
Stains & CD markers
PMS2
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: PMS2
PMS2
Author: Rebecca Obeng, M.D.
Last author update: 1 December 2016
Last staff update: 5 September 2023
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: PMS2

Table of Contents
Definition / general | Essential features | Terminology | Epidemiology | Sites | Pathophysiology | Etiology | Diagnosis | Prognostic factors | Case reports | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Molecular / cytogenetics descriptionCite this page: Obeng R. PMS2. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/stainspms2.html. Accessed May 13th, 2024.
Definition / general
- PMS2 is a component of the DNA mismatch repair system
- The PMS2 gene (on chromosome 7) encodes an endonuclease that forms a heterodimer with MLH1 to form the MutL alpha complex which is activated upon recognition of DNA mismatches, insertions or deletions by MutS alpha and MutS beta heterodimers
Essential features
- Germ line mutations in PMS2 are associated with increased risk of colorectal cancer, hereditary nonpolyposis colon cancer, Lynch syndrome, Turcot syndrome and endometrial cancer
- Milder microsatellite instability (less risk of developing cancer compared to MLH1 mutations)
- Deficiency in PMS2 is usually due to epigenetic repression (via mutations in or hypermethylation of MLH1)
Terminology
- PMS1 homolog 2, mismatch repair system component, HNPCC4, PMS2L, PMSL2, MLH4
Epidemiology
- Mutations in PMS2 have low penetrance for Lynch syndrome (35%) (Gastroenterology 2008;135:419)
- Colorectal cancer in patients with Lynch Syndrome:
- PMS2 mutations are associated with 15% - 20% in males and females (Exp Rev Mol Diagnostics 2016;16:591)
