Strategic plan to substantially reduce cancer deaths
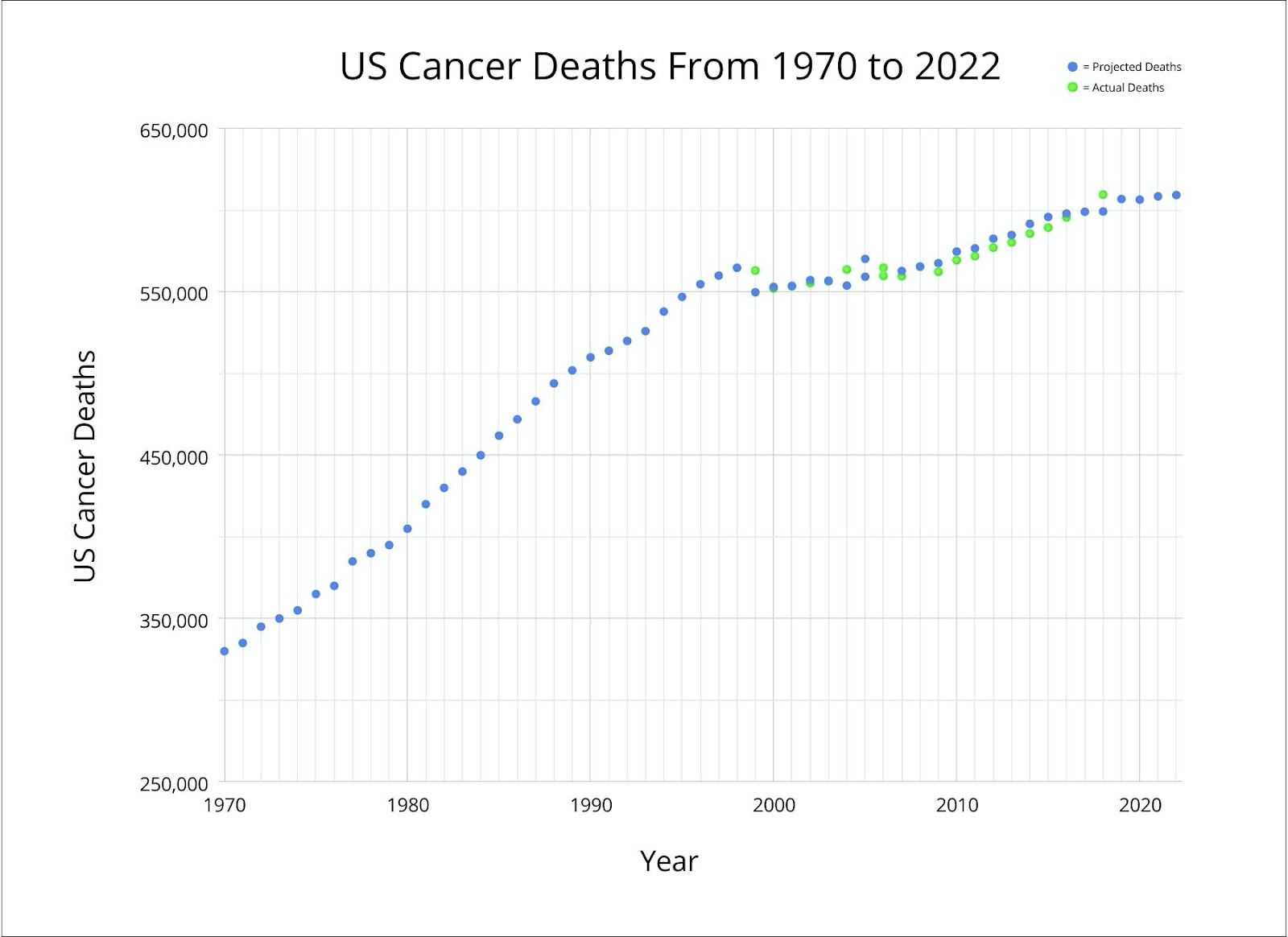
This strategic plan, created in February 2021, aims to substantially reduce cancer deaths in the United States from 600,000 projected for 2022 to 100,000 per year. After 50 years of fighting the War on Cancer (NCI: National Cancer Act of 1971, accessed 23Sep22), we need to "dare greatly" (The Man in the Arena 1910, retrieved 23Sep22), to determine our desired cancer related goals (Pernick: Let's cure cancer together 2021) and how we might attain them, even if many steps are unknown. Thus, our strategic plan differs from "challenge goals" that are based on "applying known interventions broadly and equitably" (Ma 2019).
