
16 August 2023 - Case of the Month #530
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Drs. Kristen Muller and Samantha Stephen, Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire, USA for contributing this case and discussion and to Dr. Julie Jorns, Medical College of Wisconsin, Milwaukee, Wisconsin, USA for reviewing the discussion.

Case of the Month #530
Clinical history:
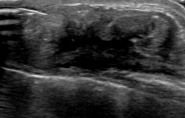
A 66 year old woman with a history of right sided invasive lobular carcinoma (ER+/PR-/ HER2-) 15 years ago and ipsilateral recurrence of the cancer 10 years later, was status post bilateral mastectomy with breast implant reconstruction. She developed rib pain and CT of the chest showed an asymmetric 4.8 cm soft tissue mass overlying the anterior fourth rib. Ultrasound revealed a hypoechoic ill defined mass with high vascularity. A biopsy was performed.
Radiology and histopathology images:


What is your diagnosis?
Diagnosis: Acellular dermal matrix
Test question (answer at the end):
Which of the following statements is true about acellular dermal matrix?
A. Comprised of avascular and acellular collagen fibers after implantation
B. Never clinically palpable
C. Not commonly used in breast reconstructive surgery
D. Shows hypercellular stroma with intermixed breast ducts and lobules
Discussion:
Acellular or regenerative dermal matrices (ADMs) such as Alloderm® (LifeCell Corp.; Branchburg, NJ, USA) are composed of decellularized cadaveric human or xenogenic tissue and are often used as a scaffold in breast reconstruction to provide bulk and support around implant capsules. ADMs are considered immunologically inert as they are acellular and sterilized to allow for revascularization and incorporation into the host tissue. These products are becoming an integral part of implant based breast reconstructive surgery as they provide a number of benefits for patients including improved contour of the inframammary fold and lateral breast margin, minimal host immune response and scar formation, as well as improved aesthetic shape and elasticity (J Plast Reconstr Aesthet Surg 2011;64:1553, Clin Breast Cancer 2017;17:266).
