
18 February 2010 - Case #170
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. David Cohen, Herzliyah Medical Center, Israel.
Case #170
Clinical history:
A 36 year old man presented with a right adrenal mass.
The specimen consisted of a tissue mass of 108 grams, measuring 10 x 6 x 5 cm, where the periphery was surrounded by a rim of fatty tissue.
On section, a peripheral, compressed slither of adrenal cortical tissue was still present but the medulla was replaced by a hemorrhagic and golden yellow soft mass.
Gross images:



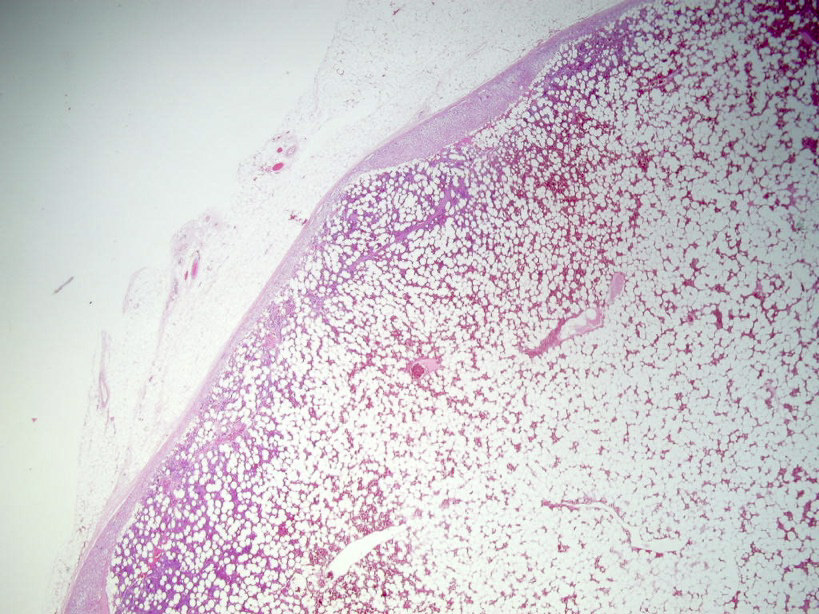
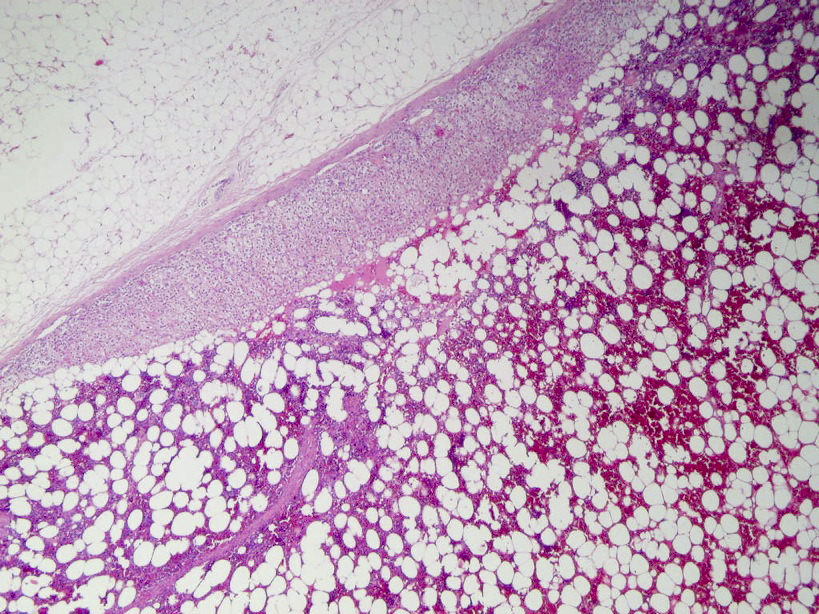
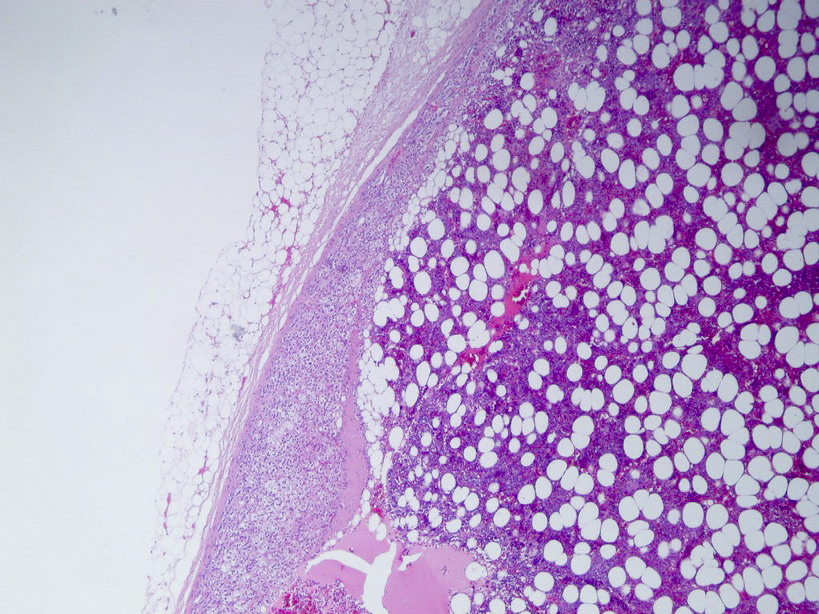
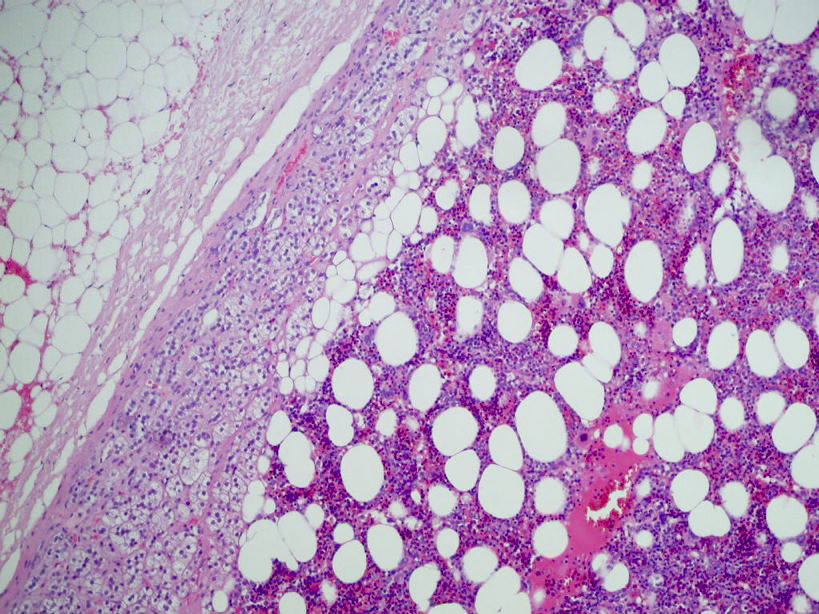
Microscopic images:
What is your diagnosis?
