
Stains & CD markers
p16
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: p16 [title]


p16
Last author update: 1 July 2017
Last staff update: 25 January 2024
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: p16 [title]

Table of Contents
Definition / general | Essential features | Terminology | Interpretation | Uses by pathologists | Microscopic (histologic) images | Positive staining - malignant | Positive staining - not malignant | Board review style question #1 | Board review style answer #1Cite this page: Hodgson A, Parra-Herran C. p16. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/stainsp16.html. Accessed May 13th, 2024.
Definition / general
- Tumor suppressor protein encoded by CDKN2A gene (9p21.3)
- Prevents progression into S phase of cell cycle
- Inhibits cyclin D dependent protein kinases (CDK4 and CDK6) therefore maintaining Rb in its hypophosphorylated state which prevents its dissociation from E2F transcription factor
- Protein expression often increased in aging cells, which eventually drives cell death and apoptosis (Exp Cell Res 1997;237:7)
- Protein function is silenced or lost in many non HPV related tumors by epigenetic or genetic abnormalities, including promoter CpG methylation or less commonly by mutations
- Examples include breast carcinoma, colon carcinoma, pancreatic carcinoma, head and neck carcinoma related to smoking and melanoma
Essential features
- Expression can be detected by immunohistochemistry
- Negative IHC in tumors with loss of p16 protein function / expression
- Immunohistochemical positivity commonly considered a surrogate marker for oncogenic HPV infection
- Inactivation of Rb by the viral E7 oncoprotein following viral integration into host genome leads to overexpression of p16 (Arch Pathol Lab Med 2007;131:1343)
- Positivity also seen in lesions with inactivation of Rb due to HPV independent mechanisms, such as Rb gene alterations or other mechanisms of Rb pathway dysregulation
- Includes liposarcoma, gastric adenocarcinoma, Hodgkin and non-Hodgkin lymphoma, pulmonary adenocarcinoma, neuroendocrine carcinoma and a subset of uterine carcinoma
- Most commonly studied and used in the evaluation of anogenital lesions (cervical, vulvar, vaginal, anal, penile)
- Also useful in the evaluation of head and neck carcinoma (specifically oropharyngeal carcinoma - tonsils, base of tongue)
- Increasingly used in the evaluation of different gynecologic tract tumors: p16 overexpression is more frequently seen in high grade endometrial and ovarian carcinoma (serous, clear cell, high grade endometrioid) compared to low grade tumors (Adv Anat Pathol 2009;16:267, Int J Gynecol Pathol 2009;28:179)
- More frequently overexpressed in uterine leiomyosarcoma, in comparison to STUMP, leiomyoma and inflammatory myofibroblastic tumor (Int J Clin Exp Pathol 2015;8:2795, Histopathol 2017;70:1138)
- Limited value in the workup of unknown primaries, as the protein is expressed in a variety of tumors from a variety of sites (Hum Pathol 2012;43:327)
Terminology
- p16 protein, also known as multiple tumor suppressor 1 (MTS1) or cyclin dependent kinase inhibitor 2A; also known as p16 INK4a
Interpretation
- Positive staining is defined as "block" staining: strong nuclear and cytoplasmic expression in a continuous segment of cells (at least 10 - 20 cells); in squamous epithelium, block positivity needs to involve basal and parabasal layers
- Positive staining (overexpression) correlates with oncogenic HPV infection and HPV independent mechanisms as outlined above
- In addition, complete absence of staining is also abnormal, since it has been correlated with CDKN2A gene silencing mutations (Histopathol 2017;70:1138)
- Cytoplasmic only staining, diffuse blush / weak intensity staining and other focal / patchy patterns should be considered negative (Arch Pathol Lab Med 2012;136:1266)
Uses by pathologists
- In the evaluation of HPV associated anogenital lesions
- Marker for detecting transcriptionally active HPV in oropharyngeal squamous cell carcinoma (Am J Surg Pathol 2010;34:1088)
- Differentiation of endocervical from endometrial carcinoma (Int J Gynecol Pathol 2003;22:231)
- Positive result favors primary endocervical adenocarcinoma
- Morphological subtyping of different gynecologic tumors
- Positive result is more common in high grade carcinoma
- The Lower Anogenital Squamous Terminology Standardization Project for HPV associated Lesions made these recommendations for p16 use:
- If the differential diagnosis is between precancer (–IN 2 or –IN 3) and either a mimic of precancer or a low grade / non HPV associated lesion; strong and diffuse block positive p16 results support a categorization of precancerous disease
- If there is a professional disagreement in histologic interpretation, when the differential diagnosis includes a precancerous lesion (–IN 2 or –IN 3)
- As an adjunct to morphologic assessment for biopsy specimens interpreted as ≤–IN 1 that are at high risk for missed high-grade disease, which is defined as a prior cytologic interpretation of HSIL, ASC-H, ASC-US/HPV-16 +, or AGC (NOS)
- p16 use is NOT recommended as a routine adjunct to histologic assessment of biopsy specimens with morphologic interpretations of negative, –IN 1 and –IN 3 (Arch Pathol Lab Med 2012;136:1266)
Microscopic (histologic) images
Contributed by Jijgee Munkhdelger, M.D., Ph.D. and Andrey Bychkov, M.D., Ph.D.
