

Testis & paratestis
Germ cell tumors
Cystic trophoblastic tumor
Editorial Board Member: Bonnie Choy, M.D.
Deputy Editor-in-Chief: Maria Tretiakova, M.D., Ph.D.


Last author update: 29 February 2024
Last staff update: 1 March 2024
Copyright: 2017-2024, PathologyOutlines.com, Inc.
PubMed Search: Cystic trophoblastic tumor
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Gupta P, Mehta V. Cystic trophoblastic tumor. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/testisctt.html. Accessed April 18th, 2024.
Definition / general
- Distinctive cystic trophoblastic lesion arising after spontaneous or chemotherapy induced regression of choriocarcinoma
- Described predominantly in postchemotherapy retroperitoneal lymph node dissections of patients with testicular germ cell tumors
- Has also been described to involve extragonadal sites in both treated and untreated testes of patients with mixed germ cell tumors
Essential features
- Cystic proliferation of trophoblasts in postchemotherapy resections from patients with metastatic, nonseminomatous germ cell tumors of the testis
- Not aggressive, with behavior that is similar to postchemotherapy residual teratoma
Terminology
- Cystic trophoblastic tumor (CTT)
- Previously known as choriocarcinoma-like lesion (CCLL) with 2 subtypes: teratomatous CCLL and cystic atypical choriocarcinoma (Am J Surg Pathol 1988;12:531)
ICD coding
Epidemiology
- Patient age can range from 15 to 43 years (Am J Surg Pathol 2004;28:1212, Am J Surg Pathol 2017;41:788)
Sites
- Primarily postchemotherapy retroperitoneal lymph nodes with mixed germ cell tumors
- Treated or untreated testes with mixed germ cell tumors
- Extragonadal sites (e.g., central nervous system) secondary to treated or untreated testicular mixed germ cell tumors
Etiology
- May arise from regressing choriocarcinoma as the more aggressive cells are eliminated by chemotherapy or spontaneous regression, leading to the persistence of a slow growing, less aggressive component of intermediate type trophoblasts that develops into cystic trophoblastic tumor (Am J Surg Pathol 2017;41:788)
- Cystic trophoblastic tumor may also represent an intermediate stage in the maturation of choriocarcinoma to teratoma (Am J Surg Pathol 2004;28:1212)
- Recent research shows that the levels of miR-371a-3p are negligible in CTT; these findings are similar to those found in postpubertal type teratoma and to the metastatic mature teratoma masses; hence, it supports the hypothesis that CTT represents an advanced maturation step toward teratoma (Histopathology 2023;83:151)
Clinical features
- Most commonly seen in patients with testicular germ cell tumors after cisplatin based chemotherapy
- Can occur as part of primary testicular mixed germ cell tumors and are occasionally seen in visceral and nonregional lymph node germ cell tumor metastases (Am J Surg Pathol 2017;41:788)
- Less commonly, these tumors have been described in germ cell tumor patients without chemotherapy (Virchows Arch 2023;482:581)
Diagnosis
- Histologic examination of involved tissue
Laboratory
- Normal to mildly elevated levels of the beta subunit of human chorionic gonadotropin (βhCG)
Radiology description
- Enlarged retroperitoneal lymph nodes
Prognostic factors
- Prognosis of CTT in retroperitoneal lymph node dissection specimens is similar to that of teratoma and complete surgical resection without additional therapy is therefore recommended (Am J Surg Pathol 2017;41:788)
Case reports
- 12 year old boy with cystic trophoblastic tumor in a primary central nervous system postchemotherapy germ cell tumor (Int J Surg Pathol 2020;28:925)
- 22 year old man with mixed germ cell tumor composed of postpubertal teratoma, embryonal carcinoma and cystic trophoblastic tumor (Cesk Patol 2022;67:212)
- 31 year old man with metastatic cystic trophoblastic tumor without prior chemotherapy (Urol Case Rep 2017;13:154)
Treatment
- Requires no further treatment, however, these patients should be carefully monitored on follow up
Gross description
- CTT is admixed commonly with teratoma and less commonly with other germ cell tumors and it occurs in small proportions; for these reasons, characteristic gross features cannot be ascribed to it
Microscopic (histologic) description
- Cysts lined by squamoid appearing, predominantly mononucleated intermediate trophoblasts
- Cyst may vary in size and shape and often appears collapsed among other germ cell tumor components
- Cells display smudged nuclei with abundant eosinophilic cytoplasm, suggesting a degenerative phenotype
- Cytoplasmic lacunae (vacuoles) may be present
- Small solid clusters of cells and single cells may be seen adjacent to the larger cysts
- Cyst may contain eosinophilic secretion or fibrinoid material
- Cytoplasmic lacunae may coalesce to create variably sized spaces
- Mitoses are rarely seen
- Reference: Am J Surg Pathol 2004;28:1212, Am J Surg Pathol 2017;41:788
Microscopic (histologic) images
Contributed by Vikas Mehta, M.D.