This strategic plan to substantially reduce cancer deaths is essentially a management plan to use all of the treatment and public health approaches possible that may impact cancer deaths (Pernick: Curing cancer - Curative cancer treatment based on complexity theory 2022). We will not be successful by focusing on a "silver bullet" or other miracle treatment that might theoretically solve all of our problems (Pernick: What should our national cancer goals be 2022). Instead, success will likely arise from an expanding number of modest improvements with occasional bursts of major successes (Pernick: What will success look like in the war on cancer 2021).
We should be honest about what we can and cannot do. We cannot achieve "a world without cancer" (American Cancer Society Mission Statement, accessed 23Sep22). Cancer will always be with us because (a) multicellular organisms are based on self-organized critical states with a predictable risk of catastrophic system failure in the form of cancer (Pernick: The Laws of Complexity and Self-organization: A Framework for Understanding Neoplasia 2017); (b) we cannot eliminate personal behavior that promotes cancer, such as tobacco use and being overweight (Pernick: Curing Cancer Blog - What should our national cancer goals be 2021); and (c) we cannot eliminate random chronic stress, a major contributor to lung, pancreatic and other cancers (Pernick: Curing cancer - Random chronic stress / bad luck as a major cause of cancer 2022).
In addition, even with curative treatments available, cancer deaths cannot be reduced to zero; therefore, proposing a goal of a very small number of deaths is not sensible. Many patients will still die from cancer due to treatment noncompliance, medical conditions which interfere with treatment, treatment error, treatment failure for unknown reasons and the development of additional cancers.
Our specific strategies are:
1. Treatment should target as many individual biologic networks as possible that contribute to the cancer itself, directly or indirectly, and our public policies must optimize all aspects of our healthcare system that affect cancer deaths.
Cancer arises in individuals due to multiple disruptions to interacting biological networks. These networks are physiologically at a "tipping point" that leads to more chaotic, premalignant states (Pernick: Curing cancer - Reductionism versus complexity 2022), but typically maintains resistance against change through redundant control systems (Pernick: How Cancer Arises Based on Complexity Theory 2017). Chronic disturbances affecting different aspects of the networks may ultimately overcome these controls and produce premalignant or malignant cells that acquire their own type of stability ("cancer attractors") that are resistant to change (Huang 2009). For individual patients, we will need treatment consisting of multiple disruptions to tumor networks and other systemic networks that nurture the malignant process and constitute an altered systems biology (Koutsogiannouli 2013). At a societal level, we will need improvements in our healthcare system regarding prevention, reducing healthcare disparities and making treatment options more available.
2. Successful treatment will likely require combinations of combinations of therapy.
Childhood leukemia is curable using combinations of therapies that target cancer cell growth (Pomeroy 2022). Treating adult solid tumors should build on this success by using combinations of therapy for as many aspects of cancer as possible; this includes not only cancer cell growth but its microenvironment (Pernick: Strategic plan for curing cancer, initial version 2021), metastases and their microenvironment, systemic inflammation which drives the malignant process, the damaged immune system that tolerates or promotes the cancer cells, hormones that push cells towards malignancy and DNA variations present at birth that advance the malignant process. It should also reflect the heterogeneity common in solid tumors (de Sousa 2018, Punt 2017).