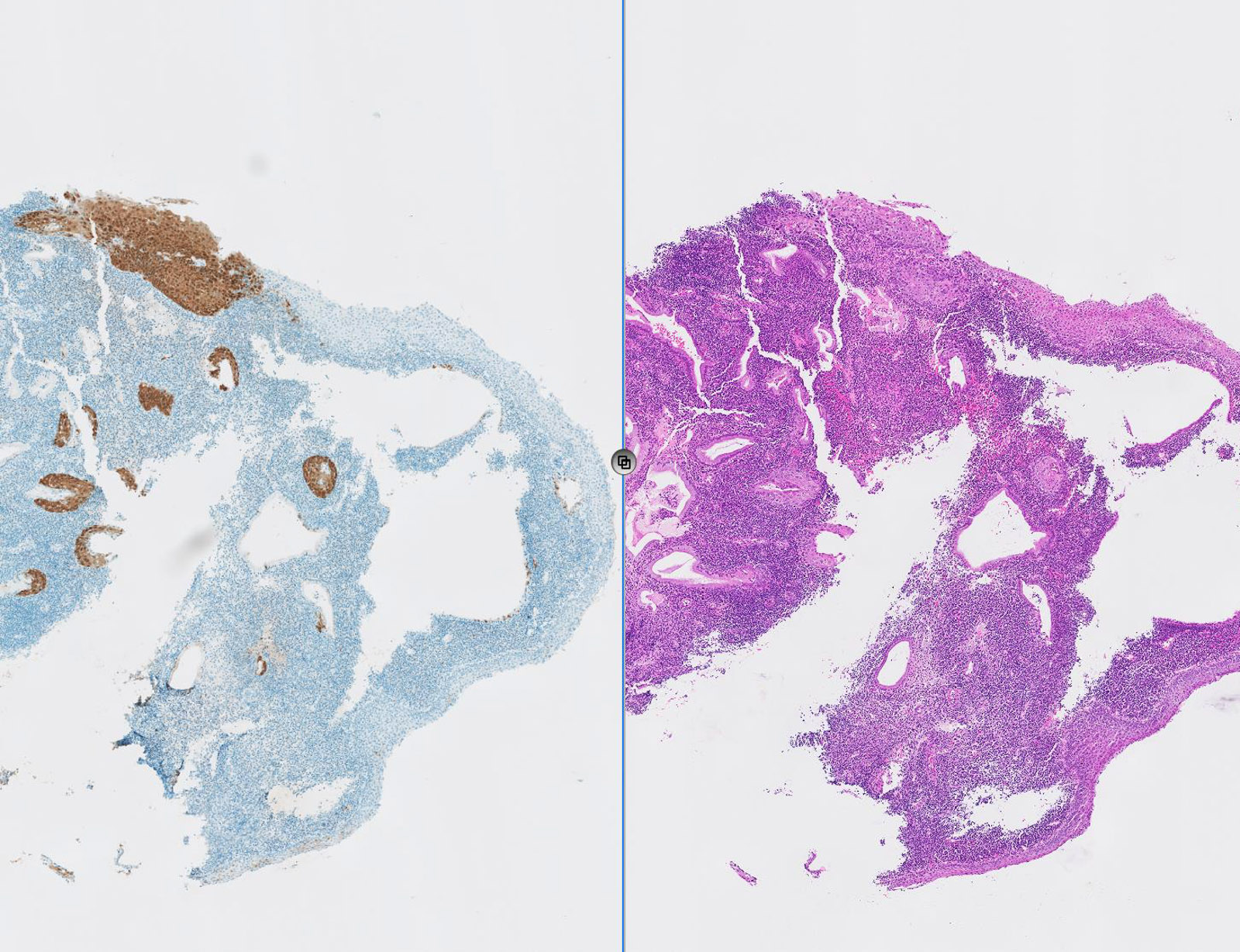
CIN 3 p16
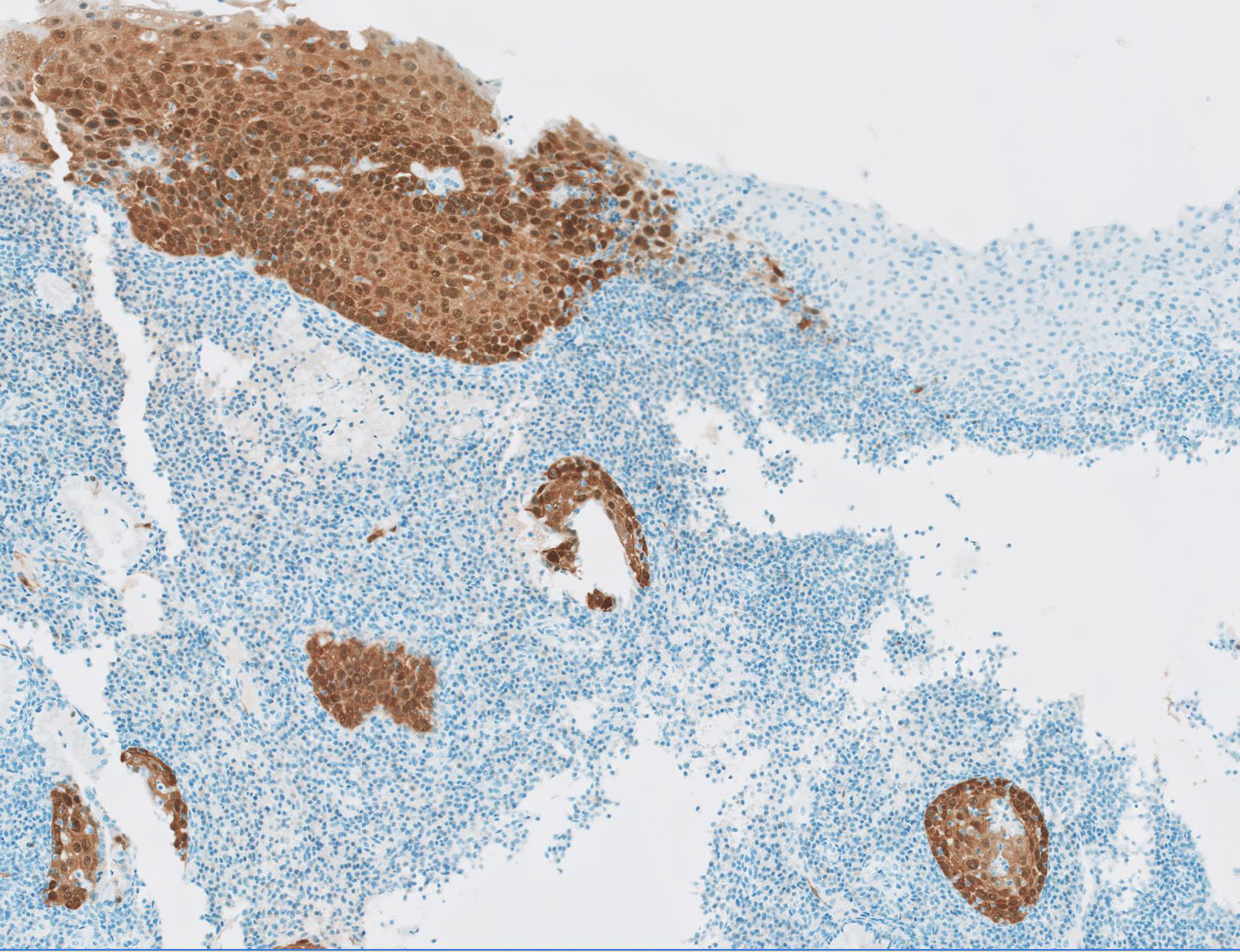
HSIL p16

AIS p16
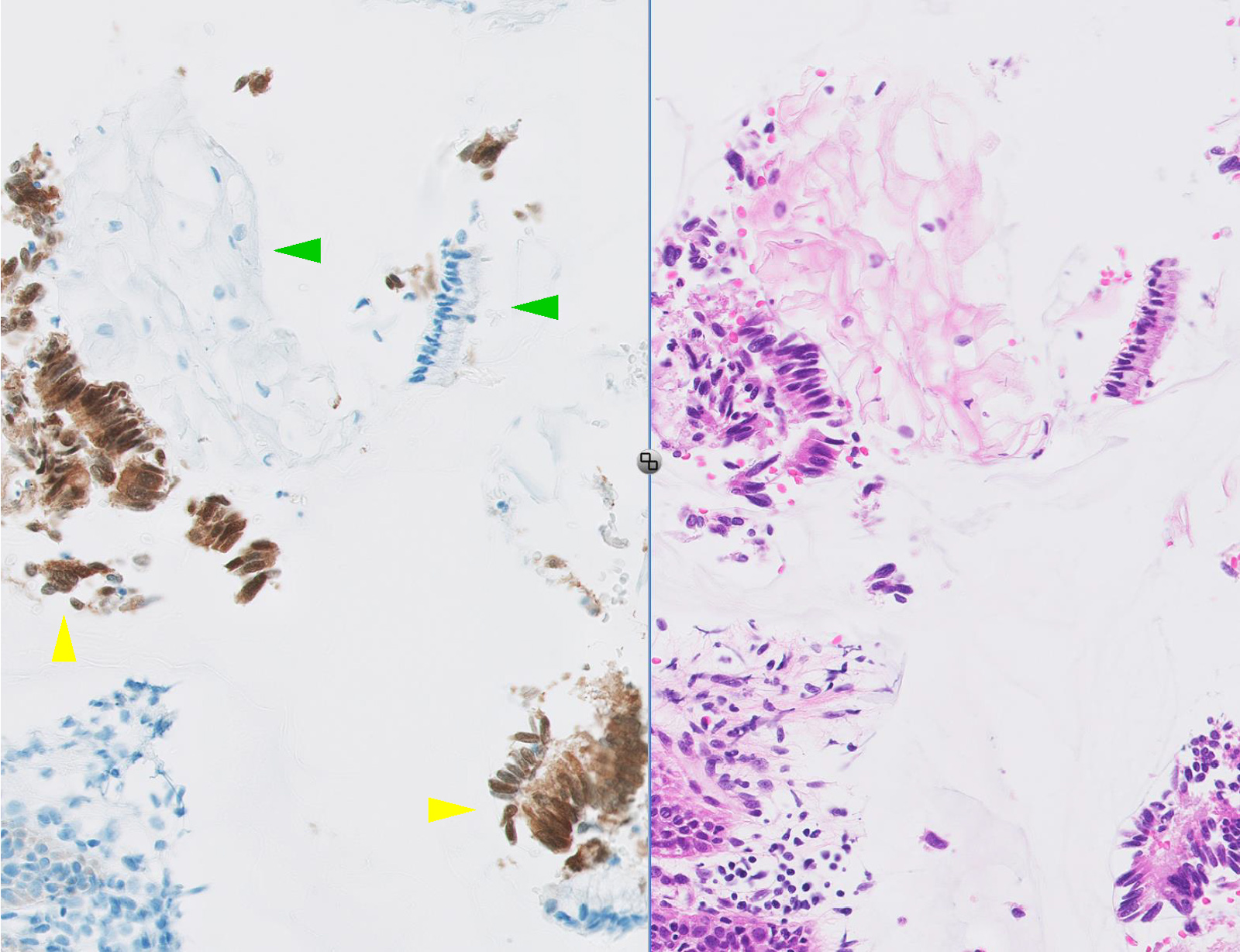
High grade cervical
glandular intraepithelial
neoplasia
Images hosted on other servers:

Diffuse strong staining in oropharyngeal carcinoma
Positive staining - malignant
- HPV related anogenital precursors (such as cervical SIL, Mod Pathol 2005;18:267), AIS, usual VIN, VAIN, undifferentiated PeIN)
- Squamous cell carcinoma (anogenital, oropharyngeal, some esophageal, some bladder)
- Endocervical adenocarcinoma
- Uterine serous carcinoma
- High grade serous carcinoma of Müllerian origin in general
- Some malignant mixed Müllerian tumors and undifferentiated carcinoma (Int J Gynecol Pathol 2012;31:57)