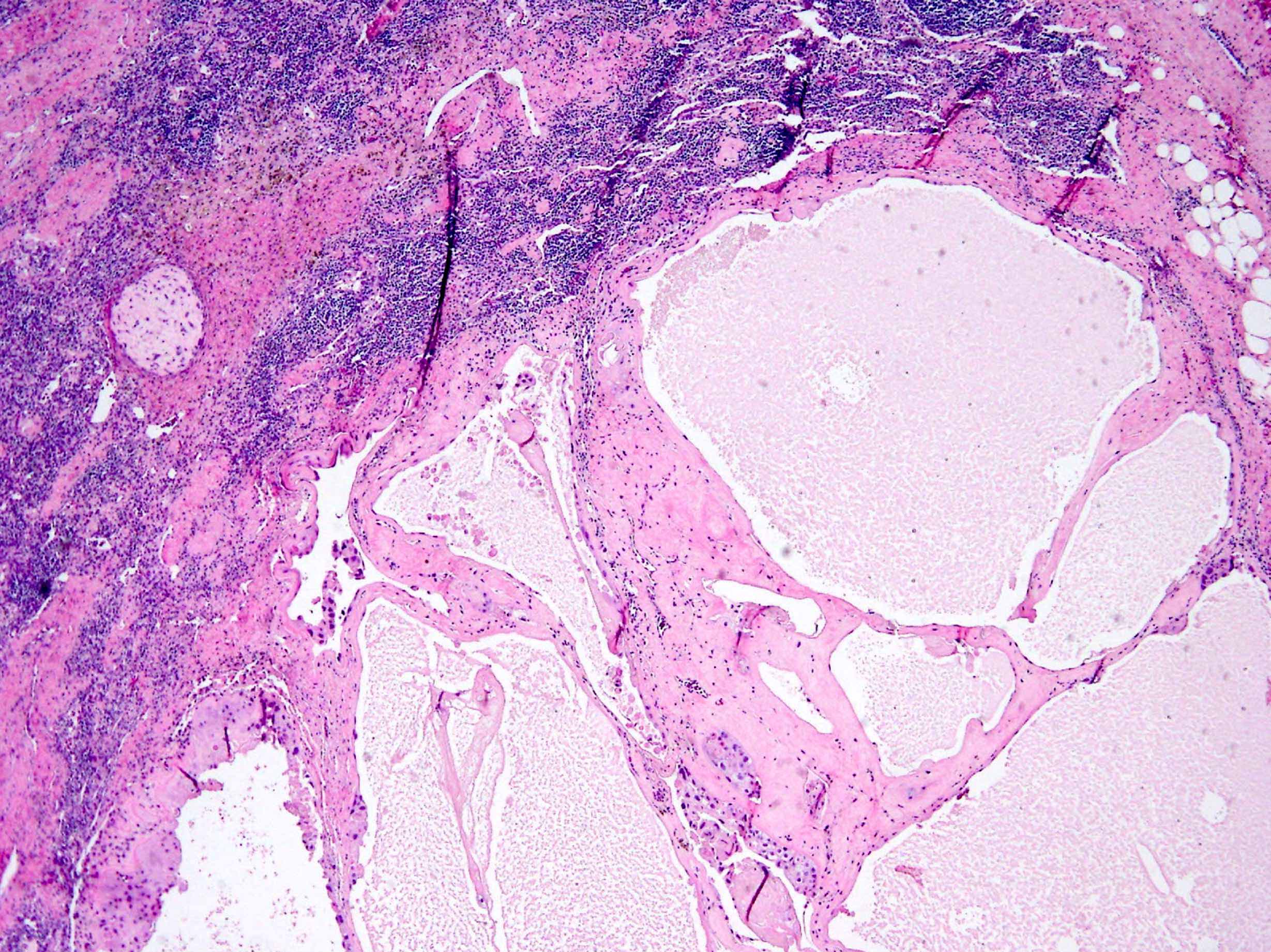
Cyst, fibrinoid material
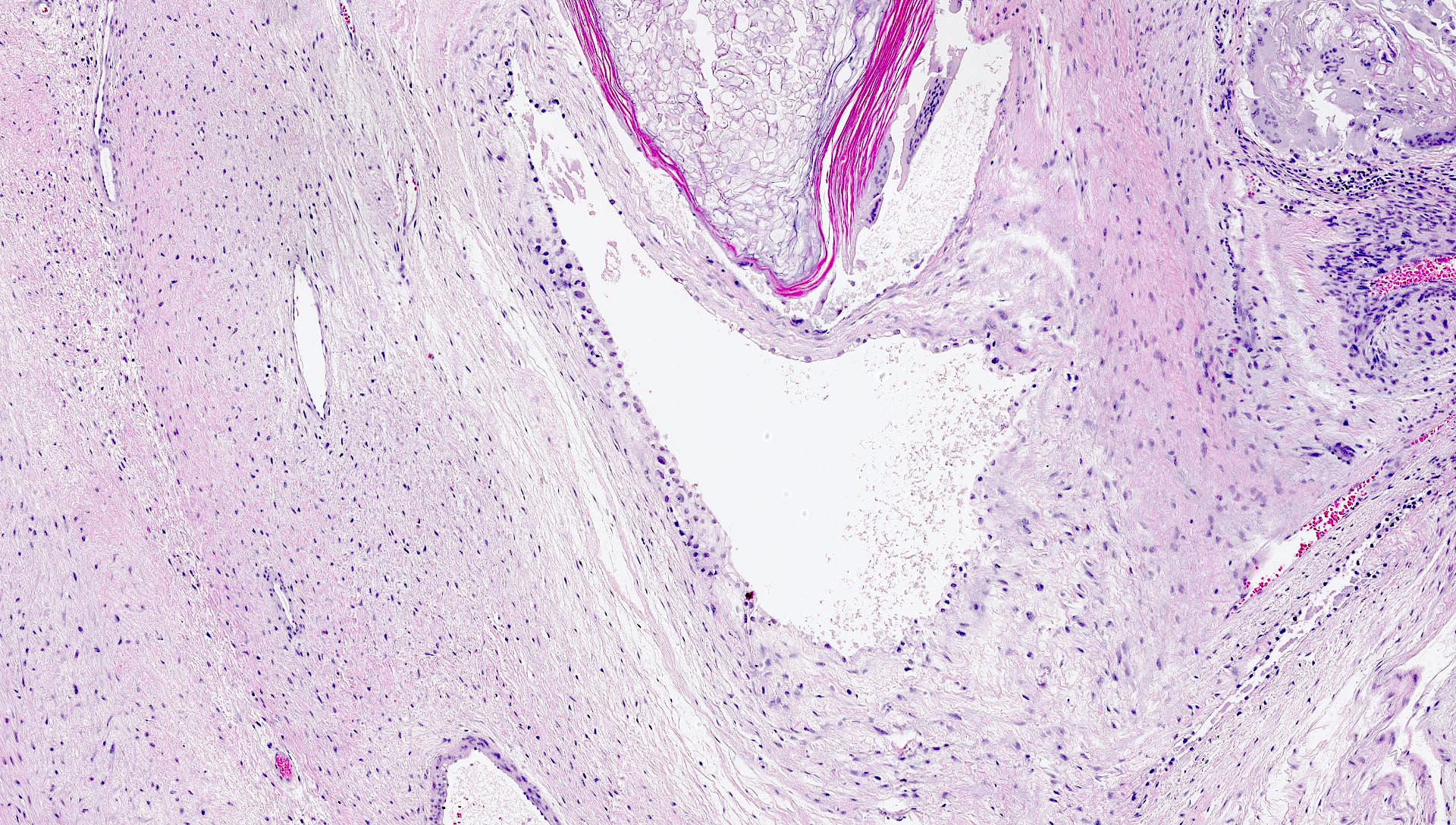

Intermediate type trophoblasts

Intermediate trophoblasts, smudged chromatin

Solid nest, fibrinoid material

βhCG positivity
Positive stains
- GATA3 diffusely positive
- GATA3 has been reported to be negative on rare occasions (Int J Surg Pathol 2020;28:925)
- Inhibin, p63 and hCG are variably positive (Am J Surg Pathol 2017;41:788)
Negative stains
Sample pathology report
- Retroperitoneal lymph node, lymph node dissection:
- Metastatic teratoma in a background of extensive fibrosis and necrosis; microscopic foci of cystic trophoblastic tumor
Differential diagnosis
- Choriocarcinoma:
- Distinctly biphasic, hemorrhagic and pleomorphic; displays brisk mitotic activity
- βhCG levels are expected to be highly elevated
- Teratoma:
- Demonstrates varying degrees of atypia
- Any type of tissue may be present, such as gastrointestinal glands, respiratory epithelium, cartilage, squamous epithelium with keratinization, primitive undifferentiated spindle cells or neuroepithelium
- Somatic malignancy, such as squamous cell carcinoma:
- Hypercellular variants with foci of solid areas can mimic CTT
Additional references