We speculate that for each cancer type, even the most aggressive, there exists a combination of 8-10 therapies that individually may be only partially effective but together can be substantially effective in reducing cancer deaths (Pernick: Combinations of therapy to substantially reduce cancer deaths 2021). No single therapy is likely to eradicate most adult cancer cells and restore order to the large number of networks altered during the malignant process; i.e. focusing solely on driver mutations alone is unlikely to be curative (Pernick: Combinations of therapy to substantially reduce cancer deaths 2021). To determine the optimal combinations, we may need to develop 30 or more partially effective therapies to choose from (Pernick: Pancreatic cancer update 2021) and use machine learning, cell lines, animal models and ultimately clinical trials to test the huge number of potential combinations (Pernick: Strategic plan to cure cancer 2021). Successful treatment plans may also involve moving cancer cells that survive treatment into less aggressive networks (Pernick: Curing cancer - Curative cancer treatment based on complexity theory 2022, Pernick: How Lung Cancer Arises, Based on Complexity Theory 2021).
For long term success, we must also reduce the chronic cellular stressors / risk factors that promoted the original cancer (Pernick: How Cancer Arises Based on Complexity Theory 2017) and will continue to promote premalignant and malignant conditions unless stopped.
3. We should initially focus on aggressive cancers that cause the most cancer deaths.
To substantially reduce US cancer deaths, we should focus on the leading causes of cancer death, namely most cancers of the lung, pancreas and liver and aggressive cancers of the colon, breast and prostate (Pernick: What will success look like in the war on cancer 2021). Successful treatments for these sites may be useful for cancer at less common sites.
4. We should reduce cancer deaths that occur shortly after diagnosis.
Many patients with cancer die within 90 days of diagnosis, which can be attributed to noncancer causes (Zaorsky 2017, Yang 2021). Although these patients have advanced cancers at diagnosis (McPhail 2013, Suhail 2019), we speculate that these deaths are immediately due to cancer related alterations in essential physiologic pathways which can be countered using treatment available today; this is analogous to treating new onset diabetes presenting with life threatening ketoacidosis (Pernick: Curing Cancer Blog: Part 9 - How cancer kills 2021).
In addition, we can reduce early treatment related cancer deaths by focusing more on managing cancer instead of killing all cancer cells (Pernick: Curing cancer - Curative cancer treatment based on complexity theory 2022, Huang 2014) and by better anticipating and treating infections that often kill cancer patients (Zheng 2021, Van de Louw 2020).
5. We should incorporate therapeutic strategies that delay cancer deaths.
We can prolong the lifespan of patients with cancer by achieving "marginal gains" at all steps of the disease process (Powell-Brett 2021); this may increase possible treatment options and reduce the sense of futility associated with cancer death (Pernick: Curing Cancer Blog: Part 9 - How cancer kills 2021). In addition, honoring patient therapeutic preferences may improve survival (Balogh 2011, Tsvitman 2021).
6. We should focus on reducing age related cancer deaths.
The incidence of most malignancies increases exponentially with age during adulthood. More than two thirds of invasive cancers occur at age 60 years or older (White 2019, Benz 2008) and advancing age is the most important risk factor for cancer overall and for many individual cancer types (Pernick: How Cancer Arises Based on Complexity Theory 2017). Since cancer incidence is projected to increase by almost 50% due to the growth and aging of the US population, a greater emphasis on cancer risk reduction is needed (Weir 2021).
7. We should aggressively enroll patients into clinical trials so physicians can learn and improve.
Clinical trials can compare the current standard therapy for a particular risk group with a potentially better treatment that may improve survival or reduce treatment side effects. They are particularly important to test whether treatment combinations will be effective and tolerable in different patient groups (Pernick: Curing cancer - Adult versus childhood cancer 2022).
