

Thyroid & parathyroid
Thyroiditis
Hashimoto thyroiditis

Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Hashimoto thyroiditis
See Also: Fibrous (fibrosing) variant

- Prototype of autoimmune disease presenting with goiter, elevated circulating antithyroid antibodies, often with hypothyroidism
- Histopathologically diffuse lymphoplasmacytic infiltration, lymphoid follicle formation, follicular atrophy, oncocytic metaplasia and fibrosis
- First described in 1912 by Dr. Hakaru Hashimoto, who called it struma lymphomatosa (Thyroid 2013;23:142)
- Most common cause of hypothyroidism in iodine sufficient areas
- Infiltration of thyroid parenchyma by mononuclear cells, lymphoid follicles with germinal centers, oncocytic cells lining residual thyroid follicles, fibrosis
- Also known as Hashimoto disease, struma lymphomatosa, chronic lymphocytic thyroiditis, goitrous thyroiditis, lymphadenoid goitre
- Hashitoxicosis: transient thyrotoxicosis due to follicle destruction in Hashimoto thyroiditis
- ICD-10: E06.3 - autoimmune thyroiditis
- Incidence per year 0.3 - 1.5/1,000 (Best Pract Res Clin Endocrinol Metab 2019;33:101367)
- 30 - 50 years (Maedica (Bucur) 2019;14:98)
- F:M = 3 - 12:1 (Autoimmun Rev 2014;13:391)
- 3:1 for IgG4 related variant
- 5:1 for Hashitoxicosis form
- 6:1 for juvenile variant
- 10:1 for fibrous variant
- 12:1 for classic variant
- Polymorphisms associated with other autoimmune diseases in 20% of cases
- Breakdown of immune tolerance (Best Pract Res Clin Endocrinol Metab 2019;33:101367)
- Genetic susceptibility
- Familial aggregation
- Polymorphisms in human leukocyte antigen (HLA) genes
- Polymorphisms in genes involved in immune regulation, including cytotoxic T lymphocyte associated antigen 4 (CTLA4), protein tyrosine phosphatase 22 (PTPN22) and interlukin 2 receptor α chain (IL2RA)
- Environmental factors (Autoimmun Rev 2014;13:391)
- Smoking has a protective effect
- Increased dietary iodine is associated with increased incidence
- Polymorphisms
- Decrease in Tregs
- Genetic susceptibility
- Autoantibodies against thyroglobulin, thyroid peroxidase (TPO) and antithyroid stimulating hormone (TSH) receptor
- CD8+ T cell mediated cytotoxicity, cytokine mediated cell death and antibody dependent cell mediated cytotoxicity
- Multifactorial; immunological, genetic and environmental