Board review style question #1
Which of the following is a feature consistent with cystic trophoblastic tumor?
- Biphasic pattern of admixed cytotrophoblasts and syncytiotrophoblasts
- Infiltrative growth pattern
- Normal to mildly elevated serum levels of βhCG
- Variable SALL4 expression in mononuclear cells
Board review style answer #1
C. Normal to mildly elevated serum levels of βhCG is consistent with cystic trophoblastic tumors. Other features are characteristic of choriocarcinoma in which βhCG levels are expected to be highly elevated.
Answer A is incorrect because choriocarcinoma is biphasic, hemorrhagic and pleomorphic and it displays brisk mitotic activity.
Answer B is incorrect because choriocarcinoma exhibits an infiltrative and destructive pattern.
Answer D is incorrect because SALL4 positivity is seen in cytotrophoblasts in choriocarcinoma.
Comment Here
Reference: Cystic trophoblastic tumor
Comment Here
Reference: Cystic trophoblastic tumor
Board review style question #2
Which of the following statements is true for cystic trophoblastic tumors (CTTs)?
- CTTs after chemotherapy show a high frequency of progressive disease and warrant additional chemotherapy
- CTTs are identified exclusively in the setting of postchemotherapy retroperitoneal lymph node dissections of patients with testicular germ cell tumors
- CTTs lack keratohyaline granules and central keratin and often have intracytoplasmic lacunae
- CTTs show goblet cells, ciliated cells and other specialized epithelial types
Board review style answer #2
C. CTTs lack keratohyaline granules and central keratin and often have intracytoplasmic lacunae. Answer A is incorrect because the prognosis of CTT is similar to teratoma and requires no further treatment but a close follow up. Answer B is incorrect because CTT was first described in retroperitoneal lymph node dissections after chemotherapy; however, it is now known that these tumors can occur as part of primary testicular mixed germ cell tumors and they are occasionally seen in visceral and nonregional lymph node germ cell tumor metastases. Less commonly, these tumors have been described in germ cell tumor patients without chemotherapy. Answer D is incorrect because cysts are lined by squamoid appearing cells with smudged irregular nuclei, abundant eosinophilic cytoplasm with intracytoplasmic lacunae and associated fibrinoid material.
Comment Here
Reference: Cystic trophoblastic tumor
Comment Here
Reference: Cystic trophoblastic tumor