8. We should make our prevention programs more effective.
Between 30-50% of cancer deaths can be prevented by dramatically reducing tobacco use and excess weight, improving diets (more non starchy vegetables, fruit, fiber and whole grains and less fat, sugar and processed food), reducing alcohol use (particularly heavy, long term use, LoConte 2017), increasing vaccinations against HPV and Hepatitis B, treating infections and infestations that predispose to cancer (Plummer 2016, de Martel 2020, Ferrara 2020, Nguyen 2020, Gredner 2018, Pernick: How cancer arises from chronic inflammation, based on complexity theory 2021), reducing other risk factors and implementing other evidence based prevention strategies (World Health Organization, accessed 23Sep22, GBD 2019 Cancer Risk Factors Collaborators 2022). This also includes targeting risk factors that are important for only specific cancer types, such as "nonuse of screening" for colorectal cancer (Pernick: How colorectal cancer arises and treatment approaches, based on complexity theory 2020).
Reducing even a single risk factor may have a disproportionate impact because a combination of multiple risk factors are typically needed in order to sufficiently disturb the networks necessary to overcome redundant controls and promote the malignant process. Optimizing one risk factor may also improve other related risk factors (e.g. reducing cigarette smoking may improve behavior related to diet, exercise and alcohol).
We need strong public health programs at all governmental levels to act as a behavioral immune system (Pernick: How Pancreatic Cancer Arises Based on Complexity Theory 2021) and to reduce cancer death. Government, as well as nonprofits, the business community and others, should promote programs and policies, such as the American Code Against Cancer, that advance a culture of being healthy and make one's own health a priority. In addition, to the extent possible, all institutions should develop and implement their own cancer action plans.
We should also optimize access to medical care that reduces cancer deaths. This includes providing care to all patient populations and reducing disparities based on race or ethnicity, region of residence and socioeconomic status (Ma 2019, Michigan Cancer Plan 2021-2030 (PDF)).
9. We should develop better screening programs for cancers with high mortality.
This includes earlier detection of lung, pancreatic and liver cancers; aggressive colorectal, breast and prostate cancers and life threatening second cancers (Zaorsky 2017). We should study whether screening for the chronic inflammation associated with many cancers is useful and if so, how best to do it (Pernick: How cancer arises from chronic inflammation, based on complexity theory 2021).
To substantially reduce cancer deaths requires a regularly updated strategy incorporating all of these proposed policies. Let's get to work!
This strategic plan to substantially reduce cancer deaths is essentially a management plan to use all of the treatment and public health approaches possible that may impact cancer deaths (Pernick: Curing cancer - Curative cancer treatment based on complexity theory 2022). We will not be successful by focusing on a "silver bullet" or other miracle treatment that might theoretically solve all of our problems (Pernick: What should our national cancer goals be 2022). Instead, success will likely arise from an expanding number of modest improvements with occasional bursts of major successes (Pernick: What will success look like in the war on cancer 2021).
We should be honest about what we can and cannot do. We cannot achieve "a world without cancer" (American Cancer Society Mission Statement, accessed 23Sep22). Cancer will always be with us because (a) multicellular organisms are based on self-organized critical states with a predictable risk of catastrophic system failure in the form of cancer (Pernick: The Laws of Complexity and Self-organization: A Framework for Understanding Neoplasia 2017); (b) we cannot eliminate personal behavior that promotes cancer, such as tobacco use and being overweight (Pernick: Curing Cancer Blog - What should our national cancer goals be 2021); and (c) we cannot eliminate random chronic stress, a major contributor to lung, pancreatic and other cancers (Pernick: Curing cancer - Random chronic stress / bad luck as a major cause of cancer 2022).
In addition, even with curative treatments available, cancer deaths cannot be reduced to zero; therefore, proposing a goal of a very small number of deaths is not sensible. Many patients will still die from cancer due to treatment noncompliance, medical conditions which interfere with treatment, treatment error, treatment failure for unknown reasons and the development of additional cancers.