Positive staining - not malignant
- Branchial cleft cyst (Hum Pathol 2010;41:535)
- Endometrial tubal metaplasia (in a mosaic pattern) (seen in 15/15 cases Cell Oncol 2007;29:37)
Board review style question #1
According to the LAST Project working group recommendations, p16 immunohistochemistry is recommended in all of the following clinical scenarios involving anogenital squamous lesions, EXCEPT:
- Routinely in the evaluation of biopsies with interpretations of negative, CIN I or CIN III
- When a biopsy interpretation is < CIN I in the setting of a prior HSIL Pap smear
- When a diagnosis of CIN II is entertained by H&E morphologic interpretation
- When the H&E morphologic differential is between a precancerous (CIN II or CIN III) lesion and a mimic of a precancerous lesion (ex. immature squamous metaplasia, atrophy)
- When there is professional disagreement in histologic interpretation (when the differential diagnosis includes CIN I or III)
Board review style answer #1
A. p16 immunohistochemistry is not recommended as a routine adjunct assessment when the biopsy interpretation is negative, CIN I or CIN III.
Strong and diffuse block staining for p16 supports a categorization of precancerous disease. Any identified p16 positive area must meet H&E morphologic criteria for a high grade lesion to reinterpreted as such. (Arch Pathol Lab Med 2012;136:1266)
Comment Here
Reference: p16
Comment Here
Reference: p16

