

Adrenal gland & paraganglia
Other tumors
Myelolipoma
Editorial Board Member: Debra L. Zynger, M.D.
Deputy Editor-in-Chief: Maria Tretiakova, M.D., Ph.D.


Last author update: 27 October 2022
Last staff update: 1 December 2023
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Adrenal myelolipoma
Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Diagnosis | Laboratory | Radiology description | Radiology images | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Cevik L, Parwani A. Myelolipoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/adrenalmyelolipoma.html. Accessed May 14th, 2024.
Definition / general
- Rare, although it is the second most common benign tumor in adrenal glands after adrenal cortical adenomas (Lancet Diabetes Endocrinol 2020;8:894)
- Benign and usually unilateral (95%) tumor composed of trilineage hematopoietic cells and mature fat
- Usually an incidental finding on imaging (CT / MRI) or on autopsy
- Not associated with hematologic disorders
Essential features
- Ages range usually between 50 - 70 years, with no gender predilection
- Benign and usually unilateral (95%) tumor composed of trilineage hematopoietic cells and mature fat
- Usually an incidental finding on imaging (CT / MRI) or on autopsy
- Not associated with hematologic disorders
- Can be associated with congenital adrenal hyperplasia (10%), Cushing syndrome and rarely, adrenal ganglioneuroma
Epidemiology
- No gender predilection
- ~3% of primary adrenal neoplasms
- Age range is usually between 50 - 70 years, rarely < 30 years
- Can be associated with:
- Congenital adrenal hyperplasia (10%) (Endocr Pract 2020;26:1351, Endocrine 2018;59:7)
- Cushing syndrome (Am J Med Sci 1997;314:338, Medicine (Baltimore) 2017;96:e9455)
- Rarely, adrenal ganglioneuroma (Int J Clin Exp Pathol 2019;12:2302, Arch Pathol Lab Med 2002;126:736)
Sites
- Adrenal gland is most common
- Extra-adrenal sites are rare but can include retroperitoneum, presacral region, mediastinum
Pathophysiology
- Unknown but several hypotheses exist (Lancet Diabetes Endocrinol 2021;9:767)
- Increased concentration of erythropoietin
- Interactions between 2 stem cell progenitors of fat cells and bone marrow cells
- Metaplastic changes of blood capillary reticuloendothelial cells due to inflammation, stress, trauma or via embolism of bone marrow cells
- Chromosomal translocation t(3;21)(q25;p11) or nonrandom X inactivation
- Hormonal factors (Cushing syndrome, congenital adrenal hyperplasia)
Diagnosis
- Adrenal myelolipomas can be diagnosed in 90% of cases by ultrasonography, CT and MRI
- Histological appearance is straightforward on H&E staining
Laboratory
- No specific laboratory findings
- Hormonally inactive; excess adrenal hormones can be detected if associated with Cushing syndrome or congenital adrenal hyperplasia
Radiology description
- Mostly unilateral and solitary; rarely bilateral (5%)
- Rounded tumor mainly comprised of macroscopic fat with a variable proportion of myeloid components
- Myeloid components can be seen as a cloudy pattern, solid strands or forming a separate solid nodule within the fat
- Reference: Lancet Diabetes Endocrinol 2021;9:767
Radiology images
Images hosted on other servers:

Abdominal US

CT abdomen findings

MRI findings

Giant bilateral myelolipomas of abdomen

CT axial section showing mass in right renal gland
Case reports
- 26 year old woman with large right adrenal myelolipoma (J Surg Case Rep 2022;2022:rjac213)
- 48 year old man with undiagnosed congenital adrenal hyperplasia and bilateral adrenal masses (Case Rep Endocrinol 2022;2022:4044602)
- 71 year old man with anterior mediastinal myelolipoma (Am J Case Rep 2022;23:e936005)
Treatment
- Follow up or excision if symptomatic (if > 8 cm, rarely acute hemorrhage and rupture can occur)
- No malignant progression or recurrence
Clinical images
Images hosted on other servers:

Large suprarenal mass
Gross description
- Well demarcated, unencapsulated, yellow (mature fat) to red (hemorrhage) nodule depending on the composition; if large, hemorrhage and infarction are common
- Mean size is 10 cm (0.5 - 43 cm); weight may be up to 11 kg
Gross images
Contributed by Debra L. Zynger, M.D. and Anil Parwani, M.D., Ph.D.
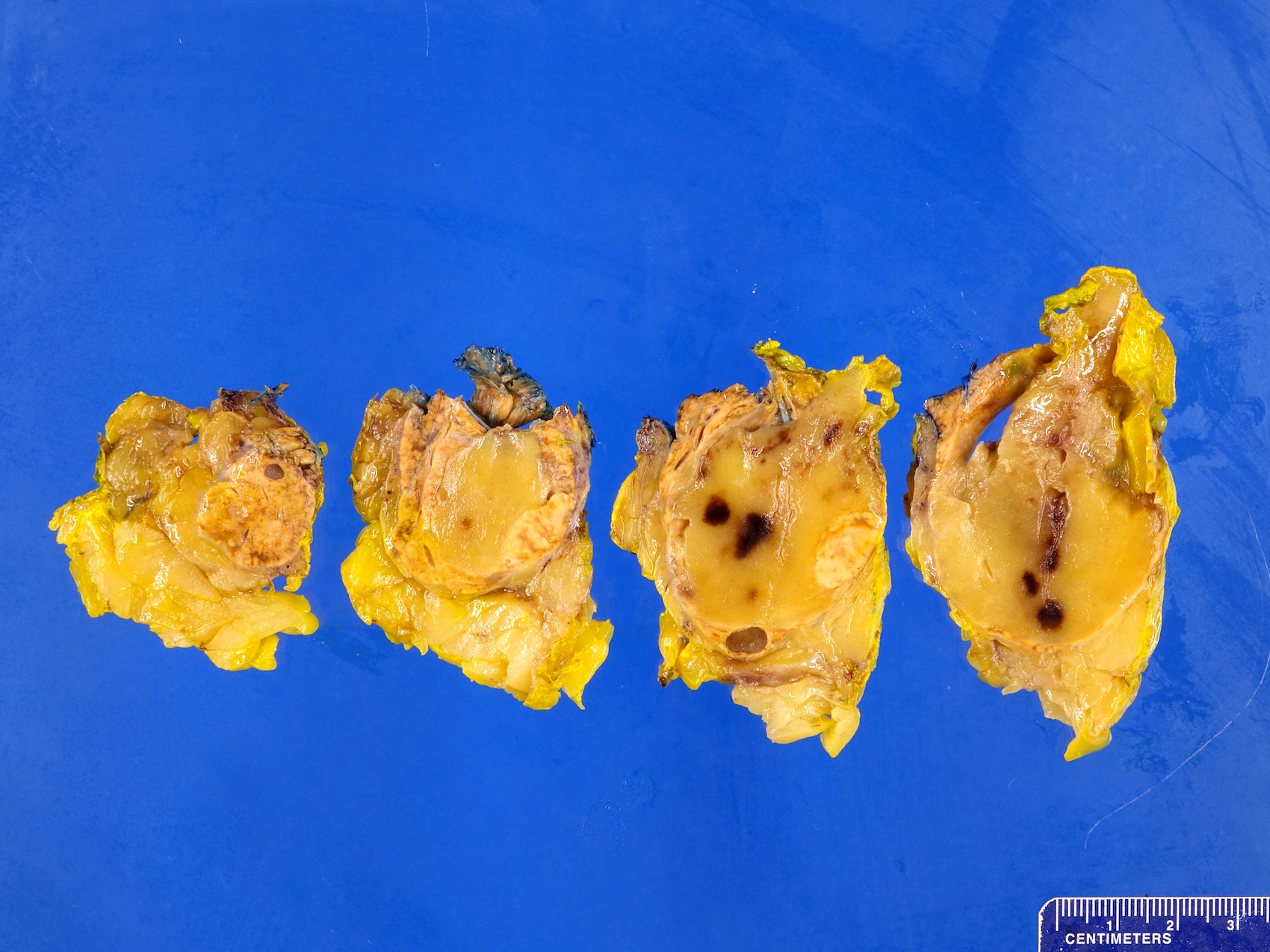
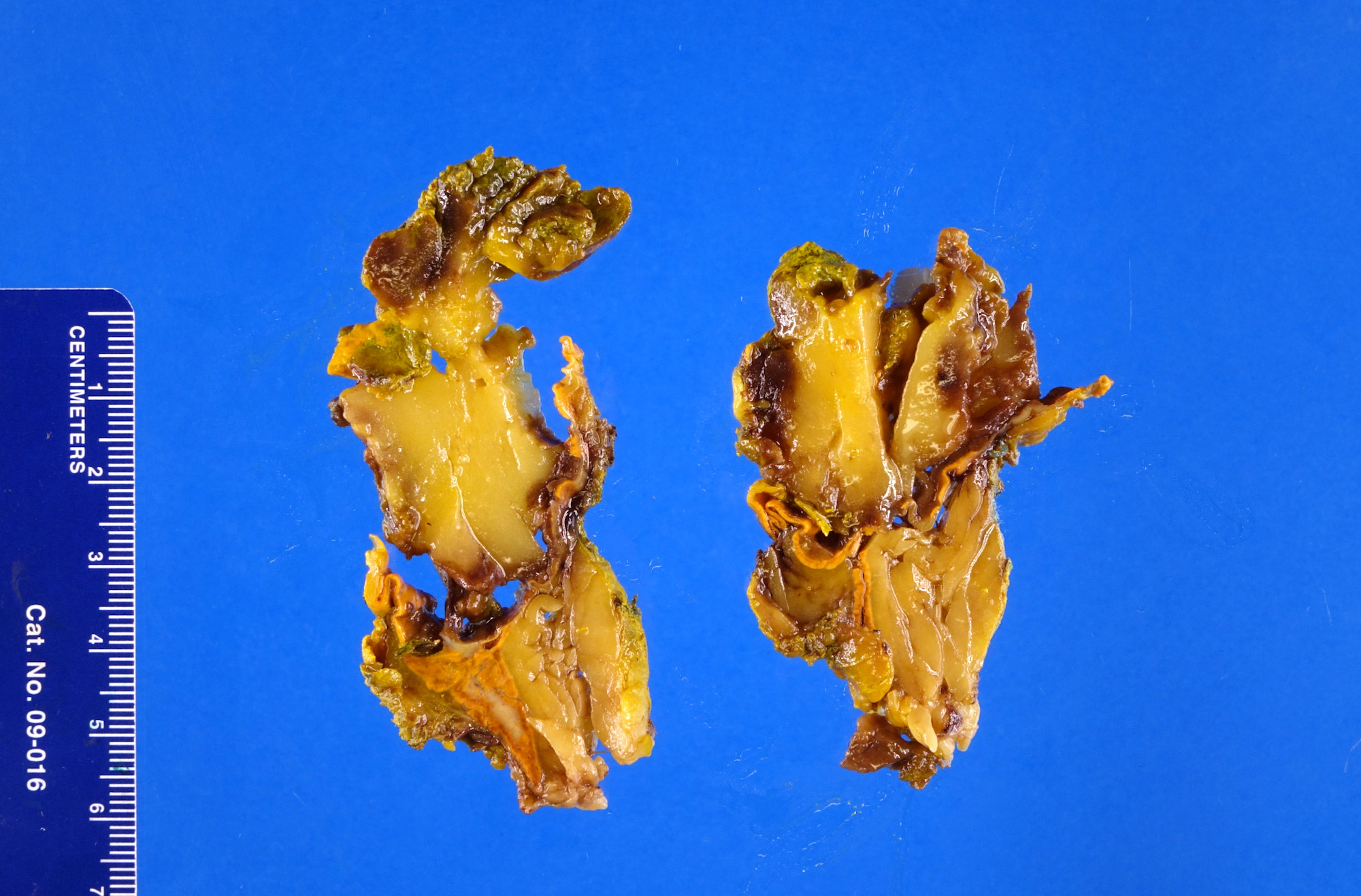
Fat predominant

