19 June 2013 - Case #277
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Syed Sarwar Ali, The Aga Khan University Hospital (Pakistan), for contributing this case and the discussion.
Advertisement
Case #277
Clinical history:
A 45 year old man was admitted for high grade fever, rigors, chills and shortness of breath. He also had anuria and generalized weakness. His medical history included hypertension and diabetes. Physical examination showed a disoriented, pale and icteric man with 102 F temperature, tachycardia and 98% oxygen saturation at 5 liters.
The CBC showed (reference ranges in brackets): Hemoglobin 8.1g/dl (13.7 - 16.3 g/dl), hematocrit 23.2% (41.9 - 48.7%), WBC 4.6 x 10E9/L (4 - 10 x 10E9/L) and platelet count 16 x 10E9/L (150 - 400 x 10E9/L). His prothrombin time was 12.1 seconds (9 - 14 seconds) and APTT was elevated at 52.7 seconds (25 - 35 seconds). Liver function tests were: total bilirubin 10.9 mg/dl (0.1 - 1.1 mg/dl), direct bilirubin 7.2 mg/dl (0.0 - 0.2mg/dl), indirect bilirubin 3.7 mg/dl (0.1 - 0.8 mg/dl) and creatinine 1.9 mg/dl (0.9 - 1.3 mg/dl).
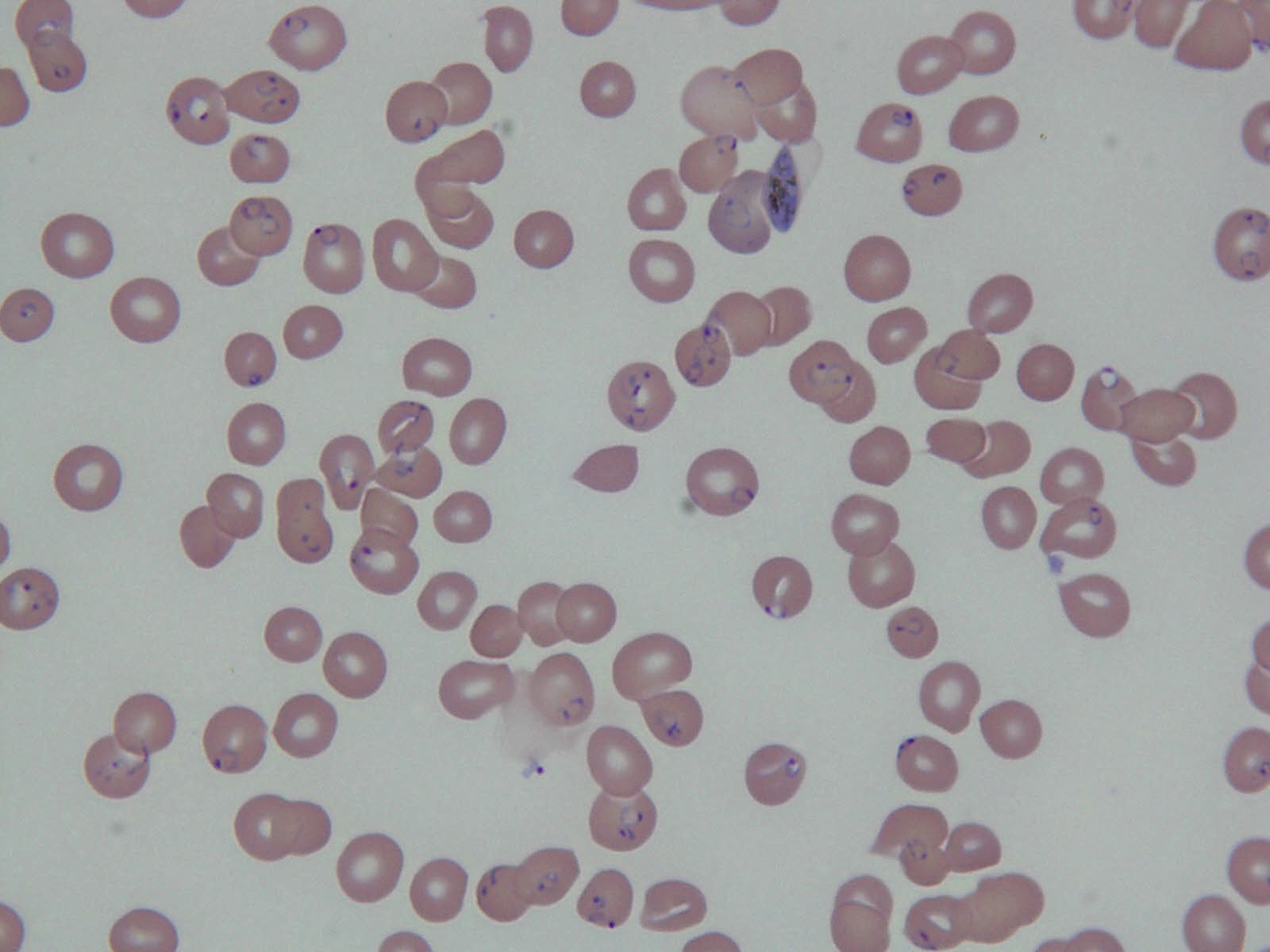
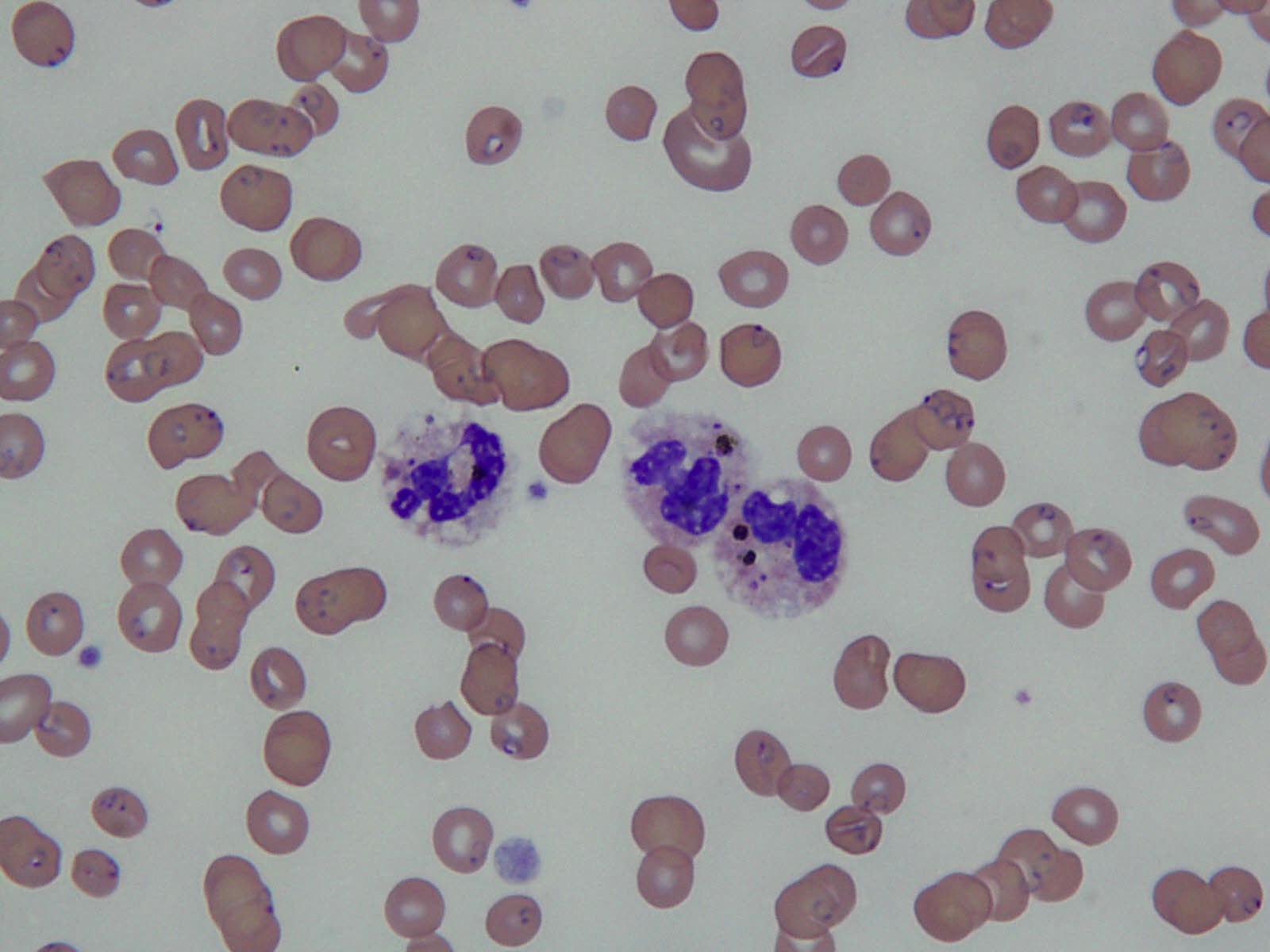
Blood smear images:
What is your diagnosis?
