

Thyroid & parathyroid
Hyperplasia / goiter
Amyloid goiter
Last author update: 1 June 2017
Last staff update: 15 August 2023
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Amyloid goiter [title] thyroid



Table of Contents
Definition / general | Terminology | Epidemiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Differential diagnosis | Board review style question #1 | Board review style answer #1Cite this page: Aly F, Satturwar S. Amyloid goiter. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/thyroidamyloidgoiter.html. Accessed April 19th, 2024.
Definition / general
- First reported in 1855 (Rokitansky: A Manual Of Pathological Anatomy; Vol: I, 2008)
- Defined as a diffuse clinically apparent enlargement of the thyroid gland due to widespread amyloid deposits (von Eisenberg: Ueber einen Fall von Amyloid-Kropf, 1904)
- Rare entity
- Diagnosis often made at autopsy (Am J Clin Pathol 1995;104:306)
- Patients usually have normal thyroid function tests (euthyroid); minority have hyperthyroidism, hypothyroidism or thyroid autoantibodies
Terminology
- Also known as amyloid tumor of thyroid
Epidemiology
- Median age 54 years, range 23 - 75 years
- In adolescence associated with juvenile arthritis or familial Mediterranean fever
- Males > females
Etiology
- Due to systemic amyloidosis (majority arise in secondary AA amyloidosis)
- Secondary AA amyloidosis occurs as a result of chronic inflammatory conditions such as rheumatoid arthritis, Crohn's disease, familial Mediterranean fever, osteomyelitis or tuberculosis, resulting in increase in serum amyloid protein
