
Uterus
Nontumor
Arias-Stella reaction
Author: Laura Ardighieri, M.D.
Editorial Board Member: Stephanie L. Skala, M.D.
Deputy Editor-in-Chief: Jennifer A. Bennett, M.D.

Last author update: 13 January 2023
Last staff update: 13 January 2023
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed search: Arias-Stella reaction uterus

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Frozen section description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Ardighieri L. Arias-Stella reaction. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/uterusariasstella.html. Accessed April 17th, 2024.
Definition / general
- Reactive and benign phenomenon of the endometrium induced by hormonal stimulation and characterized by cytomegaly and nuclear enlargement of endometrial glands; typically associated with intrauterine or extrauterine pregnancies or with gestational trophoblastic disease
Essential features
- Pseudoneoplastic glandular response of the female genital tract, first described by Javier Arias-Stella in 1954 as atypical endometrial changes associated with the presence of chorionic tissue (AMA Arch Pathol 1954;58:112)
- Typically found in the endometria of postabortion curettings of intrauterine or extrauterine pregnancies or with gestational trophoblastic disease; however, it can occur anywhere in the epithelium of female genital tract during pregnancy and under hormonal intake
- Endometrial glands are lined by enlarged or hobnail cells, characterized by abundant eosinophilic, cleared to vacuolated cytoplasm and by hyperchromatic, pleomorphic and smudged nuclei with hobnail appearance; however N:C ratio is maintained (Am J Surg Pathol 2004;28:608)
- Usually easy to recognize because it predominantly affects young and pregnant patients; however, it may occasionally raise concern for carcinoma if detected in nonpregnant or older patients (Int J Gynecol Pathol 1994;13:241)
- Most important differential diagnosis is clear cell carcinoma (Am J Surg Pathol 2019;43:325)
- Rarely can be seen in nonpregnant patients on hormonal therapy (oral contraceptives, ovulation inducing drugs and hormone replacement therapies and phytoestrogens) and more rarely in patients without hormonal treatment (Diagn Cytopathol 2005;32:94)
Terminology
- Arias-Stella phenomenon, Arias-Stella change, Arias-Stella effect
ICD coding
- ICD-11: GA1Y - other specified noninflammatory disorders of female genital tract
Epidemiology
- Relatively common phenomenon
- May be seen in up to 50% of gravid hysterectomies
- Arias-Stella changes in endometrial glands are observed in 80% of cases of intrauterine abortions (Arch Gynecol Obstet 2007;276:47)
- Can occur as early as 17 days postconception (Arch Pathol Lab Med 1978;102:651)
- Most commonly occurs in reproductive aged women and in the background of pregnancy; however, it may be seen in women of all ages and in any type of hormonal alteration (exogenous and endogenous)
Sites
- Typically found in gestational endometrium (focal or in a substantial portion of the endometrium)
- Involved glands are located in the spongiosa but occasionally in the basalis
- Surface epithelium may also be affected (Adv Anat Pathol 2002;9:12)
- Also occurs in adenomyosis and adenomyomatous polyp of the uterus and in endometria of postabortion curettings of intrauterine or extrauterine pregnancies, moles and choriocarcinoma (Acta Obstet Gynecol Scand 2007;86:106)
- Also endocervix, including endocervical polyps; this location frequently shows the monstrous cell pattern (giant and bizarre nuclei with frequent pseudoinclusions) (Adv Anat Pathol 2002;9:12)
- Extrauterine sites:
- In the epithelia of fallopian tube (Am J Clin Pathol 1991;95:892, Arch Gynecol Obstet 2007;276:47)
- Foci of endometriosis (peritoneal, subcutaneous, umbilicus, urinary bladder) (Pathol Res Pract 2009;205:653)
- Paraovarian and paratubal cysts (Acta Cytol 2001;45:627)
- Vaginal adenosis (Adv Anat Pathol 2002;9:12)
- Ovarian germinal inclusion cysts, luteal cysts of puerperium and gestation, ovarian mucinous cystadenomas (Acta Obstet Gynecol Scand 1986;65:505)
Pathophysiology
- Represents a cellular transdifferentiation process: conversion of a differentiated cell type into another cell type (Adv Anat Pathol 2002;9:12)
- Hormone related atypical endometrial reaction, related to the effects of estrogens and progesterone acting simultaneously (Adv Anat Pathol 2002;9:12)