Our specific strategies are:
1. Treatment should target as many individual biologic networks as possible that contribute to the cancer itself, directly or indirectly, and our public policies must optimize all aspects of our healthcare system that affect cancer deaths.
Cancer arises in individuals due to multiple disruptions to interacting biological networks. These networks are physiologically at a "tipping point" that leads to more chaotic, premalignant states (Pernick: Curing cancer - Reductionism versus complexity 2022), but typically maintains resistance against change through redundant control systems (Pernick: How Cancer Arises Based on Complexity Theory 2017). Chronic disturbances affecting different aspects of the networks may ultimately overcome these controls and produce premalignant or malignant cells that acquire their own type of stability ("cancer attractors") that are resistant to change (Huang 2009). For individual patients, we will need treatment consisting of multiple disruptions to tumor networks and other systemic networks that nurture the malignant process and constitute an altered systems biology (Koutsogiannouli 2013). At a societal level, we will need improvements in our healthcare system regarding prevention, reducing healthcare disparities and making treatment options more available.
2. Successful treatment will likely require combinations of combinations of therapy.
Childhood leukemia is curable using combinations of therapies that target cancer cell growth (Pomeroy 2022). Treating adult solid tumors should build on this success by using combinations of therapy for as many aspects of cancer as possible; this includes not only cancer cell growth but its microenvironment (Pernick: Strategic plan for curing cancer, initial version 2021), metastases and their microenvironment, systemic inflammation which drives the malignant process, the damaged immune system that tolerates or promotes the cancer cells, hormones that push cells towards malignancy and DNA variations present at birth that advance the malignant process. It should also reflect the heterogeneity common in solid tumors (de Sousa 2018, Punt 2017).
We speculate that for each cancer type, even the most aggressive, there exists a combination of 8-10 therapies that individually may be only partially effective but together can be substantially effective in reducing cancer deaths (Pernick: Combinations of therapy to substantially reduce cancer deaths 2021). No single therapy is likely to eradicate most adult cancer cells and restore order to the large number of networks altered during the malignant process; i.e. focusing solely on driver mutations alone is unlikely to be curative (Pernick: Combinations of therapy to substantially reduce cancer deaths 2021). To determine the optimal combinations, we may need to develop 30 or more partially effective therapies to choose from (Pernick: Pancreatic cancer update 2021) and use machine learning, cell lines, animal models and ultimately clinical trials to test the huge number of potential combinations (Pernick: Strategic plan to cure cancer 2021). Successful treatment plans may also involve moving cancer cells that survive treatment into less aggressive networks (Pernick: Curing cancer - Curative cancer treatment based on complexity theory 2022, Pernick: How Lung Cancer Arises, Based on Complexity Theory 2021).
For long term success, we must also reduce the chronic cellular stressors / risk factors that promoted the original cancer (Pernick: How Cancer Arises Based on Complexity Theory 2017) and will continue to promote premalignant and malignant conditions unless stopped.
3. We should initially focus on aggressive cancers that cause the most cancer deaths.
To substantially reduce US cancer deaths, we should focus on the leading causes of cancer death, namely most cancers of the lung, pancreas and liver and aggressive cancers of the colon, breast and prostate (Pernick: What will success look like in the war on cancer 2021). Successful treatments for these sites may be useful for cancer at less common sites.
4. We should reduce cancer deaths that occur shortly after diagnosis.
Many patients with cancer die within 90 days of diagnosis, which can be attributed to noncancer causes (Zaorsky 2017, Yang 2021). Although these patients have advanced cancers at diagnosis (McPhail 2013, Suhail 2019), we speculate that these deaths are immediately due to cancer related alterations in essential physiologic pathways which can be countered using treatment available today; this is analogous to treating new onset diabetes presenting with life threatening ketoacidosis (Pernick: Curing Cancer Blog: Part 9 - How cancer kills 2021).