- Painless enlargement of thyroid gland
- Majority (75%) are euthyroid (Autoimmun Rev 2014;13:391)
- Progressively increasing hypothyroidism
- May have an initial transient phase of hyperthyroidism
- May coexist with other autoimmune diseases, like type 1 diabetes mellitus, Addison disease, systemic lupus erythematosus, Sjögren syndrome, pernicious anemia, myasthenia gravis, vitiligo, celiac disease, chronic active hepatitis
- Increased risk of primary thyroid lymphoma and papillary thyroid carcinoma (PTC) (Front Oncol 2017;7:53, Endocr Pathol 2021;32:368)
- 6 clinicopathologic forms: classic, fibrous variant, IgG4 related variant, juvenile form, Hashitoxicosis and painless (or silent) thyroiditis (Autoimmun Rev 2014;13:391)
- Idiopathic myxedema in older patients with fibrous variant
- Juvenile variant: < 18 years of age, (mean age of 11 years); usually asymptomatic thyroid swelling
- Hashitoxicosis variant: initial hyperthyroid phase similar to Graves disease, followed by hypothyroidism
- Painless thyroiditis: sporadic or (more commonly) postpartum (within 12 months of delivery); usually self limited
- Diagnostic workup is similar to any thyroid swelling
- Thyroid function test
- Serum antithyroid antibody levels
- Ultrasound neck
- Fine needle aspiration cytology (FNAC) if thyroid nodule present
- References: J Endocrinol Invest 2021;44:883, Autoimmun Rev 2020;19:102649
- Deranged thyroid function tests
- Elevated levels of TSH, with normal or low serum thyroid hormones (T3,T4)
- Decreased TSH, with normal or increased serum T3,T4
- Elevated serum antithyroid antibodies
- Antithyroglobulin
- Anti-TPO
- Anti-TSH receptor
- References: J Endocrinol Invest 2021;44:883, Autoimmun Rev 2020;19:102649
- Sonography: diffusely enlarged thyroid gland; diffusely heterogeneous, coarse and hypoechogenic parenchyma with micronodular pattern (Eur J Endocrinol 2019;181:539, AJR Am J Roentgenol 2010;195:208)
- IgG4 related variant: more marked hypoechogenicity (Autoimmun Rev 2014;13:391)
- Fibrous variant: hypoechogenicity along with prominent nodularity of the parenchyma