- Also reported in dialysis dependent chronic renal failure patients as a result of beta-2-microglobulin accumulation (Case Rep Endocrinol 2012;2012:741754)
Clinical features
- Nontender, diffuse enlargement of gland over weeks to months
- May have obstructive symptoms of dyspnea, hoarseness, dysphagia
- Patients usually have normal thyroid function tests (euthyroid); minority have hyperthyroidism or hypothyroidism
Diagnosis
- Fine needle aspiration cytology
- Thyroidectomy for definitive diagnosis
Laboratory
- Majority have normal thyroid function tests (euthyroid)
- Minority have hyperthyroidism, hypothyroidism or thyroid autoantibodies
Radiology description
- Ultrasound: enlargement with high echogenicity and very fine homogenous echotexture similar to ground glass appearance (J Clin Ultrasound 1994;22:239)
Case reports
- 30 year old man with chronic kidney disease (Anal Quant Cytopathol Histpathol 2014;36:241)
- 40 year old man with parathyroid involvement (Arch Pathol Lab Med 2000;124:281)
- 46 year old man, a renal allograft recipient, with transthyretin type (Endocr Pathol 2008;19:66)
- 48 year old woman with multiple myeloma (Arch Pathol Lab Med 1990;114:429)
- 58 year old woman with diffuse fatty infiltration in amyloid goiter (Pathol Int 2007;57:449)
- 61 year old woman with diffuse thyroid enlargement (Case #247)
- Case with Castleman disease (Arch Pathol Lab Med 1989;113:542)
Treatment
- Treatment of underlying systemic amyloidosis
- Thyroidectomy to relieve pressure symptoms