- Very rarely, Arias-Stella reaction (ASR) can occur in the absence of pregnancy or hormonal intake, also in foci of endometriosis (J Clin Diagn Res 2016;10:ED03)
Etiology
- Increase or imbalance of hormones
- Associated with:
- Pregnancy (AMA Arch Pathol 1954;58:112)
- Gestational trophoblastic disease (AMA Arch Pathol 1954;58:112)
- Oral contraceptives and ovulation inducing drugs (Diagn Cytopathol 2005;32:94)
- Postmenopausal women taking hormone replacement therapies (Int J Gynecol Pathol 1994;13:241)
- High dose progestin for endometrial hyperplasia or low grade endometrial carcinoma: ASR may be seen in background endometrium or hyperplastic / neoplastic epithelium, where the persistence of nuclear atypia does not always signify treatment failure (Virchows Arch 2018;472:907)
- Phytoestrogen use (Int J Gynecol Pathol 2010;29:185)
Clinical features
- Incidental finding
Diagnosis
- Microscopic finding on histological samples
- Arias-Stella glandular changes can also be present in cytological material obtained from cervix and vagina through Pap test during pregnancy and postpartum (Acta Cytol 1980;24:328, Acta Cytol 1983;27:28, Acta Cytol 1995;39:905)
Laboratory
- Increased serum levels of beta human chorionic gonadotropin (βhCG) in gestational cases
Radiology description
- Ultrasonography can reveal a pregnancy (intrauterine or extrauterine)
Prognostic factors
- Benign condition that typically regresses postpartum
Case reports
- 21 year old woman with missed abortion, with signet ring-like cells within endometrial glands with ASR (Int J Surg Pathol 2018;26:283)
- 30 year old nonpregnant woman with ASR in a cervicovaginal smear (Diagn Cytopathol 2005;32:94)
- 31 year old nonpregnant woman with coexistence of endometriosis and ASR (J Clin Diagn Res 2016;10:ED03)
- 45 year old woman with endometrioid carcinoma of the endometrium with superimposed ASR related to medroxyprogesterone intake (Int J Surg Pathol 2016;24:330)
- 48 year old woman with polypoid cervical endometriosis with a superficial growth pattern (Int J Gynecol Pathol 2010;29:185)
Treatment
- Benign condition that does not need treatment
Gross description
- Does not typically form mass lesion
- May extensively involve pre-existing polyp
Frozen section description
- Since Arias-Stella can be found anywhere in the female genital tract and outside it in ectopic endometrial glands (e.g., in endometriotic lesions), in view of the presence of giant cells with coarse chromatin and macronucleoli, a false positive diagnosis of malignancy can be made during intraoperative examination if the clinician does not provide information regarding current or recent pregnancy or hormonal treatment (J Clin Diagn Res 2016;10:ED03, AMA Arch Pathol 1954;58:112)
- ASR can occasionally be mistaken for clear cell carcinoma; differentiation from it is made by the lack of stromal invasion, as well as by the absence of the classic tubular and papillary areas typical of clear cell carcinoma and the lack of mitotic activity (Am J Surg Pathol 2019;43:325)
- In pregnant patients, diagnosis of malignancy should be made with caution when evaluating frozen sections
Microscopic (histologic) description
- Endometrial glands lined by large polyhedral cells with abundant eosinophilic cytoplasm with large hyperchromatic, pleomorphic and smudged nuclei
- Focal or diffuse: can involve portion of a gland, a single gland or a different number of glands
- Affected glands may have micropapillary or cribriform growth and intraglandular papillary epithelial tufts; occasionally they can be confluent cells protruding into the lumen, with nuclei placed at the bulbous shaped apical portion of the cytoplasm, imparting hobnail appearance
- Absence of stromal invasion
- Dr. Arias-Stella classified the histologic variants into 5 types (Adv Anat Pathol 2002;9:12):
- Minimal atypia: characterized by mild nuclear enlargement
- Early secretory pattern: marked nuclear enlargement, subnuclear and supranuclear vacuoles
- Secretory or hypersecretory pattern: enlarged nuclei and intense and diffuse cytoplasmic vacuolization
- Regenerative, proliferative or nonsecretory pattern: nuclei with a vesicular configuration with glands showing no / minimal secretory activity
- Monstrous cell pattern: nuclei show giant and bizarre forms with homogenous chromatin and frequent pseudoinclusions
- Mitotic figures in the ASR are rare and thus, frequent or atypical mitoses should raise concern for adenocarcinoma
Microscopic (histologic) images
Contributed by Ayse Ayhan, M.D., Ph.D.