Contributed by Ayana Suzuki, C.T.
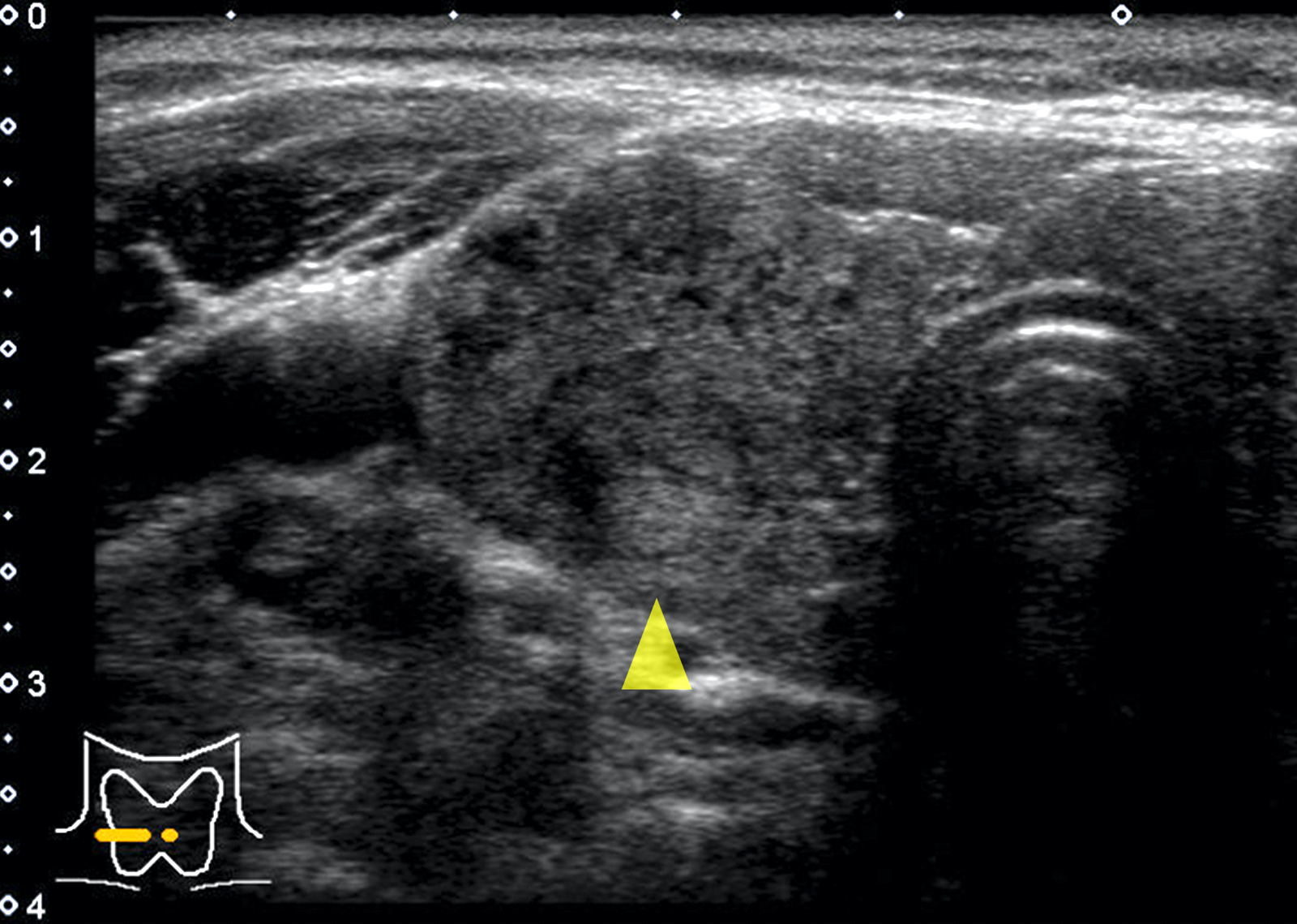
Isoechoic nodule
Images hosted on other servers:
Ultrasound
Ultrasound
- IgG4 related variant shows a more aggressive clinical course, with more severe and treatment resistant hypothyroidism (Autoimmun Rev 2014;13:391)
- 24 year old woman with Hashimoto thyroiditis associated with inflammatory myopathy (Pathology 2017;49:97)
- 28 year old woman with RET / PTC1 rearrangement in Hashimoto thyroiditis and in associated papillary thyroid carcinoma and hyalinizing trabecular adenoma (AJSP Reviews & Reports 2019;24:13)
- 31 year old man with Hashimoto thyroiditis presented with myxedema psychosis (J Am Osteopath Assoc 2017;117:50)
- 41 year old woman with hypothyroidism and multinodular goiter (Arch Pathol Lab Med 2003;127:e253)
- 43 year old woman with coexisting affective psychosis and brain perfusion abnormalities (Clin Pract Epidemiol Ment Health 2007;3:31)
- 46 year old woman with thyroid adenoma and Hashimoto thyroiditis (Rom J Morphol Embryol 2017;58:241)
- 52 year old woman with Hashimoto thyroiditis involving ectopic cervical thyroid tissue (Head Neck Pathol 2021;15:328)
- Thyroid hormone replacement if hypothyroid
- Subtotal thyroidectomy to relieve compression symptoms (Best Pract Res Clin Endocrinol Metab 2019;33:101367)
- Hemitotal or subtotal thyroidectomy in case of oncocytic cell neoplasm or suspicious for malignancy cytology
- Short course glucocorticoids in IgG4 related variant (Autoimmun Rev 2014;13:391)
- Diffuse symmetric enlargement of thyroid gland; occasionally asymmetric enlargement or nodular
- Cut surface: pale, yellow-tan, firm, nodular; resembles lymph nodes
- May be fibrotic and atrophied
Contributed by Mark R. Wick, M.D.
Diffusely enlarged thyroid lobe
Images hosted on other servers:
Atrophic gland
Nodular gland
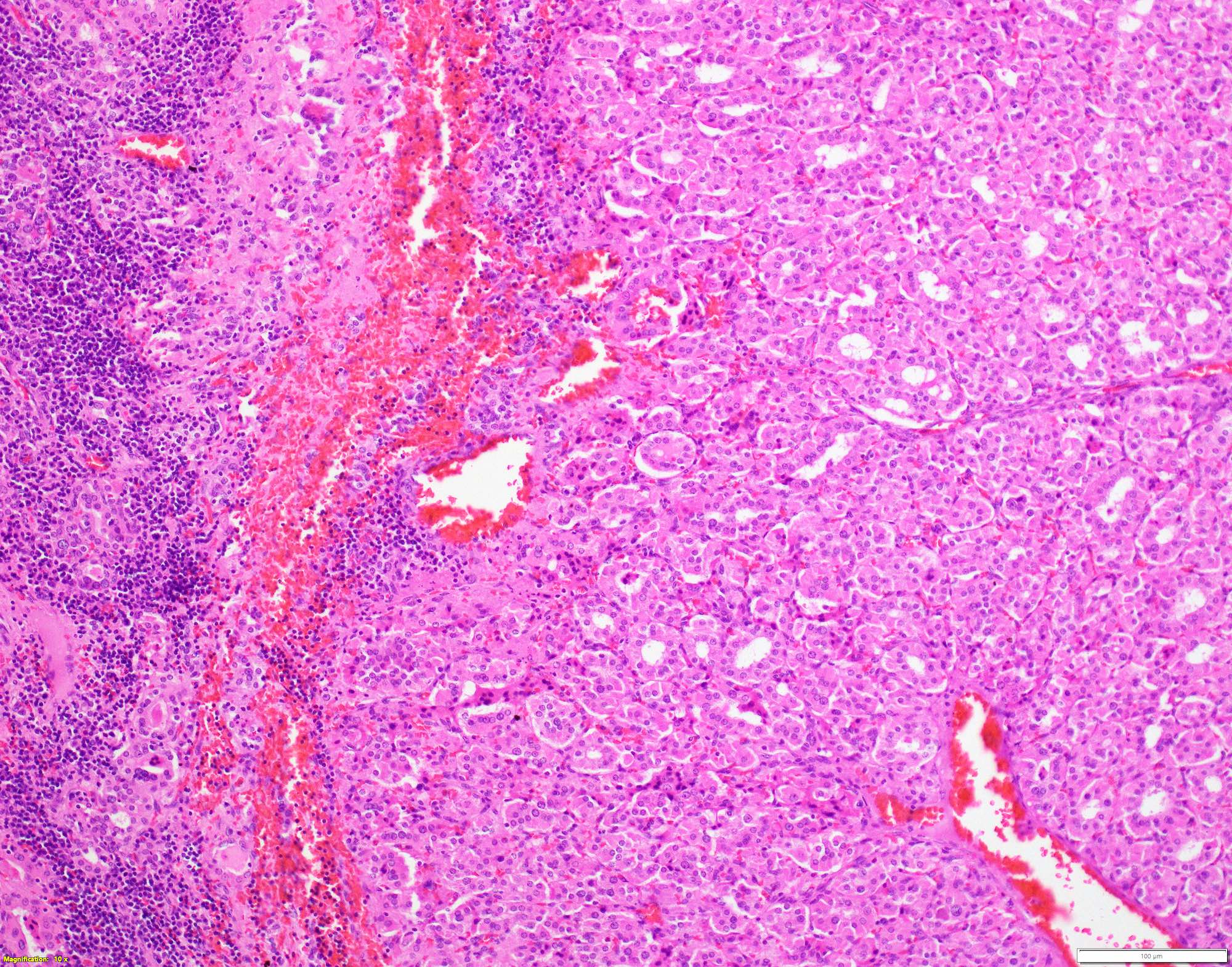
- Classic form: diffuse infiltration of thyroid parenchyma with lymphocytes and plasma cells; lymphoid follicle formation with germinal centers (Best Pract Res Clin Endocrinol Metab 2019;33:101367)
- Polymorphic lymphocytic infiltrate, predominantly T cells