Diagnosis: Malaria (Plasmodium falciparum)
Discussion:
The blood smear review displayed heavy infestation with Plasmodium falciparum with 60% parasitemia. Erythrocytes with double parasites were also observed. 10% of neutrophils had visible malarial pigments or hemozoin. A diagnosis of severe falciparum malaria with multiorgan failure was made. Shortly after admission, he developed cardiac arrest. He revived initially with CPR and full supportive measures but later died.
Malaria is the single most important disease hazard from travel to developing countries. Worldwide, there are over 200 million annual cases with over 600,000 annual deaths (Wikipedia: Malaria [Accessed 29 March 2024], CDC: Malaria [Accessed 29 March 2024]). Hematological indicators of poor prognosis in severe malaria include a platelet count < 50 x 10E9/L, prolonged PT > 3 seconds, prolonged APTT, fibrinogen < 200mg/dl, hyperparasitemia > 100,00/uL (high mortality if > 500,000/uL), > 20% parasites and > 5% neutrophils containing visible malarial pigment. Early recognition and prompt management are important.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Syed Sarwar Ali, The Aga Khan University Hospital (Pakistan), for contributing this case and the discussion.
November 2, 2013
The Henry, Autograph Collection
Dearborn, Michigan (USA)
10th Annual Course
Contemporary Issues
In Diagnostic Pathology

Website
Hotel
Website news:
(1) We have finished updating the Thyroid chapter with images contributed by Dr. Mark R. Wick.
(2) We have updated the Skin-melanocytic tumor chapter based on reviews by Christopher Hale, M.D.
(3) Next month, we will begin sending out our new Oncology newsletter quarterly with information on new pathology related drugs and other tumor related information for both oncologists and pathologists. Click here to sign up to receive this free newsletter.
Visit and follow our Blog to see recent updates to the website.
(1) We have finished updating the Thyroid chapter with images contributed by Dr. Mark R. Wick.
(2) We have updated the Skin-melanocytic tumor chapter based on reviews by Christopher Hale, M.D.
(3) Next month, we will begin sending out our new Oncology newsletter quarterly with information on new pathology related drugs and other tumor related information for both oncologists and pathologists. Click here to sign up to receive this free newsletter.
Visit and follow our Blog to see recent updates to the website.
Case #277
Clinical history:
A 45 year old man was admitted for high grade fever, rigors, chills and shortness of breath. He also had anuria and generalized weakness. His medical history included hypertension and diabetes. Physical examination showed a disoriented, pale and icteric man with 102 F temperature, tachycardia and 98% oxygen saturation at 5 liters.
The CBC showed (reference ranges in brackets): Hemoglobin 8.1g/dl (13.7 - 16.3 g/dl), hematocrit 23.2% (41.9 - 48.7%), WBC 4.6 x 10E9/L (4 - 10 x 10E9/L) and platelet count 16 x 10E9/L (150 - 400 x 10E9/L). His prothrombin time was 12.1 seconds (9 - 14 seconds) and APTT was elevated at 52.7 seconds (25 - 35 seconds). Liver function tests were: total bilirubin 10.9 mg/dl (0.1 - 1.1 mg/dl), direct bilirubin 7.2 mg/dl (0.0 - 0.2mg/dl), indirect bilirubin 3.7 mg/dl (0.1 - 0.8 mg/dl) and creatinine 1.9 mg/dl (0.9 - 1.3 mg/dl).
Blood smear images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Malaria (Plasmodium falciparum)
Discussion:
The blood smear review displayed heavy infestation with Plasmodium falciparum with 60% parasitemia. Erythrocytes with double parasites were also observed. 10% of neutrophils had visible malarial pigments or hemozoin. A diagnosis of severe falciparum malaria with multiorgan failure was made. Shortly after admission, he developed cardiac arrest. He revived initially with CPR and full supportive measures but later died.
Malaria is the single most important disease hazard from travel to developing countries. Worldwide, there are over 200 million annual cases with over 600,000 annual deaths (Wikipedia: Malaria [Accessed 29 March 2024], CDC: Malaria [Accessed 29 March 2024]). Hematological indicators of poor prognosis in severe malaria include a platelet count < 50 x 10E9/L, prolonged PT > 3 seconds, prolonged APTT, fibrinogen < 200mg/dl, hyperparasitemia > 100,00/uL (high mortality if > 500,000/uL), > 20% parasites and > 5% neutrophils containing visible malarial pigment. Early recognition and prompt management are important.