- Treat associated hypothyroidism, which may cause cardiomyopathy, gastrointestinal involvement (leading to malabsorption of oral therapy) and abnormal circulating immunoglobulins, which may interfere with hormone assays or hormone function (Head Neck 1995;17:343)
Gross description
- Depending on the amount of amyloid deposited, thyroid gland can be soft, hard, diffuse or nodular
- Bilateral and diffusely enlarged gland with inhomogeneous nodules, whitish tan / light brown or pale yellow
Gross images
AFIP images
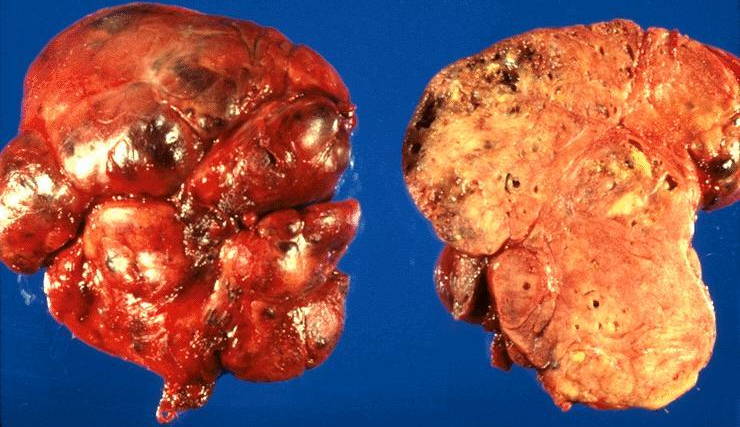
Enlarged and bosselated with salmon cut surface
Images hosted on other servers:

Lipomatosis and amyloidosis
Microscopic (histologic) description
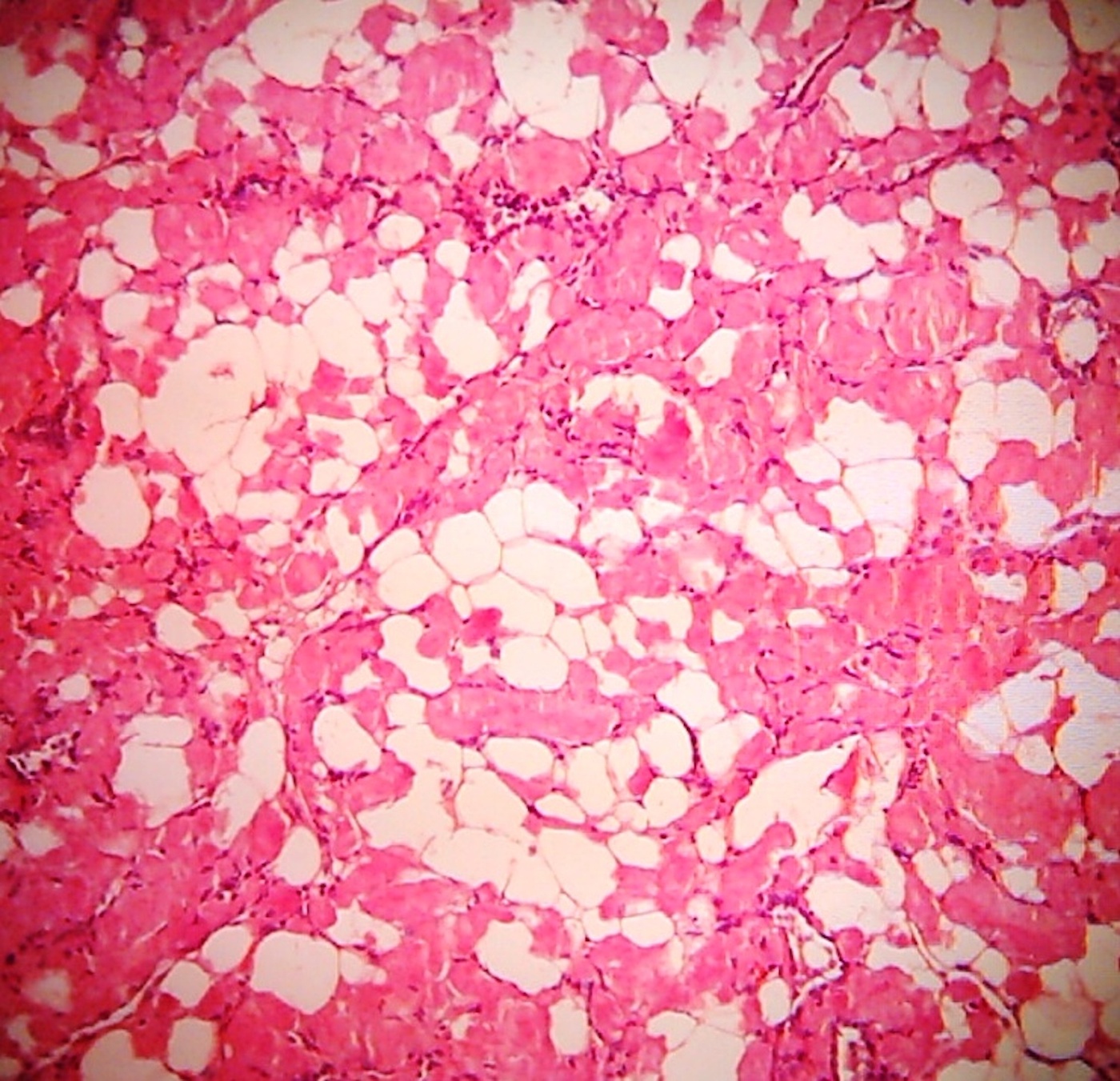