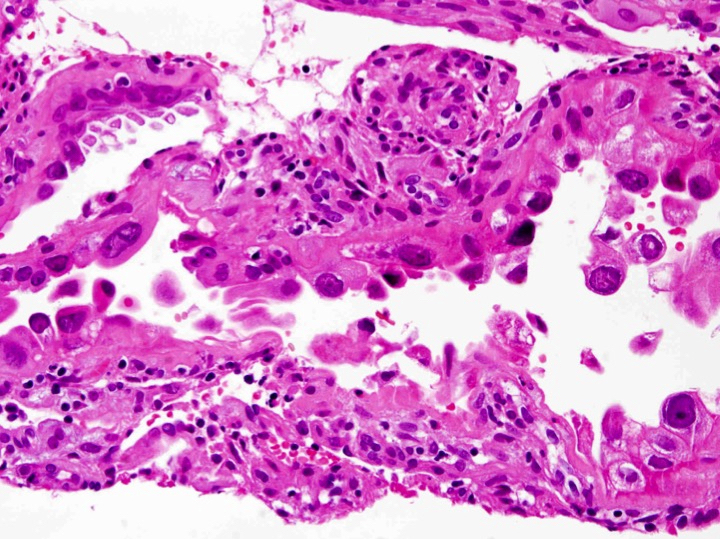

Enlarged nuclei, sub / supranuclear vacuoles
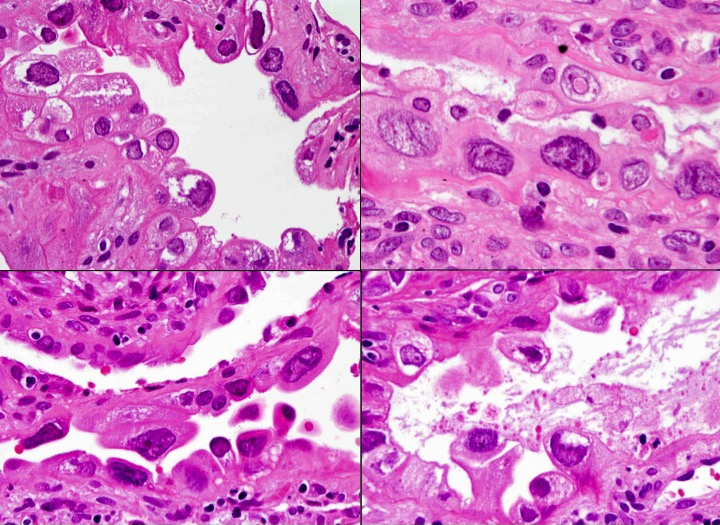
Hobnail growth pattern
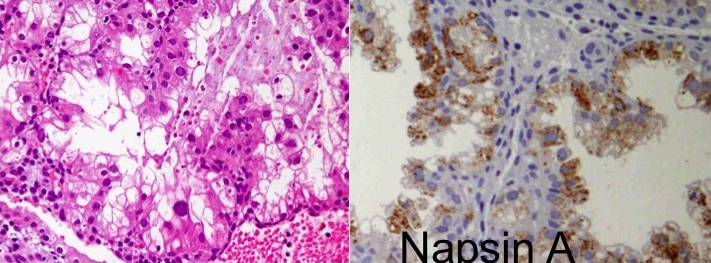
Napsin A positivity
Cytology description
- Cellular enlargement, to double or many times the normal size
- Abundant eosinophilic, clear to vacuolated cytoplasm
- Hypertrophied and hyperchromatic nuclei of ovoid or round shape with irregular nuclear contours and variable chromatin patterns (smudgy, open, even)
- Normal N:C ratio
- Mitotic figures in 10 - 15% of cases; rarely can be atypical or numerous (Arch Pathol Lab Med 1981;105:116)
Positive stains
- ER / PR (lower than in proliferative phase endometrium) (Int J Gynecol Pathol 2004;23:223)
- Cytokeratin AE1 / AE3, CAM5.2 and cytokeratin 7 (epithelial glandular component) and EMA (Pathol Res Pract 2009;205:653, Acta Cytol 1997;41:285)
- Vimentin and CD10 (decidual component) (Pathol Res Pract 2009;205:653)
- p53 and Ki67: diminished staining in ASR (Int J Gynecol Pathol 2004;23:223)
Negative stains
- CK20 (Pathol Res Pract 2009;205:653)