Diagnosis: Adrenal gland myelolipoma
Discussion:
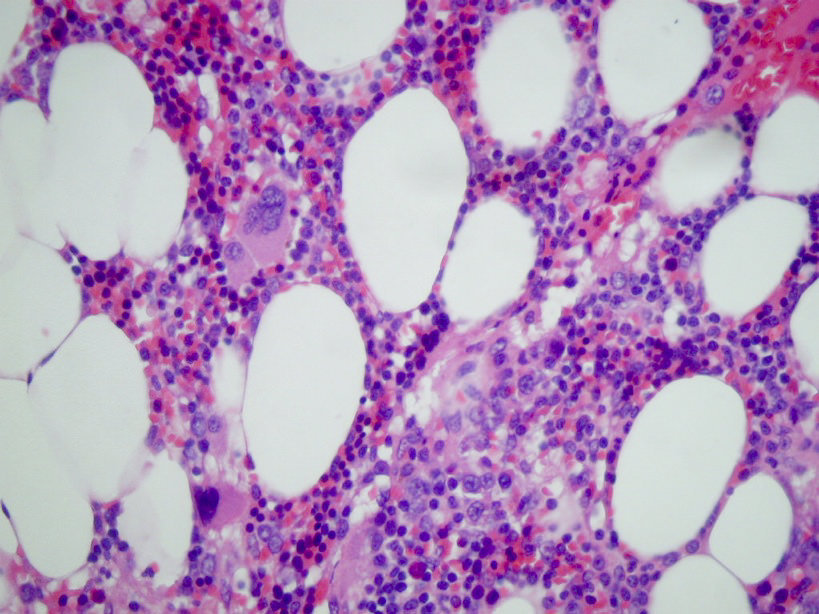
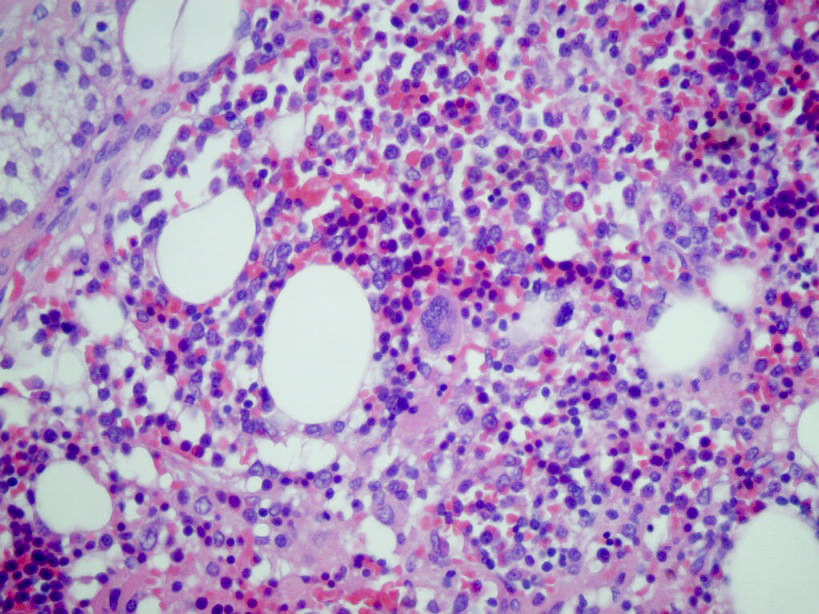
Sections showed a thin but essentially normal adrenal cortex at the periphery. The medulla was replaced by a benign proliferation of mature adipocytes interspersed with vascular channels and fresh hemorrhage, most likely due to surgery. The diagnostic finding was the presence of elements from all 3 hematopoietic cell lines.
Myelolipomas are benign, usually asymptomatic and often incidental lesions typically found in the adrenal region. Grossly, they vary from yellow to red to brown. Microscopic sections show normal adrenal tissue combined with myeloid, erythroid and megakaryocytic forming cell lines (Mod Pathol 2007;20:405). However, they differ from normal bone marrow due to increased frequency of megakaryocytes, reduced frequency of early myeloid precursors, and different vascular and stromal patterns (Am J Surg Pathol 2006;30:838). These tumors may be neoplastic, as 80% have nonrandom X chromosome inactivation.
Excision may be necessary if the lesion is painful or presents other symptoms. Large myelolipomas may cause local tissue necrosis, high blood pressure or hematuria. There have been no reports of malignant transformation.
The differential diagnosis includes adrenal adenoma (no hematopoietic elements) and angiomyolipoma (prominent myoid and vascular component, no hematopoietic elements). In addition, myelolipomas can coexist with other adrenal tumors (Arch Pathol Lab Med 2002;126:736).