- Endometrial cancer:
- PMS2 mutation is associated with 12% - 15% increased risk of endometrial cancer (J Clin Oncol 2015;33:319, Exp Rev Mol Diagnostics 2016;16:591)
Sites
- Ubiquitous nuclear expression in normal tissue
Pathophysiology
- Genetic alterations in PMS2 contribute to DNA mismatch repair deficiency that leads to microsatellite instability and increased risk of cancer
- PMS2 is unstable in absence of MLH1
- Loss of expression of MLH1 due to mutations generally leads to loss of expression PMS2 as well (Adv Anat Pathol 2009;16:405; Exp Rev Mol Diagnostics 2016;16:591)
Etiology
- Germline or sporadic mutations in PMS2 lead to microsatellite instability
Diagnosis
- Screening: immunohistochemical (IHC) stain. Loss of nuclear
staining suggests microsatellite instability
- Lack of PMS2 staining is generally due to mutations in MLH1 and raises suspicion for germline mutations (Cancer Treat Rev 2016;51:19)
- Missense and point mutations that lead to nonfunctional protein can result in false negative results on IHC
- Confirmatory: molecular studies (PCR for microsatellite instability)
- High (MSI-H): at least 2 of 5 unstable markers or greater than or equal to 30% of unstable markers
- Low (MSI-L): one of five unstable markers or less than 30% of unstable markers
Prognostic factors
- Microsatellite instability due to mutations in PMS2 or other proteins is associated with better prognosis in comparison with microsatellite stable colorectal cancers (Ann Surg 1998;227:51; Clin Cancer Res 2005;11:8332; Ann Oncol 2013;24:1274; Cancer Epidemiol Biomarkers Prev 2001;10:917)
Case reports
- 15 year old girl with rectal cancer, with a novel MLH1 and MSH6 biallelic inheritance (Int J Colorectal Dis 2015;30:435)