In addition, we can reduce early treatment related cancer deaths by focusing more on managing cancer instead of killing all cancer cells (Pernick: Curing cancer - Curative cancer treatment based on complexity theory 2022, Huang 2014) and by better anticipating and treating infections that often kill cancer patients (Zheng 2021, Van de Louw 2020).
5. We should incorporate therapeutic strategies that delay cancer deaths.
We can prolong the lifespan of patients with cancer by achieving "marginal gains" at all steps of the disease process (Powell-Brett 2021); this may increase possible treatment options and reduce the sense of futility associated with cancer death (Pernick: Curing Cancer Blog: Part 9 - How cancer kills 2021). In addition, honoring patient therapeutic preferences may improve survival (Balogh 2011, Tsvitman 2021).
6. We should focus on reducing age related cancer deaths.
The incidence of most malignancies increases exponentially with age during adulthood. More than two thirds of invasive cancers occur at age 60 years or older (White 2019, Benz 2008) and advancing age is the most important risk factor for cancer overall and for many individual cancer types (Pernick: How Cancer Arises Based on Complexity Theory 2017). Since cancer incidence is projected to increase by almost 50% due to the growth and aging of the US population, a greater emphasis on cancer risk reduction is needed (Weir 2021).
7. We should aggressively enroll patients into clinical trials so physicians can learn and improve.
Clinical trials can compare the current standard therapy for a particular risk group with a potentially better treatment that may improve survival or reduce treatment side effects. They are particularly important to test whether treatment combinations will be effective and tolerable in different patient groups (Pernick: Curing cancer - Adult versus childhood cancer 2022).
8. We should make our prevention programs more effective.
Between 30-50% of cancer deaths can be prevented by dramatically reducing tobacco use and excess weight, improving diets (more non starchy vegetables, fruit, fiber and whole grains and less fat, sugar and processed food), reducing alcohol use (particularly heavy, long term use, LoConte 2017), increasing vaccinations against HPV and Hepatitis B, treating infections and infestations that predispose to cancer (Plummer 2016, de Martel 2020, Ferrara 2020, Nguyen 2020, Gredner 2018, Pernick: How cancer arises from chronic inflammation, based on complexity theory 2021), reducing other risk factors and implementing other evidence based prevention strategies (World Health Organization, accessed 23Sep22, GBD 2019 Cancer Risk Factors Collaborators 2022). This also includes targeting risk factors that are important for only specific cancer types, such as "nonuse of screening" for colorectal cancer (Pernick: How colorectal cancer arises and treatment approaches, based on complexity theory 2020).
Reducing even a single risk factor may have a disproportionate impact because a combination of multiple risk factors are typically needed in order to sufficiently disturb the networks necessary to overcome redundant controls and promote the malignant process. Optimizing one risk factor may also improve other related risk factors (e.g. reducing cigarette smoking may improve behavior related to diet, exercise and alcohol).
We need strong public health programs at all governmental levels to act as a behavioral immune system (Pernick: How Pancreatic Cancer Arises Based on Complexity Theory 2021) and to reduce cancer death. Government, as well as nonprofits, the business community and others, should promote programs and policies, such as the American Code Against Cancer, that advance a culture of being healthy and make one's own health a priority. In addition, to the extent possible, all institutions should develop and implement their own cancer action plans.
We should also optimize access to medical care that reduces cancer deaths. This includes providing care to all patient populations and reducing disparities based on race or ethnicity, region of residence and socioeconomic status (Ma 2019, Michigan Cancer Plan 2021-2030 (PDF)).
9. We should develop better screening programs for cancers with high mortality.
This includes earlier detection of lung, pancreatic and liver cancers; aggressive colorectal, breast and prostate cancers and life threatening second cancers (Zaorsky 2017). We should study whether screening for the chronic inflammation associated with many cancers is useful and if so, how best to do it (Pernick: How cancer arises from chronic inflammation, based on complexity theory 2021).
To substantially reduce cancer deaths requires a regularly updated strategy incorporating all of these proposed policies. Let's get to work!
