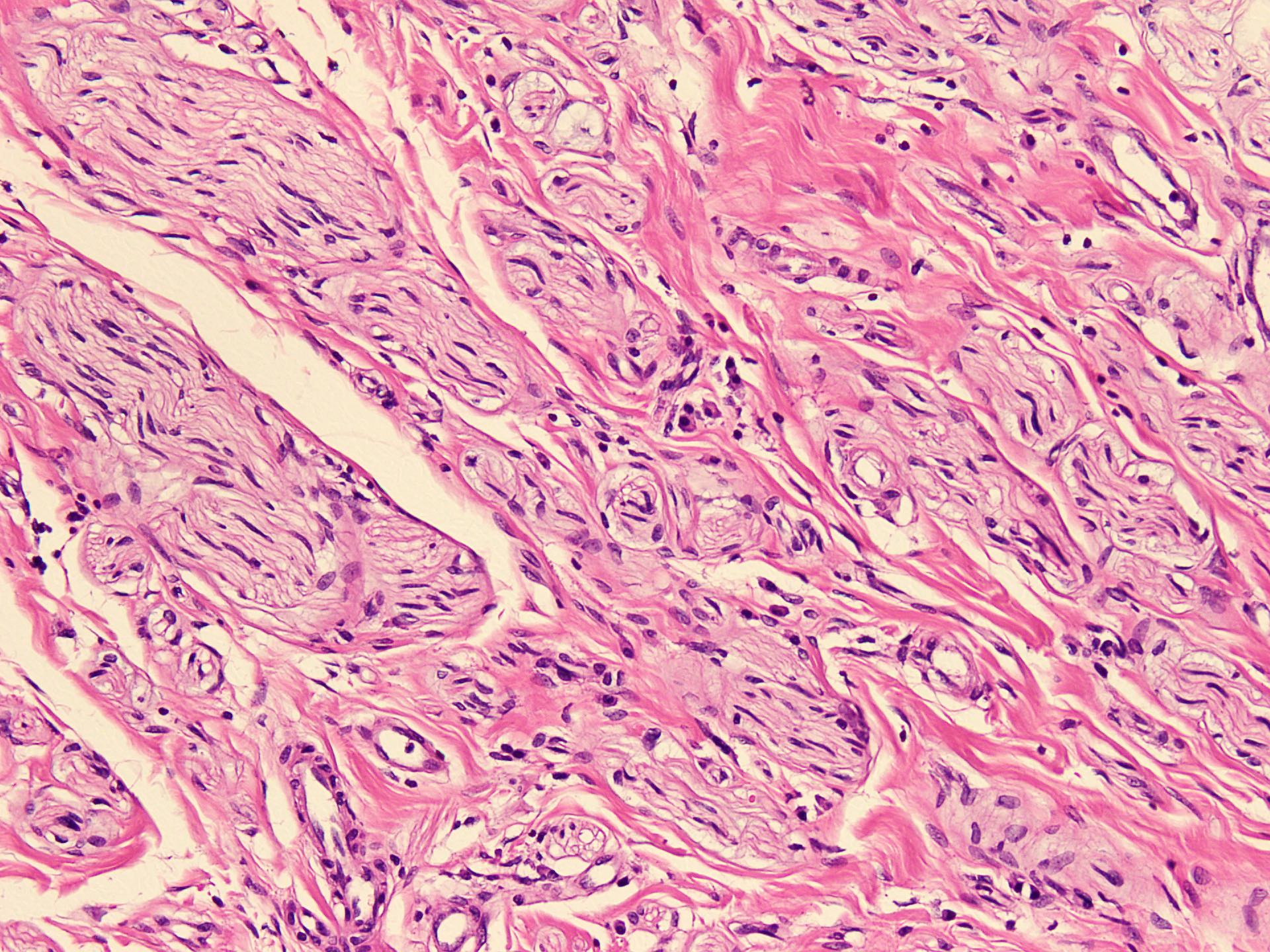
Clusters of nerve components
Cytology description
- FNAC of traumatic neuroma yields scant aspirate, hypocellular smears showing scattered spindle cells in single or clustered fashion (Patholog Res Int 2014;2014:678628)
Positive stains
- S100 (World J Clin Cases 2020;8:3821)
- CD68 and KiM1P: macrophage associated antigens aberrantly positive in Schwann cells (Goldblum: Rosai and Ackerman's Surgical Pathology, 11th Edition, 2017)
Videos
Nerve sheath tumors, etc.
by Dr. Jerad Gardner
Sample pathology report
- Upper limb, excision:
- Neuroma (see comment)
- Microscopy: The sections examined show a circumscribed, unencapsulated lesion composed of variable sized, closely packed nerve bundle along with scar tissue in the background.
- Comment: It is a benign condition and has been completely excised.
Differential diagnosis
- Localized interdigital neuritis (Morton neuroma / Morton metatarsalgia):
- Occurs in female adults
- Location: interdigital planter nerve between third and fourth toes
- Histology: markedly distorted nerve with extensive perineurial fibrosis arranged in concentric circles
- IHC: S100 positive
- Neurofibroma:
- In skin, deeply situated medium sized nerve, common in patient with type 1 neurofibromatosis
- Location: no particular anatomical distribution
- Histology: haphazard proliferation of Schwann cells, fibroblasts, perineurial cells, few axons and mast cells, shredded collagen fibers and myxoid stroma
- IHC: S100, SOX10, collagen IV, CD34 positive, EMA positive at periphery
- Palisaded encapsulated neuroma:
- Age: middle age
- Location: small, solitary asymptomatic papule in face skin
- Histology: dermal encapsulated lesion exhibiting Schwann cells and numerous axons with perineurium
- IHC: S100, neurofilament, EMA
- Schwannoma:
- Age: occurs in all ages with peak incidence in fourth to sixth decade
- Few sporadic cases associated with type 2 neurofibromatosis
- Location: flexor surface of extremities, neck, mediastinum, retroperitoneum, spinal roots and cerebellopontine angle
- Histology: encapsulated lesion with hypocellular and hypercellular areas of spindle cells, Verocay bodies present
- IHC: S100, H3k27me3
- Mucosal neuroma:
- Associated with multiple endocrine neoplasia type 2 (MEN2) caused by RET proto-oncogene, known as mucosal neuroma syndrome
- Variant of traumatic neuroma with distinctive clinical features; however, not associated with trauma or surgery
- Syndrome is characterized by presence of medullary carcinoma thyroid, pheochromocytoma, marfanoid features and mucosal neuromas of the tongue, lips, inner cheeks and inner eyelids (J Oral Maxillofac Pathol 2020;24:339)
Additional references
Practice question #1
A patient presented with a painful nodule that developed after an amputation of the left first finger. On examination, the nodule is painful. Excision of the lesion is performed which shows the histology above. Which of the following is the most likely diagnosis?
- Granular cell tumor
- Neurofibroma
- Neurothekoma
- Traumatic neuroma
- Schwannoma
Practice answer #1