- 34 year old woman with Lynch syndrome associated rectal cancer and novel PMS2 mutation (Jpn J Clin Oncol 2015;45:987)
Treatment
- Anti-PD-1 pathway blockade therapy for mismatch repair deficient colorectal cancers are in clinical trials with some showing significant objective response (Mod pathol 2009;22:1186; Clin Cancer Res 2013;19:462; N Engl J Med 2015;372:2509)
Microscopic (histologic) description
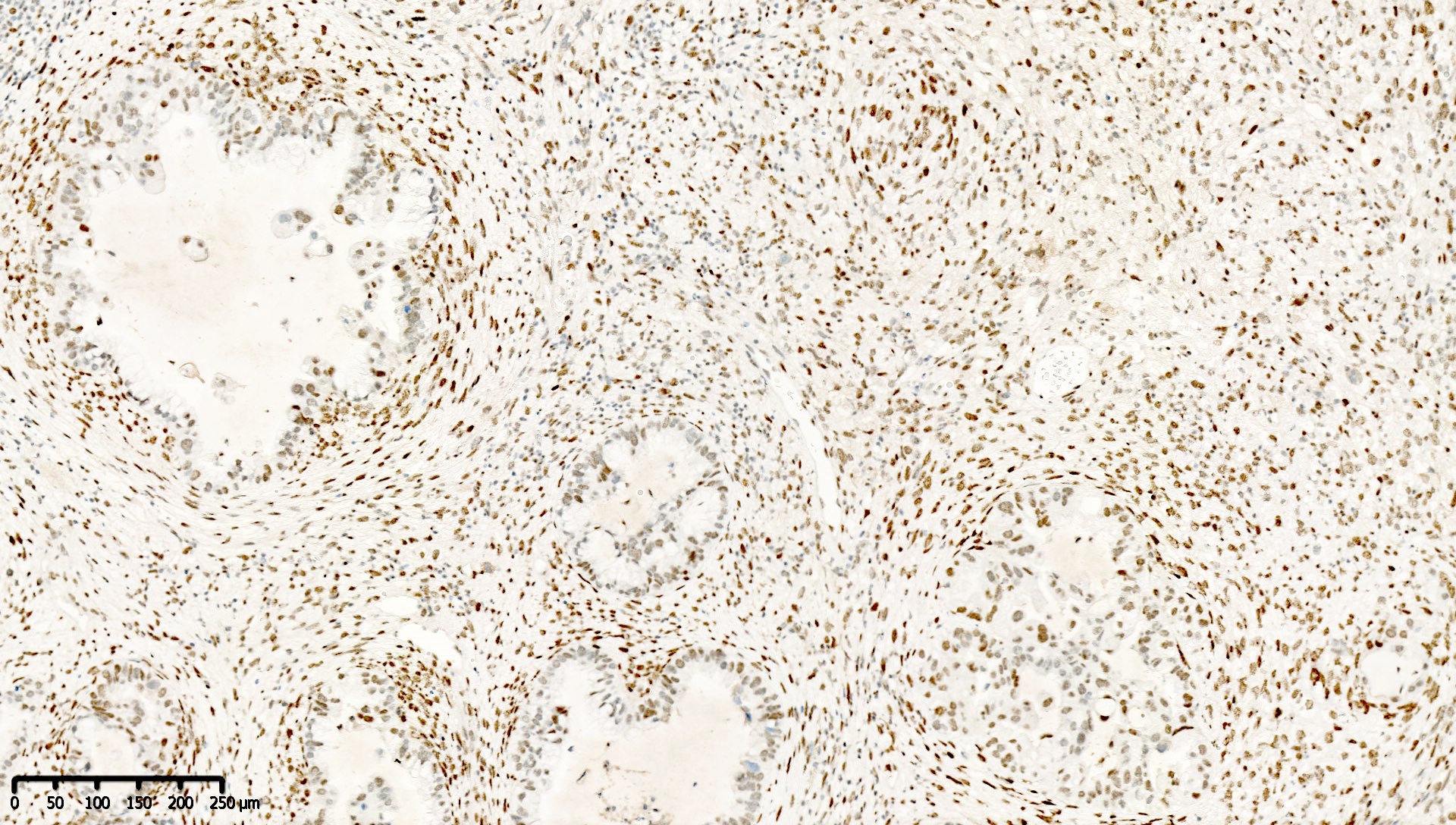
- Normal staining pattern: nuclear
- Cytoplasmic staining is abnormal and should not be misinterpreted as normal staining
Microscopic (histologic) images
Contributed by Mieke R. Van Bockstal, M.D., Ph.D., Jian-Hua Qiao, M.D. and Epitomics
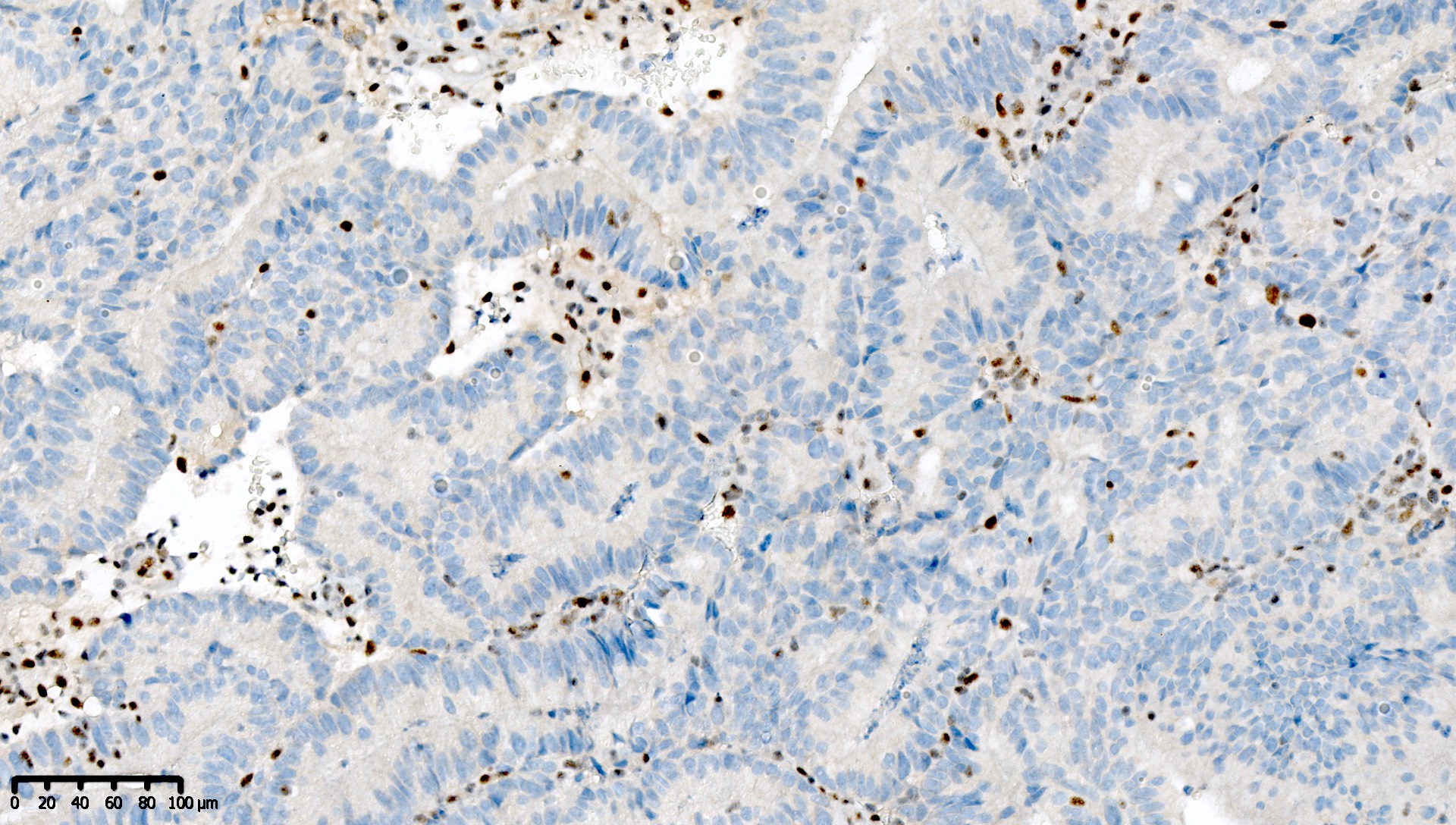
PMS2 deficient endometrioid carcinoma
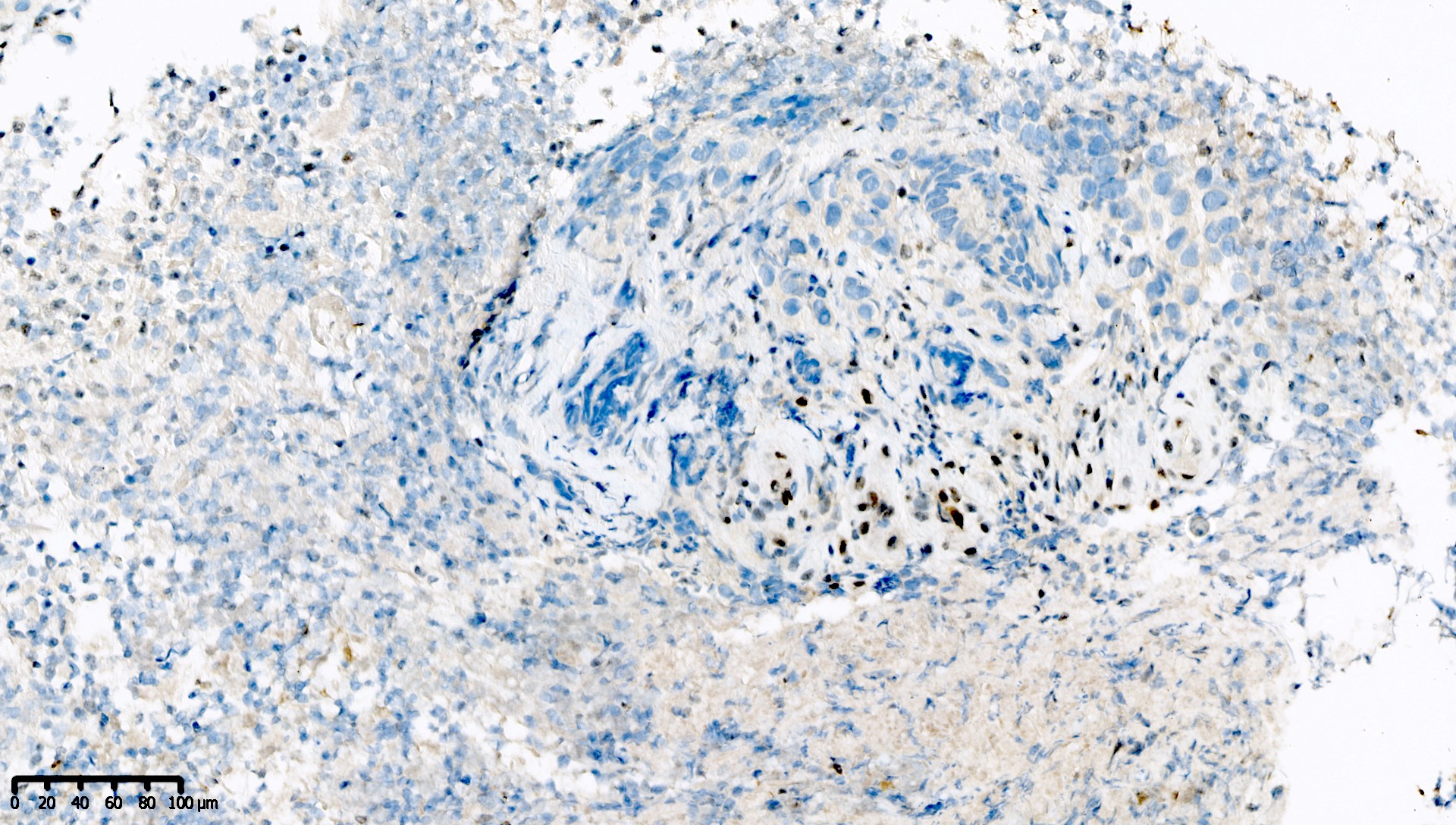
PMS2 deficient gastric carcinoma