- Thyroid follicular destruction
- Atrophic thyroid follicles; many lined by oncocytic cells / oncocytes having abundant granular eosinophilic cytoplasm; rarely squamous metaplasia
- Later fibrosis and nodularity (Virchows Arch 2013;462:557)
- Fibrous (or fibrosing) variant: extensive keloid-like fibrosis of thyroid parenchyma, fibrous septa divide the parenchyma into lobules, mononuclear cell infiltration, lymphoid follicles, thyroid follicular atrophy, oncocytic cell and squamous metaplasia (Autoimmun Rev 2014;13:391)
- IgG4 related variant: dense lymphoplasmacytic infiltrate, enriched in IgG4 producing plasma cells (> 20 cells per high power field); interstitial fibrosis; often associated with obliterative phlebitis (Autoimmun Rev 2014;13:391)
- Juvenile thyroiditis, Hashitoxicosis and painless thyroiditis: rare / absent germinal center formation and follicular atrophy, follicular cell hyperplasia, less pronounced oncocytic cell metaplasia and fibrosis (Autoimmun Rev 2014;13:391)
- Variable atypia of follicular cells and oncocytic cells, may mimic and act as a precursor (limited evidence) of papillary thyroid carcinoma (Endocr Pathol 2021;32:368)
- Squamous metaplasia of follicular epithelium can be confused with solid cell nests (J Clin Endocrinol Metab 2012;97:2209)
- May be associated with colloid goiter, follicular neoplasm, oncocytic cell neoplasm, papillary thyroid carcinoma and primary thyroid lymphoma (Acta Cytol 2009;53:507, Front Oncol 2017;7:53)
Contributed by Andrey Bychkov, M.D., Ph.D. and Shipra Agarwal, M.D.
Lymphoid follicles with germinal centers
Diffuse
lymphoplasmacytic
infiltration
Squamous metaplasia: p63+ cells in many follicles
Evolution of squamous metaplasia
Intense immunostaining
Lobulation of thyroid tissue by fibrotic bands
Vesicular nuclei of thyroid follicles similar to PTC nuclei
Aggregation of lymphoid follicles mimic thyroid nodule
Hashimoto thyroiditis with lymphoepithelial cyst
Nodular Hashimoto thyroiditis
Papillary microcarcinoma and Hashimoto thyroiditis
Oncocytic cell nodule
Images hosted on other servers:

Fibrous variant of Hashimoto thyroiditis

Lymphoid follicles and oncocytic metaplasia

Dense infiltrate and atrophied follicles

Oncocytic metaplasia

Fibrous variant with squamous metaplasia

Oncocytic and adenomatous nodules

Oncocytic nodule
- Moderately or highly cellular aspirate
- Inflammatory infiltrate
- Variable number of lymphocytes in different stages of development (Cureus 2019;11:e5851, J Thyroid Res 2018;2018:5246516)
- Lymphocytes infiltrating follicular epithelial cells
- Lymphoglandular bodies (Acta Cytol 2009;53:507)
- Plasma cells
- Can grade based on lymphocytic infiltration from 0 to 3+ (see Diagrams / tables) but does not correlate with clinical, biochemical, radionuclide and ultrasonographic parameters (Cytojournal 2007;4:10, J Cytol 2016;33:145)
- Aggregates of oncocytic cells / oncocytes
- Crushed cells, lymphoid tangles
- Absent or scant colloid
- Mild anisonucleosis, giant cells, macrophages, epithelioid cells, eosinophils, fire flares
- Usually Bethesda System for Reporting Thyroid Cytopathology (TBSRTC) category II; can be TBSRTC III / IV / V
Contributed by Shipra Agarwal, M.D. and Ayana Suzuki, C.T.
Cellular aspirate
Crushed cells

Lymphocytes and oncocytes
Images hosted on other servers:
Oncocytic cells with atypical nuclei
Sheet of follicular cells with oncocytic change mixed with benign lymphoid cells
Resembles lymphoma
Grade I: mild lymphocytic inflammatory infiltrate
Grade II: moderate lymphocytic inflammation
Grade III: marked
inflammation with
polymorphous
lymphocytes
ThinPrep versus Pap stain

Lymphocytes and oncocytes


Follicular destruction by lymphocytes

Crushed cells
Grade 1, 2 and 3 thyroiditis
- High molecular weight keratin, p63 (Hum Pathol 2003;34:764)
- May have elevated kappa/lambda ratio (Am J Clin Pathol 2006;125:42)
- Mixture of T and B cells (Indian J Pathol Microbiol 2011;54:464)
- HBME-1, cytokeratin 19, cyclin D1, galectin3: variable positivity in case of atypia (Virchows Arch 2013;462:557, Endocr Pathol 2021;32:368)
- Oncocytic cells have numerous large mitochondria
- Polyclonal (Hum Pathol 1988;19:1444, Indian J Pathol Microbiol 2011;54:464)
- No mutations, gene fusions (previously reported RET / PTC rearrangements were erroneous)
Thyroid: compare and contrast
Histopathology thyroid: Hashimoto thyroiditis
- Thyroid, total thyroidectomy:
- Hashimoto thyroiditis
- Chronic (focal) lymphocytic thyroiditis:
- Incidental detection of focal aggregates of lymphocytes, with or without germinal center formation, in thyroid parenchyma
- Absent or limited oncocytic metaplasia
- Follicular atrophy and fibrosis
- Usually absent clinical and laboratory indicators of autoimmune thyroid disease
- Riedel thyroiditis:
- Hard fixed mass simulating thyroid carcinoma
- Active fibroblastic proliferation; storiform fibrosis
- Inflammation and fibrosis extends beyond the thyroid capsule into perithyroidal tissues
- Associated with fibroinflammatory lesions in other sites
- MALT lymphoma:
- Age: > 60 years
- Rapid increase in size of thyroid swelling, hard swelling
- Clonal proliferation of B cells, confirmed on immunostaining and flow cytometry
- Destructive lymphoepithelial lesions (Rom J Morphol Embryol 2017;58:731)
- Oncocytic cell neoplasms:
- Well circumscribed lesion within an echonormal background
- Composed mainly of oncocytic cells without (or with minimal) mononuclear cell infiltration (Rom J Morphol Embryol 2017;58:731)
- Papillary carcinoma:
- Presence of true papillae, more well developed and diffuse nuclear features, infiltrative borders
- Lithium intake:
- Significant clinical history; shows similar morphologic findings (Hum Pathol 1983;14:737)
Which of the following is true regarding the thyroid lesion shown above?
- Fibrosis extends into perithyroidal soft tissues
- Increased risk of follicular thyroid carcinoma
- Increased risk of medullary thyroid carcinoma
- Increased risk of primary thyroid lymphoma
- Shows monoclonal lymphoid cell proliferation
Comment Here
Reference: Hashimoto thyroiditis
- Common in iodine deficient areas
- Mononuclear cell infiltration of the thyroid parenchyma
- More common in males
- Not a familial disease
- Usually presents with hyperthyroidism
Comment Here
Reference: Hashimoto thyroiditis