References: Cases J 2009;2:9313, Cases J 2009;2:8414, eMedicine: Adrenal Myelolipoma (Incidentaloma) Imaging [Accessed 23 April 2024], J Pak Med Assoc 2009;59:491
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. David Cohen, Herzliyah Medical Center, Israel.
Website news:
(1) We posted a new article on our Management Page, Another Pay Cut for Pathology Practices and Laboratories, by Mick Raich, Vachette Pathology.
(2) We have updated the Acquired non-neoplastic anomalies section of the Bladder chapter.
(3) We have updated the Staging sections for all chapters with information from AJCC Cancer Staging Manual (7th ed)
(4) Thanks to the following contributors of images: Angel Fernandez-Flores, MD, PhD, Hospital El Bierzo & Clinica Ponferrada, Ponferrada, Spain; Andrea L. Wiens, D.O. and Janet E. Roepke, M.D., Ph.D, Ball Memorial Hospital, Muncie, Indiana (USA); Dr. Nadeem Zafar, Memphis, Tennessee (USA) - oxyphil adenoma for the Parathyroid gland chapter.
Visit and follow our Blog to see recent updates to the website.
(1) We posted a new article on our Management Page, Another Pay Cut for Pathology Practices and Laboratories, by Mick Raich, Vachette Pathology.
(2) We have updated the Acquired non-neoplastic anomalies section of the Bladder chapter.
(3) We have updated the Staging sections for all chapters with information from AJCC Cancer Staging Manual (7th ed)
(4) Thanks to the following contributors of images: Angel Fernandez-Flores, MD, PhD, Hospital El Bierzo & Clinica Ponferrada, Ponferrada, Spain; Andrea L. Wiens, D.O. and Janet E. Roepke, M.D., Ph.D, Ball Memorial Hospital, Muncie, Indiana (USA); Dr. Nadeem Zafar, Memphis, Tennessee (USA) - oxyphil adenoma for the Parathyroid gland chapter.
Visit and follow our Blog to see recent updates to the website.
Case #170
Clinical history:
A 36 year old man presented with a right adrenal mass.
The specimen consisted of a tissue mass of 108 grams, measuring 10 x 6 x 5 cm, where the periphery was surrounded by a rim of fatty tissue.
On section, a peripheral, compressed slither of adrenal cortical tissue was still present but the medulla was replaced by a hemorrhagic and golden yellow soft mass.
Gross images:
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Adrenal gland myelolipoma
Discussion:
Sections showed a thin but essentially normal adrenal cortex at the periphery. The medulla was replaced by a benign proliferation of mature adipocytes interspersed with vascular channels and fresh hemorrhage, most likely due to surgery. The diagnostic finding was the presence of elements from all 3 hematopoietic cell lines.
Myelolipomas are benign, usually asymptomatic and often incidental lesions typically found in the adrenal region. Grossly, they vary from yellow to red to brown. Microscopic sections show normal adrenal tissue combined with myeloid, erythroid and megakaryocytic forming cell lines (Mod Pathol 2007;20:405). However, they differ from normal bone marrow due to increased frequency of megakaryocytes, reduced frequency of early myeloid precursors, and different vascular and stromal patterns (Am J Surg Pathol 2006;30:838). These tumors may be neoplastic, as 80% have nonrandom X chromosome inactivation.
Excision may be necessary if the lesion is painful or presents other symptoms. Large myelolipomas may cause local tissue necrosis, high blood pressure or hematuria. There have been no reports of malignant transformation.
The differential diagnosis includes adrenal adenoma (no hematopoietic elements) and angiomyolipoma (prominent myoid and vascular component, no hematopoietic elements). In addition, myelolipomas can coexist with other adrenal tumors (Arch Pathol Lab Med 2002;126:736).
References: Cases J 2009;2:9313, Cases J 2009;2:8414, eMedicine: Adrenal Myelolipoma (Incidentaloma) Imaging [Accessed 23 April 2024], J Pak Med Assoc 2009;59:491