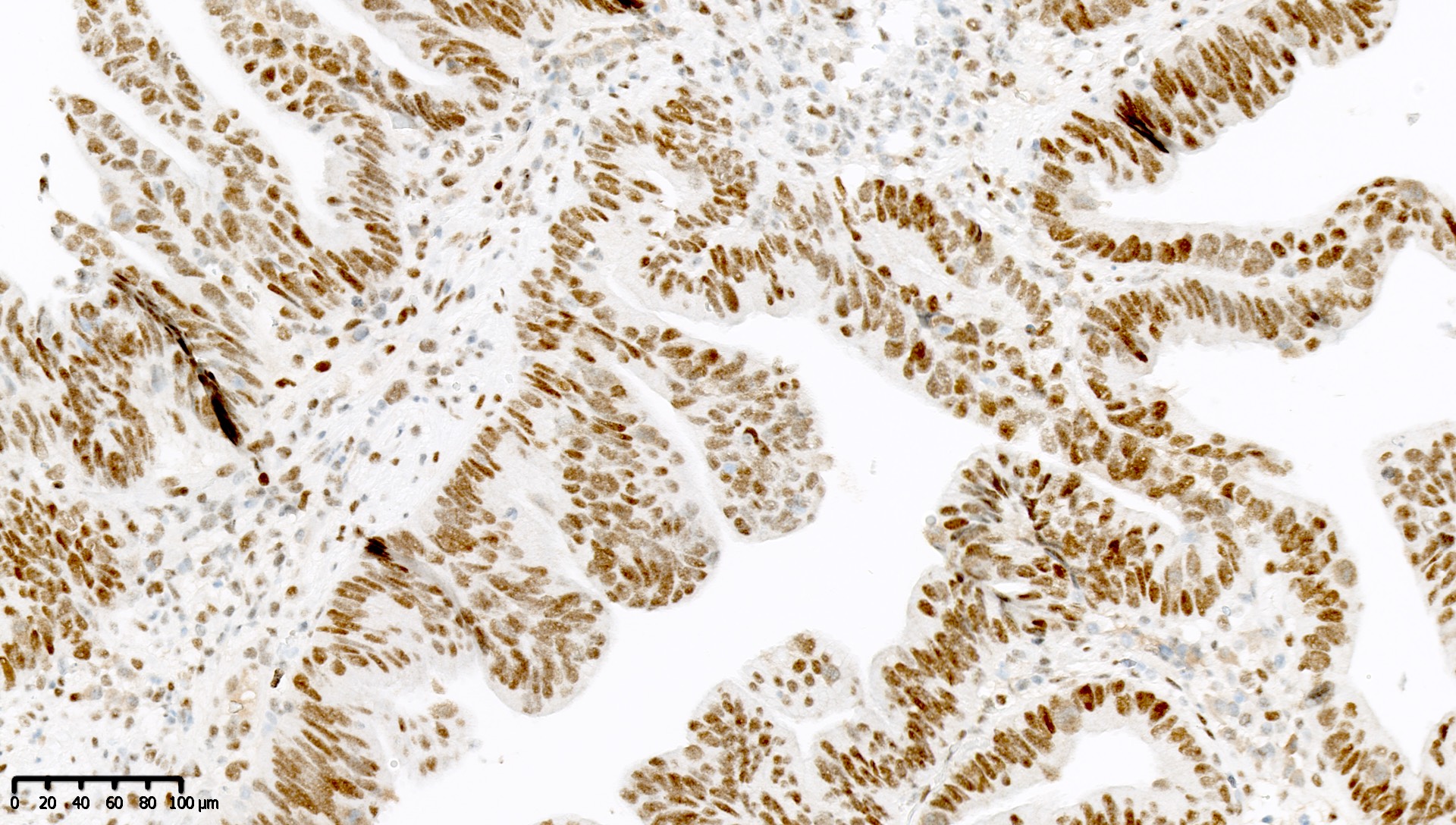
PMS2 proficient colon carcinoma
PMS2 proficient endometrial carcinosarcoma
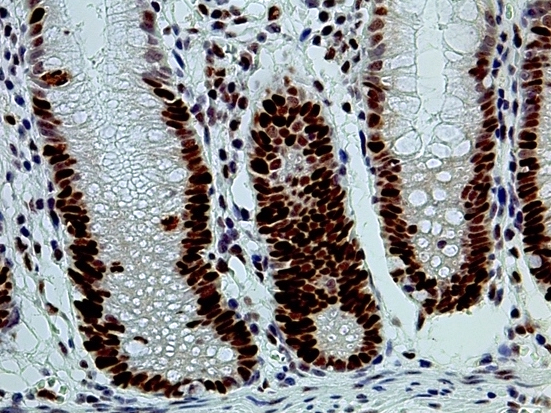
Colon, normal histology epithelium
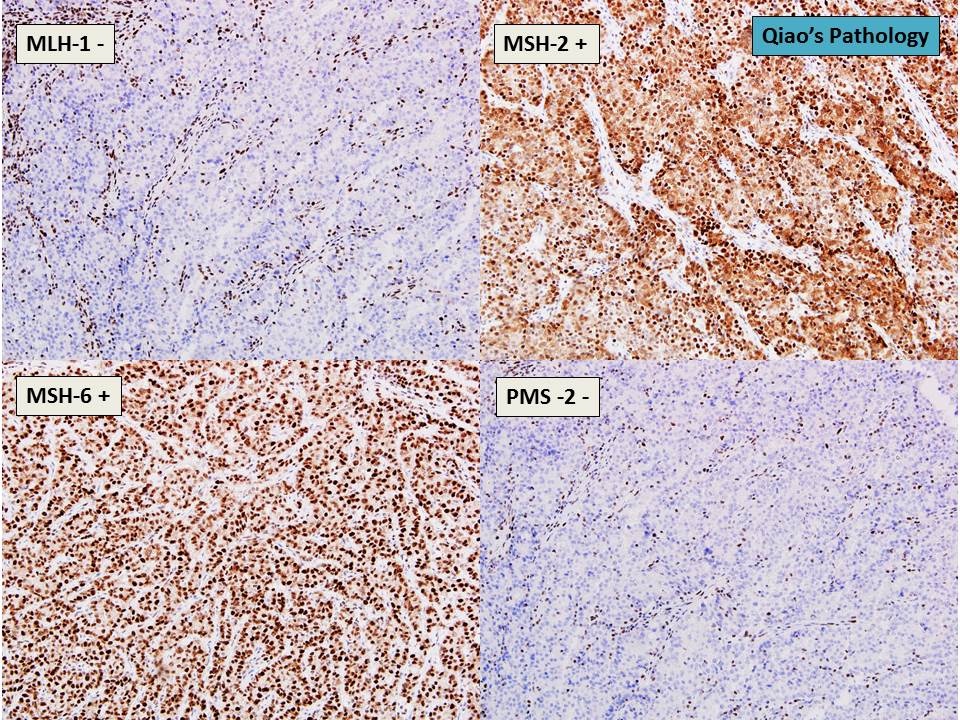
Colon cancer with loss of MLH1 and PMS2
Images hosted on other servers:

Sequential sections of the same colon crypt

Sequential sections of
a segment of colon
epithelium near a
colorectal cancer
Molecular / cytogenetics description
- National Cancer Institute recommendations: 5 microsatellite markers (BAT25, BAT26, N2S123, N5S346 and D17S250) for sequencing (Cancer Res 1998;58:5248) (additional markers may be used, however, there is no consensus on which markers to use)
- Sanger sequencing for germline mutations
- Multiplex ligation dependent probe amplification for large copy number variant detection
- Next generation sequencing