Palpable or abnormal imaging findings may present in patients with a history of breast reconstruction and the differential diagnosis in such cases usually includes recurrence, fat necrosis and scar. ADM tissue should be included in this differential as well, as some patients report developing a new palpable area of concern and it is important for pathologists to recognize the histologic features. The literature on imaging and pathology findings of ADMs is sparse. On ultrasound imaging, ADMs may display features of a hypoechoic mass or nodularity with indistinct margins. There is reported variability in the imaging features of ADMs, with some cases showing areas of thickening and decreased echogenicity, focal echogenic spots or even diffusely increased echogenicity. The variable imaging features may correspond to different points of transformation from acellular matrix to mature collagenous tissue (J Clin Med 2022;11:1057, J Clin Imaging Sci 2017;7:13).
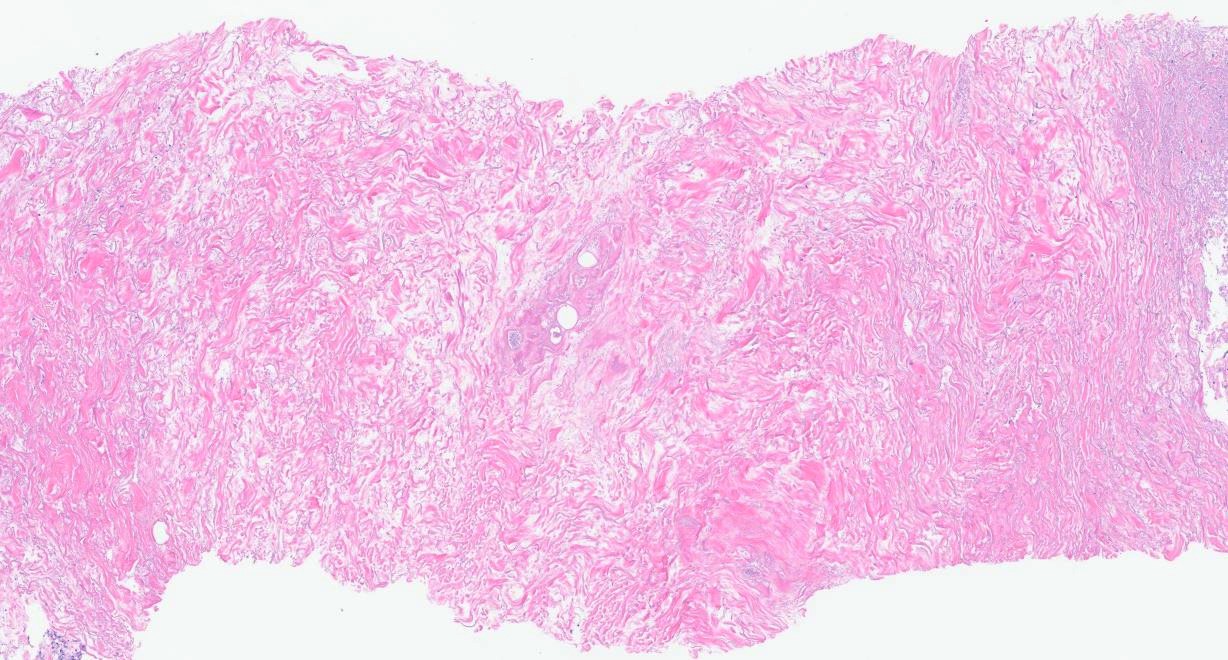
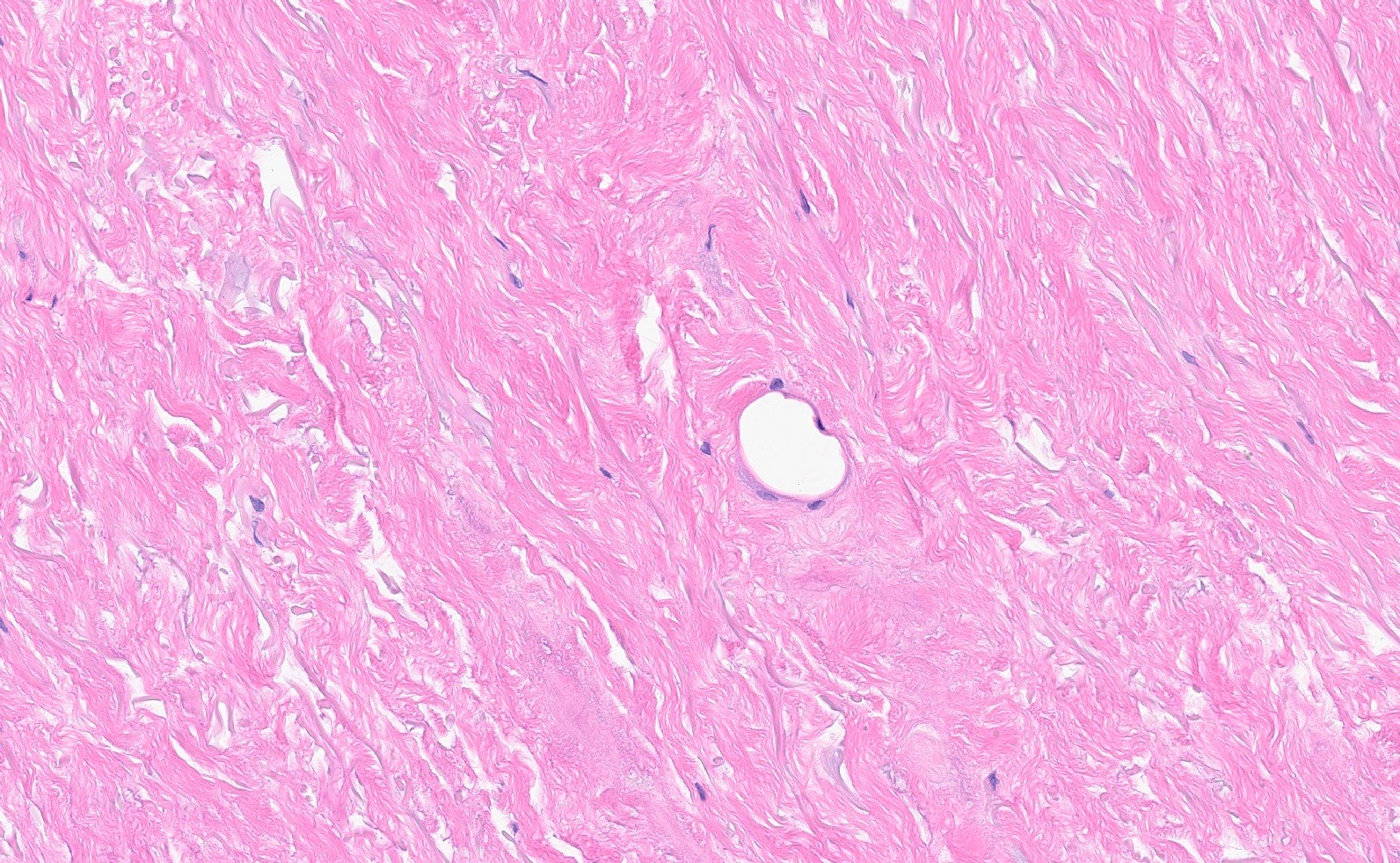
The histologic features of ADM vary based on the stage of tissue remodeling. After implantation, the tissue is comprised of acellular and avascular disorganized collagen fibers. Eventually, the acellular matrix undergoes neovascularization with the production of small capillaries and proliferation of fibroblasts around the collagen fibers. Once ADM undergoes tissue remodeling and incorporation, the tissue can resemble mature dense fibrous tissue, although it has a higher density of collagen fibers and a comparatively lower density of fibroblasts. Patchy chronic inflammation and degenerative changes can be seen, as well as multinucleated foreign body giant cells. The histologic differential diagnosis usually includes scar and fat necrosis. Differentiating ADM from fat necrosis can be further complicated by the presence of focal fat necrosis that has been reported within ADM (J Clin Med 2022;11:1057).