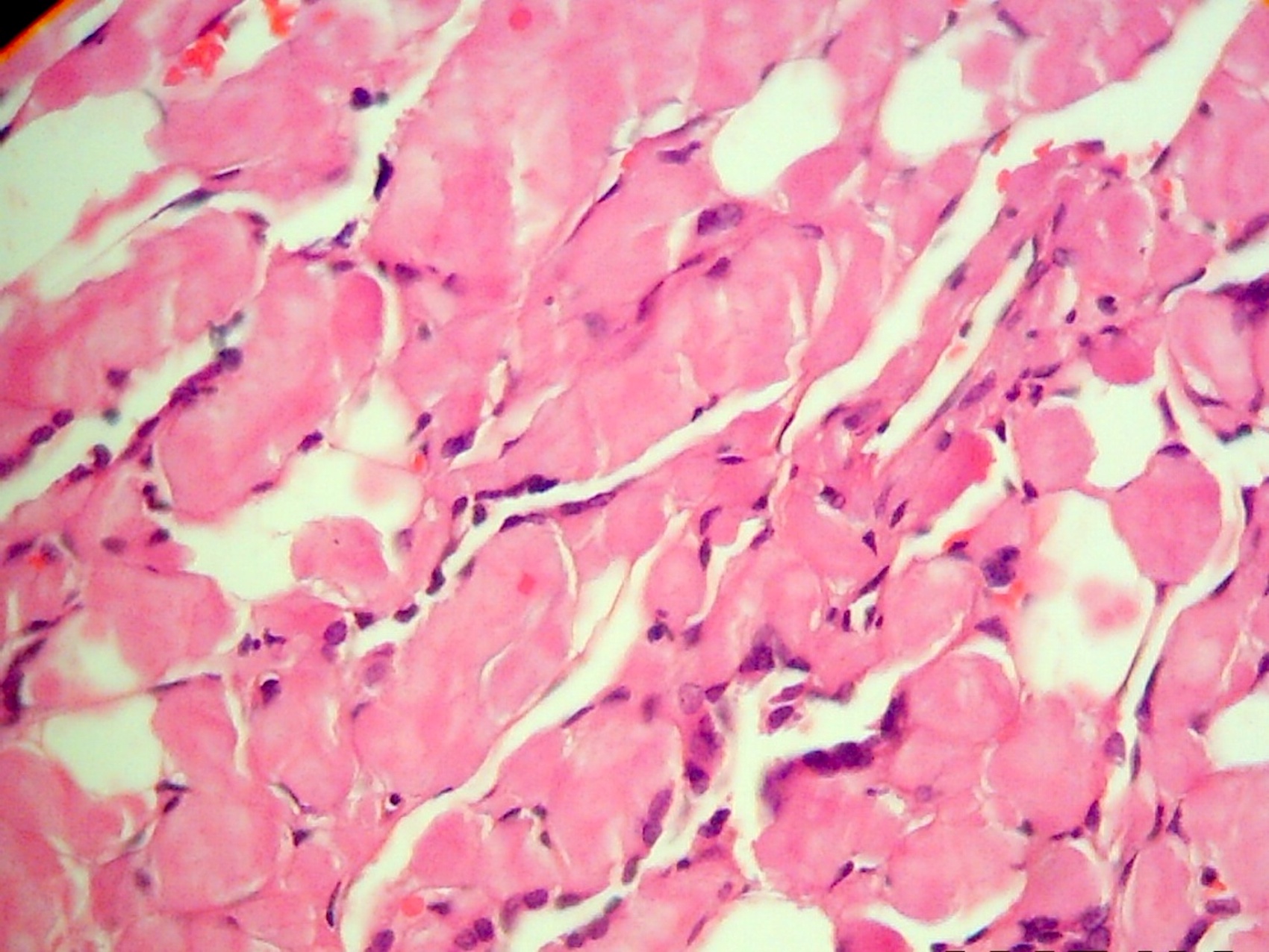
- Diffuse deposition of amorphus eosinophilic fibrillary material in perifollicular and perivascular regions, may replace thyroid follicles
- Other associated findings: fatty metaplasia, foreign body giant cell reaction, squamous metaplasia or focal lymphocytic thyroiditis
Microscopic (histologic) images
Contributed by Nazar M. T. Jawhar, M.D.
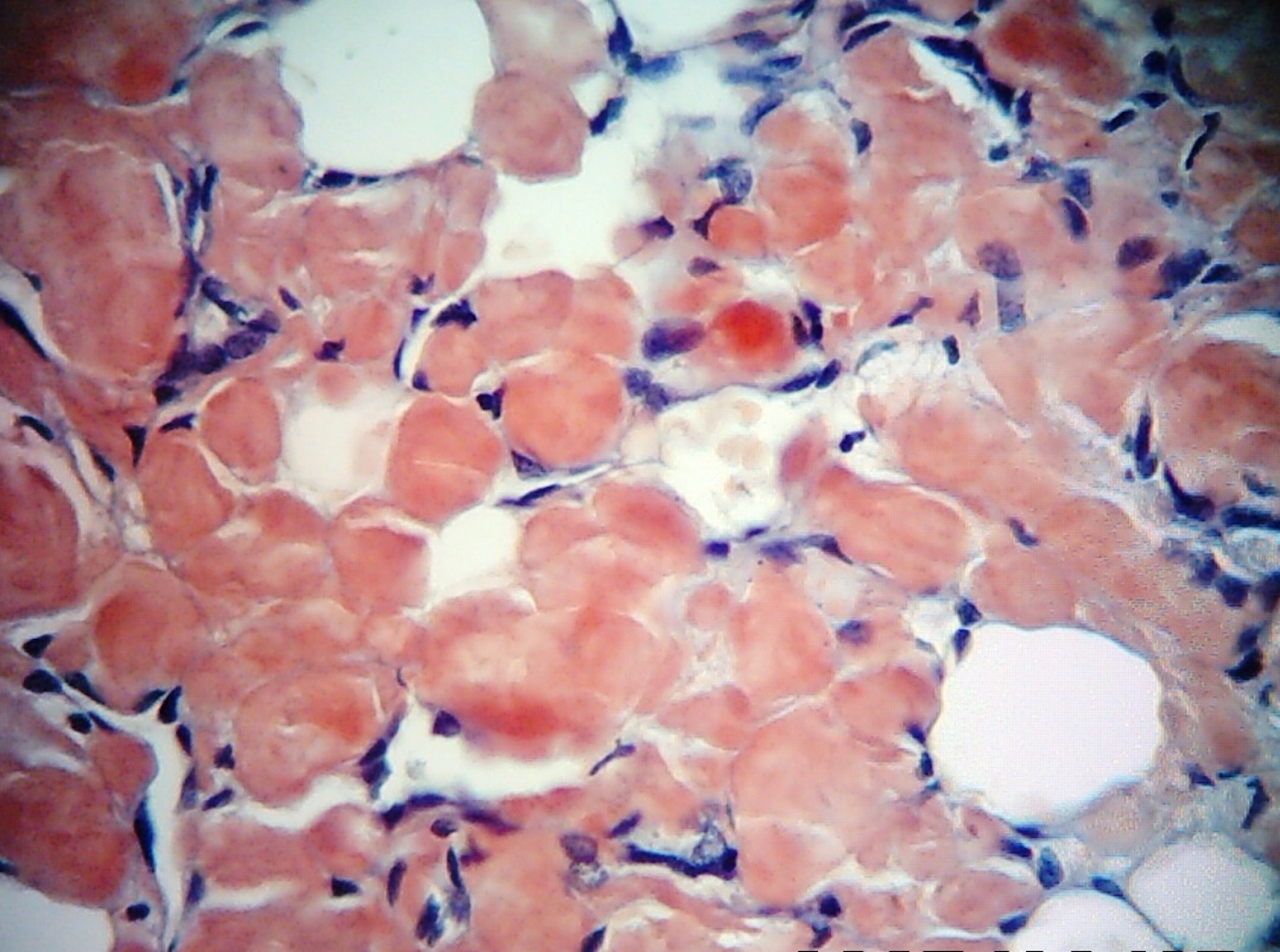
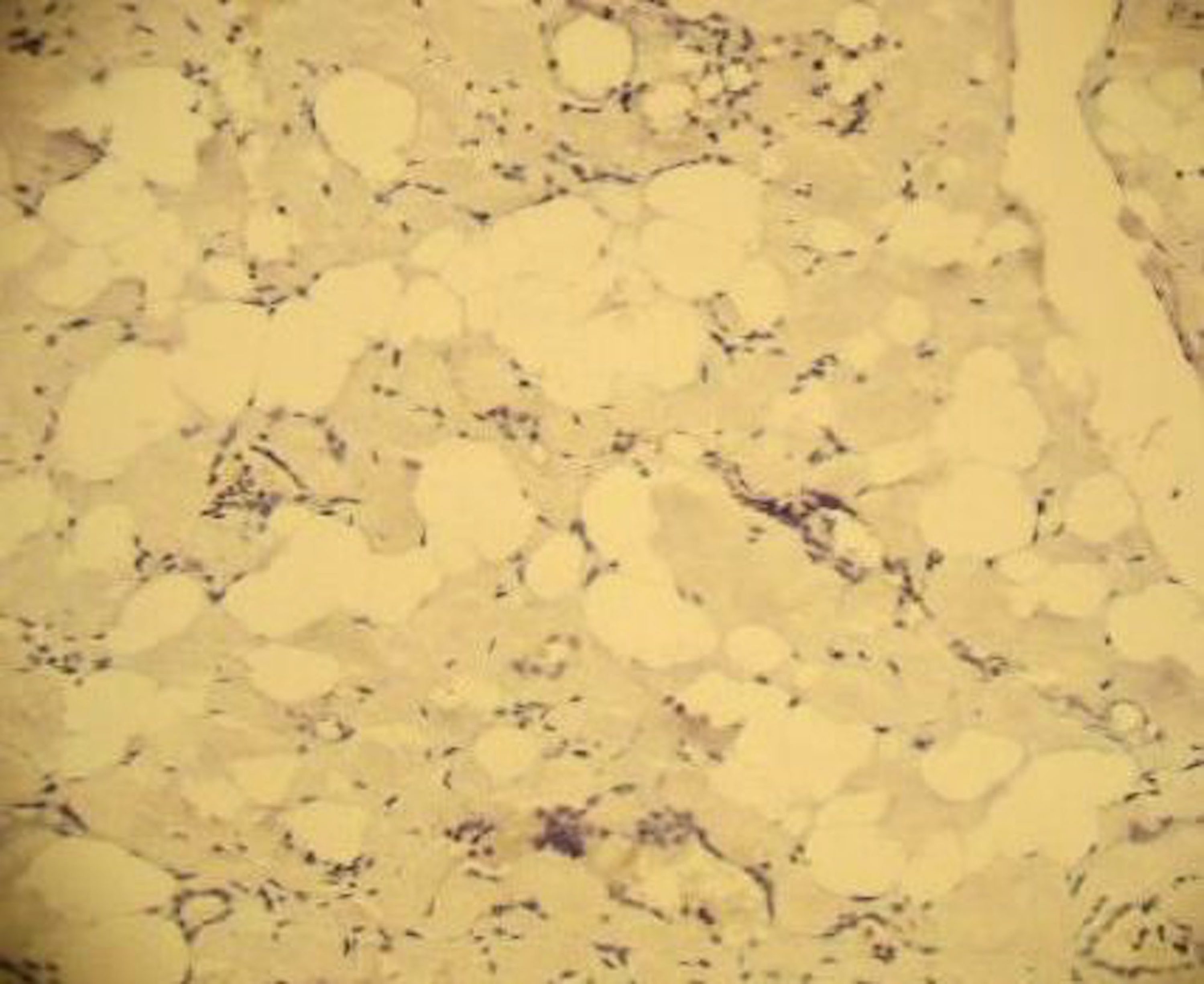
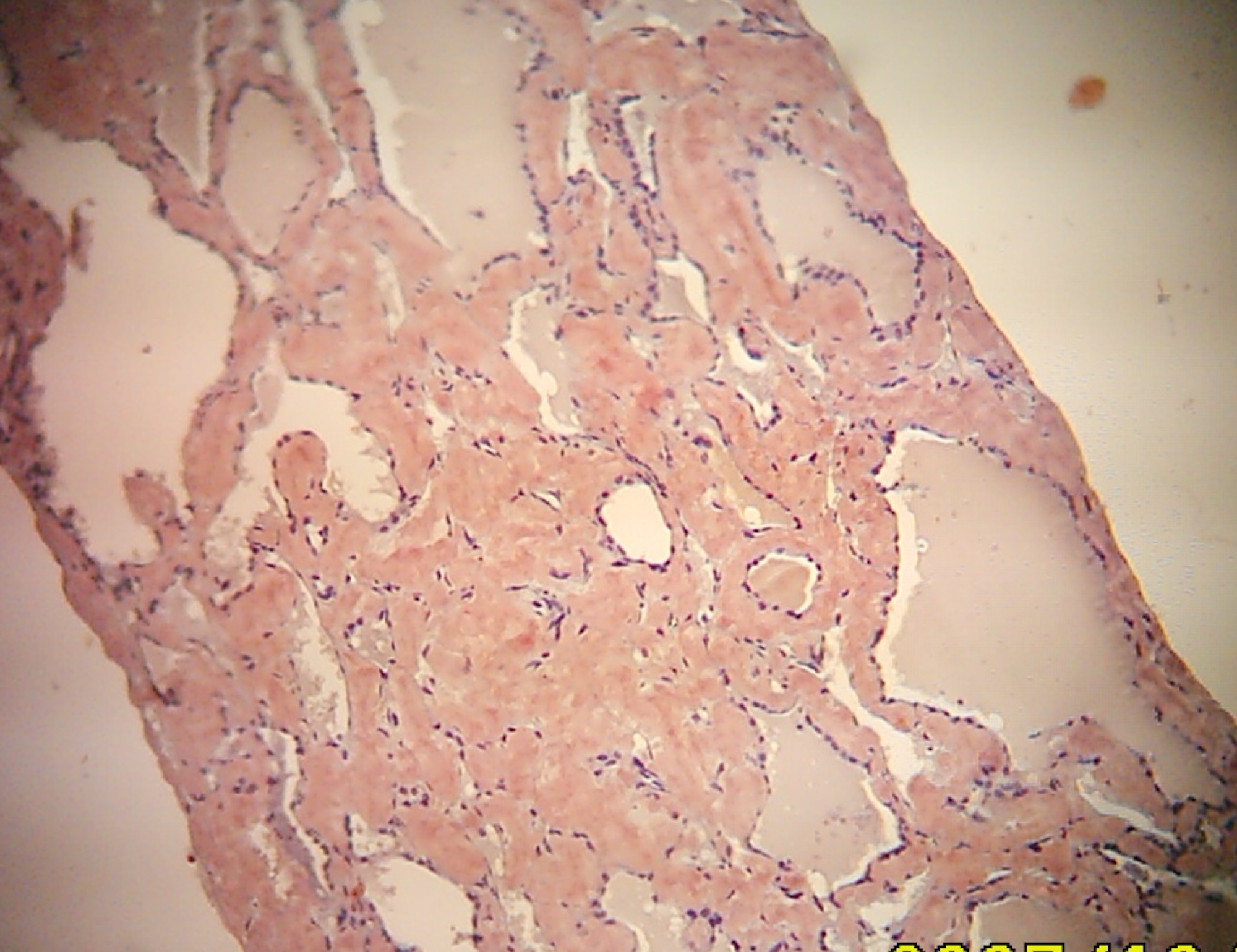
Various images
Case #247 and AFIP images

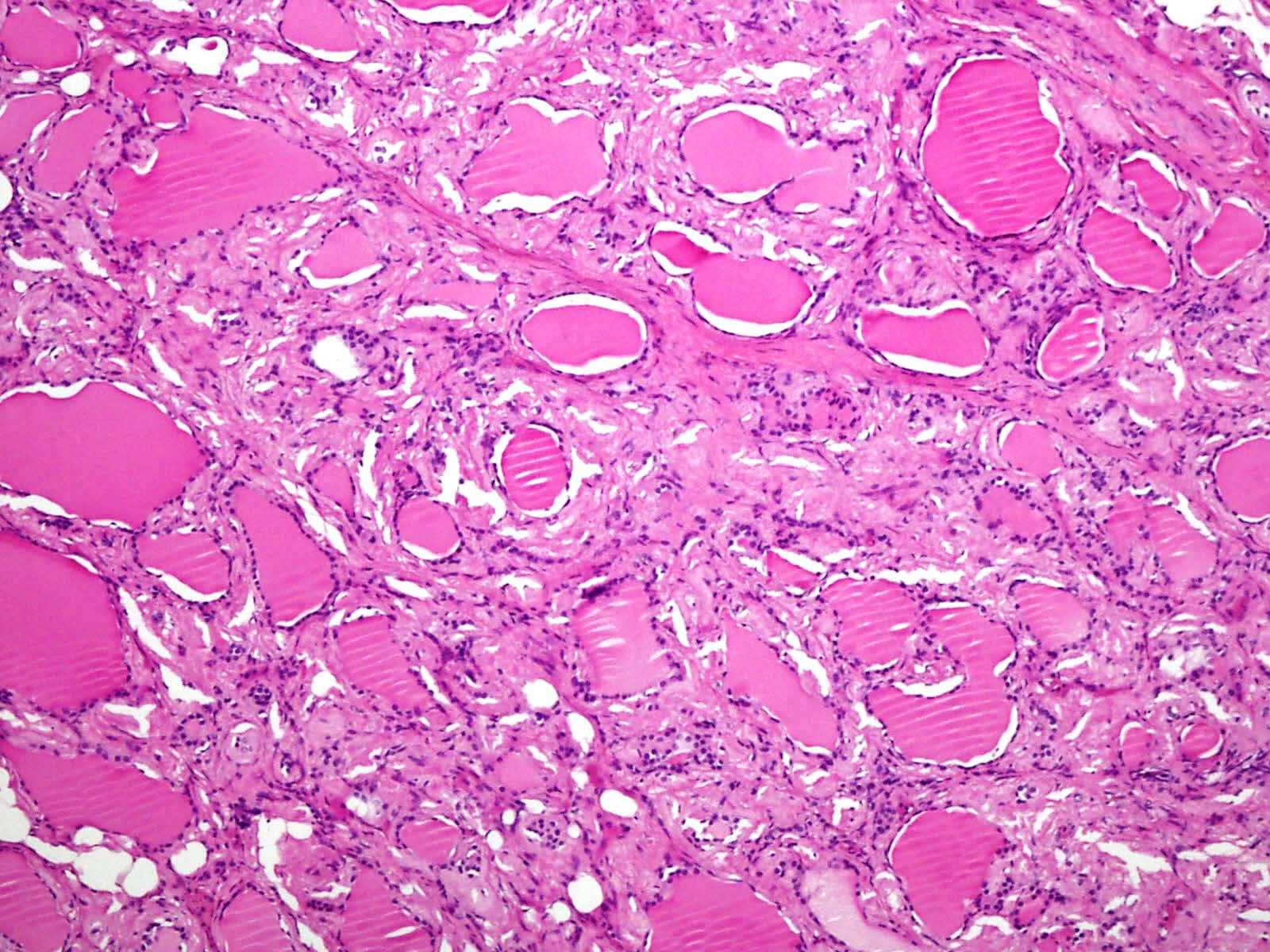
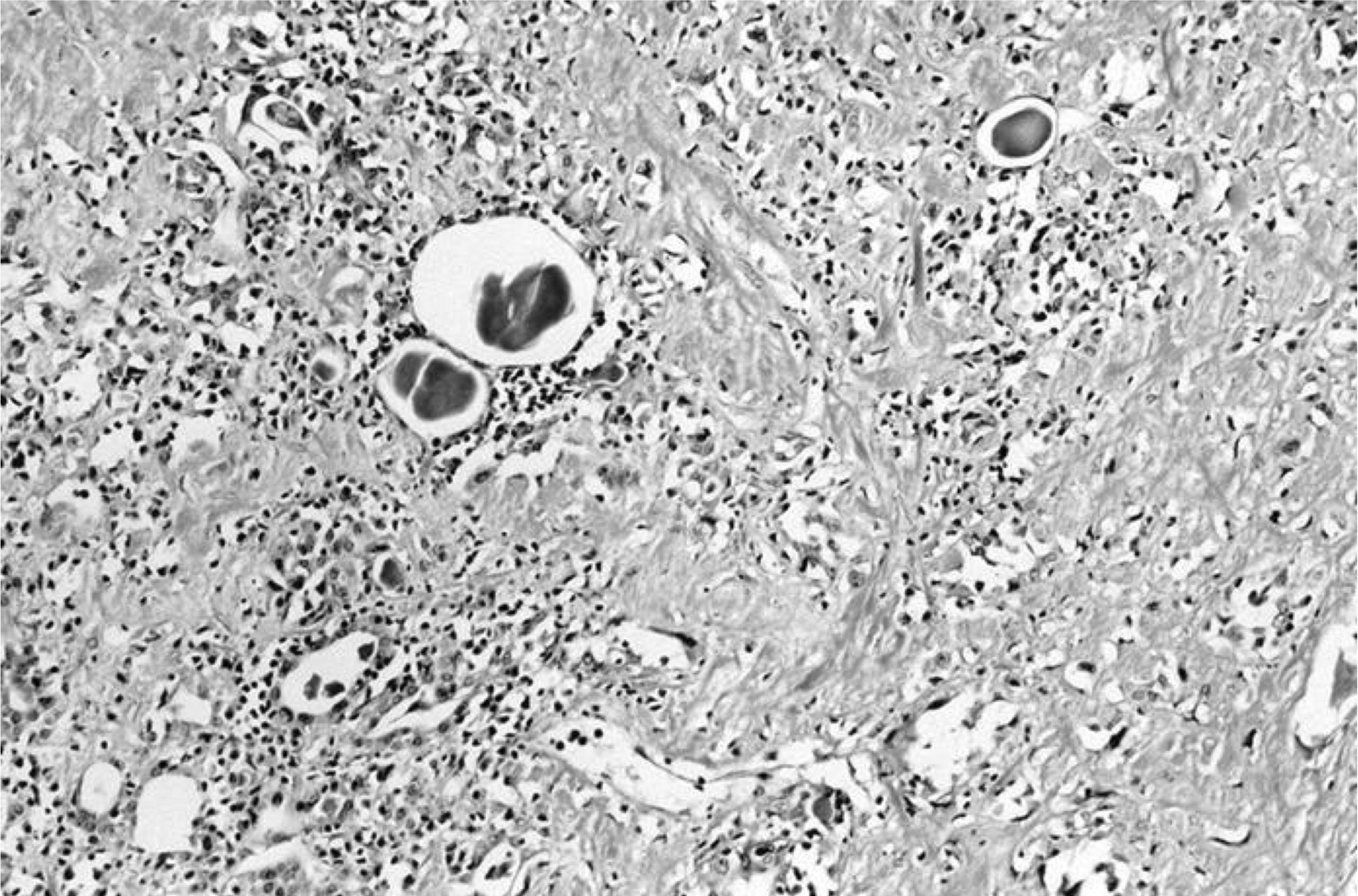
Amyloid and inflammatory cells
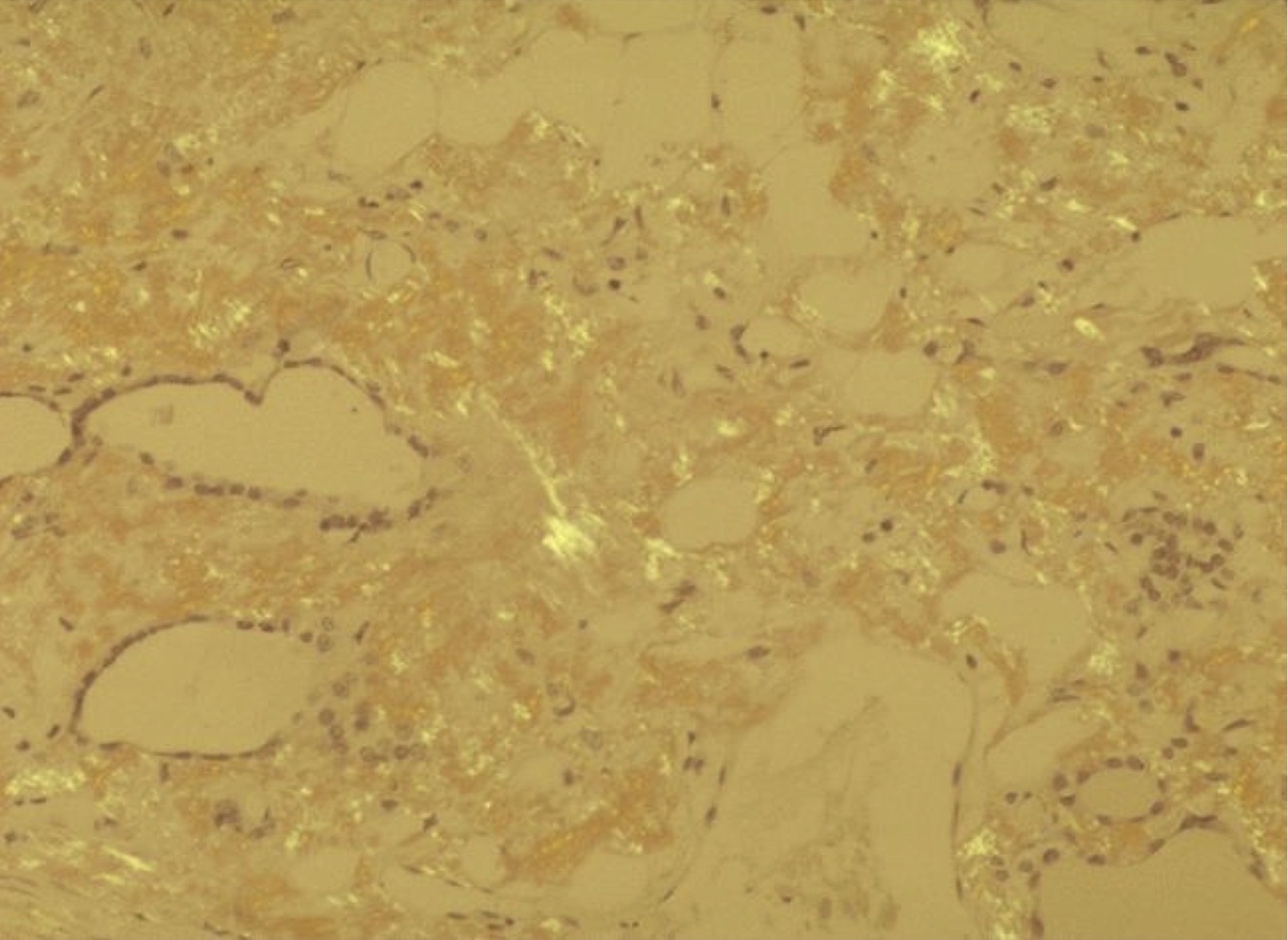
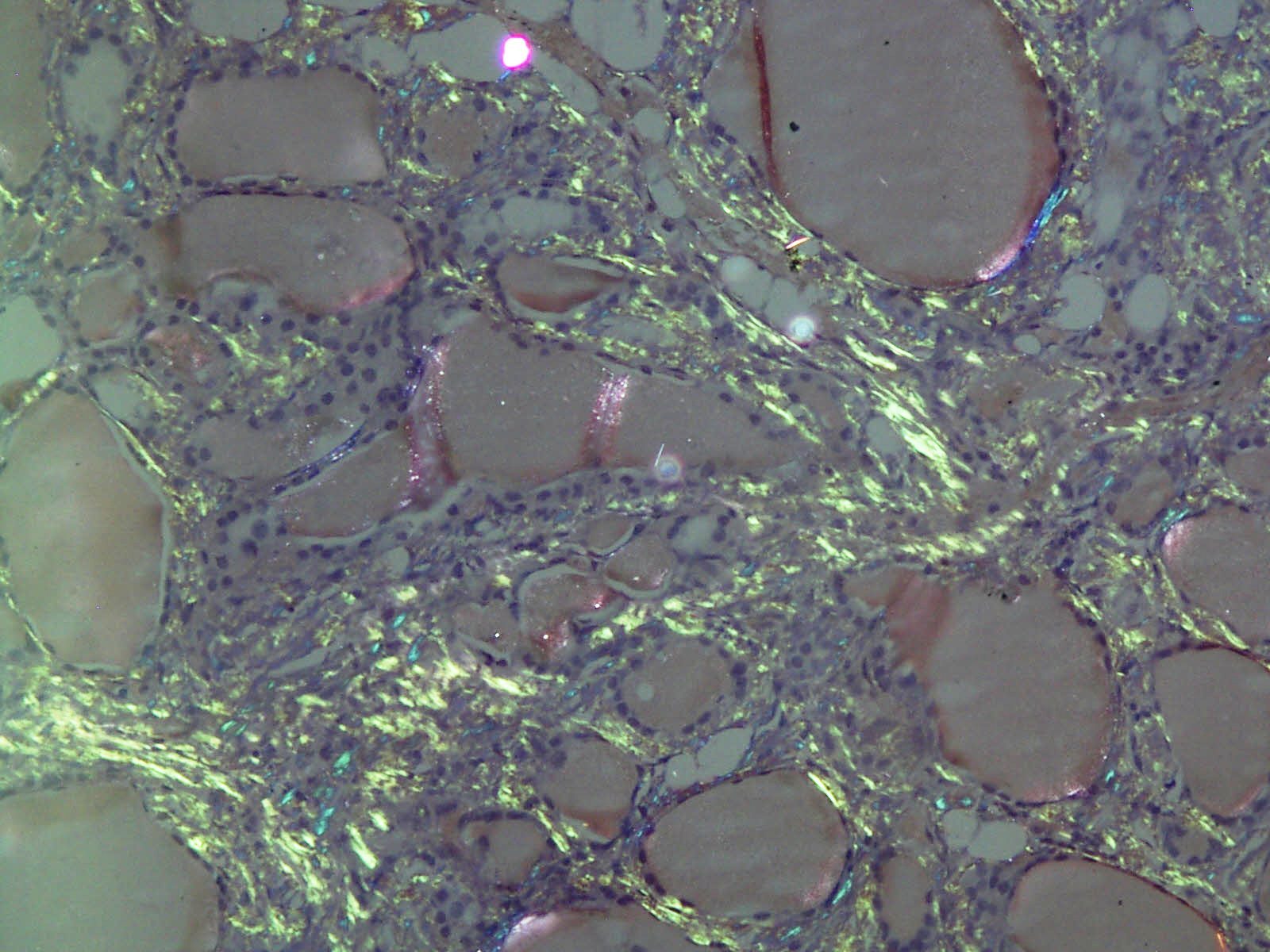
Apple green birefringence
Images hosted on other servers:

Birefringent apple green staining under polarized light
Cytology description
- Dense amorphus clumps of extracellular material or irregularly shaped fragments with scalloped and pointed edges
- The amorphous fragments stain eosinophilic on Papanicolaou stain, magenta colored on Giemsa and deep blue with Diff-Quick cytology stain
Positive stains
- Congo red shows salmon color and apple green dichroism with polarized light
- The type of fibril can be determined by immunochemical staining using specific antibodies (AL and AA)
Negative stains
Differential diagnosis
- Medullary thyroid carcinoma: calcitonin+ tumor cells present
- Microscopic deposition of amyloid within the thyroid occurs in 59 - 92% of patients with amyloidosis; this frequency is similar between AL and AA amyloidosis (Q J Med 1974;43:127) but is not considered part of the amyloid goiter discussed here
Board review style question #1
Which statement about amyloid goiter of the thyroid is false?
- Can be seen in renal transplant patients on dialysis
- Commonly seen in males
- Is associated with medullary thyroid carcinoma
- Microscopically shows diffuse deposition of amyloid
- Rarely presents with dysphagia, dysphonia or dyspnea
Board review style answer #1
C. Is associated with medullary thyroid carcinoma. Amyloid goiter is not associated with medullary thyroid carcinoma. It is defined as amyloid deposits in thyroid associated with a goiter, but not with a malignant neoplasm.
Comment Here
Reference: Amyloid goiter
Comment Here
Reference: Amyloid goiter