- ASS1 (argininosuccinate synthase 1): 63.6% sensitive and 95.1% specific for ASR (Int J Gynecol Pathol 2020;39:344)
Electron microscopy description
- Overall few organelles; sparse particles that resemble granules of ribonucleic acid in the clear cells
- Conspicuous Golgi apparatus, vesicles of endoplasmic reticulum, numerous mitochondrial crests and Palade grains in the dark cells
- Presence of parallel rows of rough endoplasmic reticulum (Am J Obstet Gynecol 1964;89:661, Am J Obstet Gynecol 1972;112:113, Am J Clin Pathol 1991;95:892)
Molecular / cytogenetics description
- Nuclei of ASR cells enlarge because of DNA polyploid contents; aneuploidy is absent (Adv Anat Pathol 2002;9:12)
Sample pathology report
- Endometrium, biopsy:
- Gestational endometrium with Arias-Stella reaction
Differential diagnosis
- Clear cell / serous carcinoma of the endometrium:
- No concurrent pregnancy
- Absence of stromal decidual reaction or hypersecretory glands
- Presence of glandular mitotic figures
- Presence of desmoplasia and stromal invasion
- Presence of mass lesion
- Endometrial intraepithelial carcinoma:
- Mitotically active and high proliferative activity
- Nucleus highly atypical with prominent nucleoli
- p53 abnormal
- Ischemic or reactive atypia of endometrium:
- Stromal necrosis is usually present
- Microglandular and mesonephric hyperplasia:
- Small polypoid lesion or erosion
- Usually nuclei are uniform without atypia
- No hobnail cells
- GATA3 positivity
- Invasive or in situ adenocarcinoma of the cervix:
- Colposcopically or macroscopically visible lesion
- Increased proliferative activity and frequent mitotic and apoptotic figures
- Disturbance of glandular architecture, common nuclear stratification
- p16 INK4a diffuse and strong
- Radiation atypia of the cervix:
- Mostly history
Board review style question #1
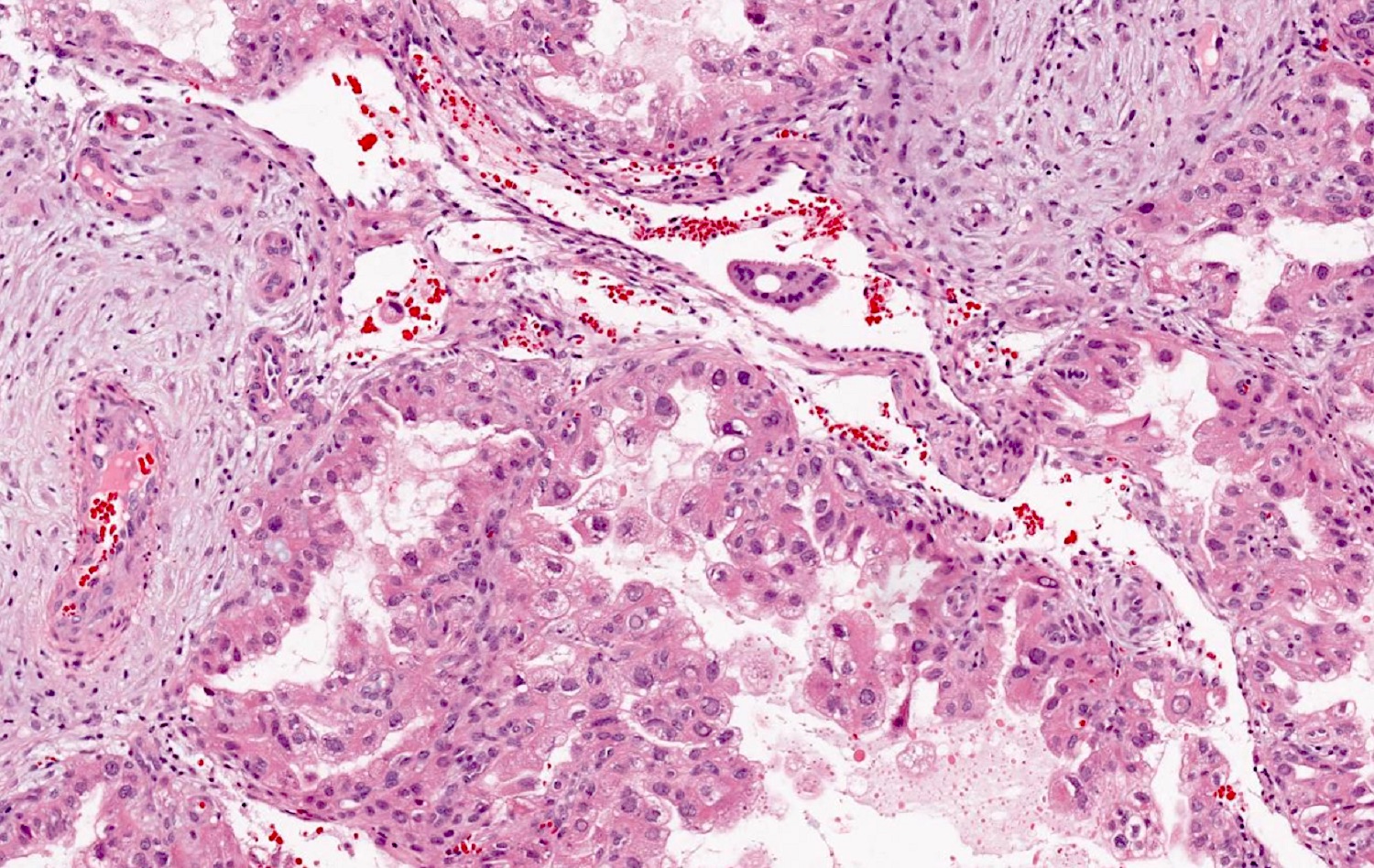
The finding in the figure above is found in gestational endometrium. What is the diagnosis?
- Arias-Stella reaction
- Clear cell carcinoma
- Endometrioid carcinoma
- Endometritis
Board review style answer #1
Board review style question #2
Where can the Arias-Stella phenomenon occur?
- Anywhere in the female genital tract
- In the endometrium only
- In the uterine cervix
- Only in gestational endometrium
Board review style answer #2