Test question answer:
A. Acellular dermal matrix is comprised of avascular and acellular collagen fibers after implantation. The histologic features of acellular matrix vary based on the stage of tissue remodeling. After implantation, the tissue is comprised of acellular and avascular disorganized collagen fibers. Eventually, the acellular matrix undergoes neovascularization with the production of small capillaries and proliferation of fibroblasts around the collagen fibers. Once acellular dermal matrix undergoes tissue remodeling and incorporation, the tissue may resemble mature dense fibrous tissue.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Drs. Kristen Muller and Samantha Stephen, Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire, USA for contributing this case and discussion and to Dr. Julie Jorns, Medical College of Wisconsin, Milwaukee, Wisconsin, USA for reviewing the discussion.
Case of the Month #530
Clinical history:
A 66 year old woman with a history of right sided invasive lobular carcinoma (ER+/PR-/ HER2-) 15 years ago and ipsilateral recurrence of the cancer 10 years later, was status post bilateral mastectomy with breast implant reconstruction. She developed rib pain and CT of the chest showed an asymmetric 4.8 cm soft tissue mass overlying the anterior fourth rib. Ultrasound revealed a hypoechoic ill defined mass with high vascularity. A biopsy was performed.
Radiology and histopathology images:
What is your diagnosis?
Click here for diagnosis, test question and discussion:
Diagnosis: Acellular dermal matrix
Test question (answer at the end):
Which of the following statements is true about acellular dermal matrix?
A. Comprised of avascular and acellular collagen fibers after implantation
B. Never clinically palpable
C. Not commonly used in breast reconstructive surgery
D. Shows hypercellular stroma with intermixed breast ducts and lobules
Discussion:
Acellular or regenerative dermal matrices (ADMs) such as Alloderm® (LifeCell Corp.; Branchburg, NJ, USA) are composed of decellularized cadaveric human or xenogenic tissue and are often used as a scaffold in breast reconstruction to provide bulk and support around implant capsules. ADMs are considered immunologically inert as they are acellular and sterilized to allow for revascularization and incorporation into the host tissue. These products are becoming an integral part of implant based breast reconstructive surgery as they provide a number of benefits for patients including improved contour of the inframammary fold and lateral breast margin, minimal host immune response and scar formation, as well as improved aesthetic shape and elasticity (J Plast Reconstr Aesthet Surg 2011;64:1553, Clin Breast Cancer 2017;17:266).
Palpable or abnormal imaging findings may present in patients with a history of breast reconstruction and the differential diagnosis in such cases usually includes recurrence, fat necrosis and scar. ADM tissue should be included in this differential as well, as some patients report developing a new palpable area of concern and it is important for pathologists to recognize the histologic features. The literature on imaging and pathology findings of ADMs is sparse. On ultrasound imaging, ADMs may display features of a hypoechoic mass or nodularity with indistinct margins. There is reported variability in the imaging features of ADMs, with some cases showing areas of thickening and decreased echogenicity, focal echogenic spots or even diffusely increased echogenicity. The variable imaging features may correspond to different points of transformation from acellular matrix to mature collagenous tissue (J Clin Med 2022;11:1057, J Clin Imaging Sci 2017;7:13).
The histologic features of ADM vary based on the stage of tissue remodeling. After implantation, the tissue is comprised of acellular and avascular disorganized collagen fibers. Eventually, the acellular matrix undergoes neovascularization with the production of small capillaries and proliferation of fibroblasts around the collagen fibers. Once ADM undergoes tissue remodeling and incorporation, the tissue can resemble mature dense fibrous tissue, although it has a higher density of collagen fibers and a comparatively lower density of fibroblasts. Patchy chronic inflammation and degenerative changes can be seen, as well as multinucleated foreign body giant cells. The histologic differential diagnosis usually includes scar and fat necrosis. Differentiating ADM from fat necrosis can be further complicated by the presence of focal fat necrosis that has been reported within ADM (J Clin Med 2022;11:1057).
Test question answer:
A. Acellular dermal matrix is comprised of avascular and acellular collagen fibers after implantation. The histologic features of acellular matrix vary based on the stage of tissue remodeling. After implantation, the tissue is comprised of acellular and avascular disorganized collagen fibers. Eventually, the acellular matrix undergoes neovascularization with the production of small capillaries and proliferation of fibroblasts around the collagen fibers. Once acellular dermal matrix undergoes tissue remodeling and incorporation, the tissue may resemble mature dense fibrous tissue.