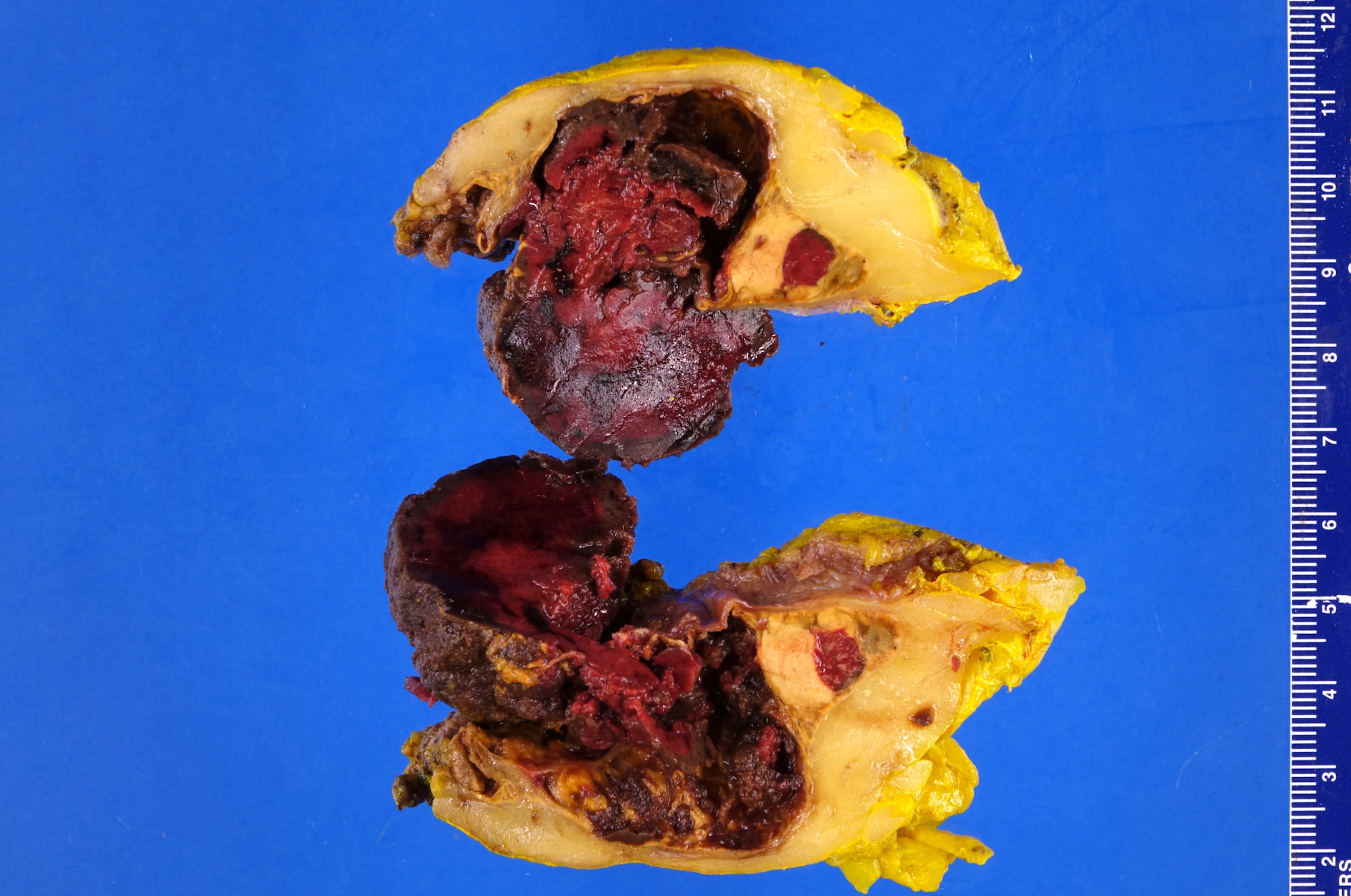
Extensive hemorrhage
Images hosted on other servers:


Intact adrenal specimen


Bright yellow and focally red, fatty tumor with extensive hemorrhage

Grey / brown / yellowish with hemorrhage

Well circumscribed
tumor with hemorrhage
Microscopic (histologic) description
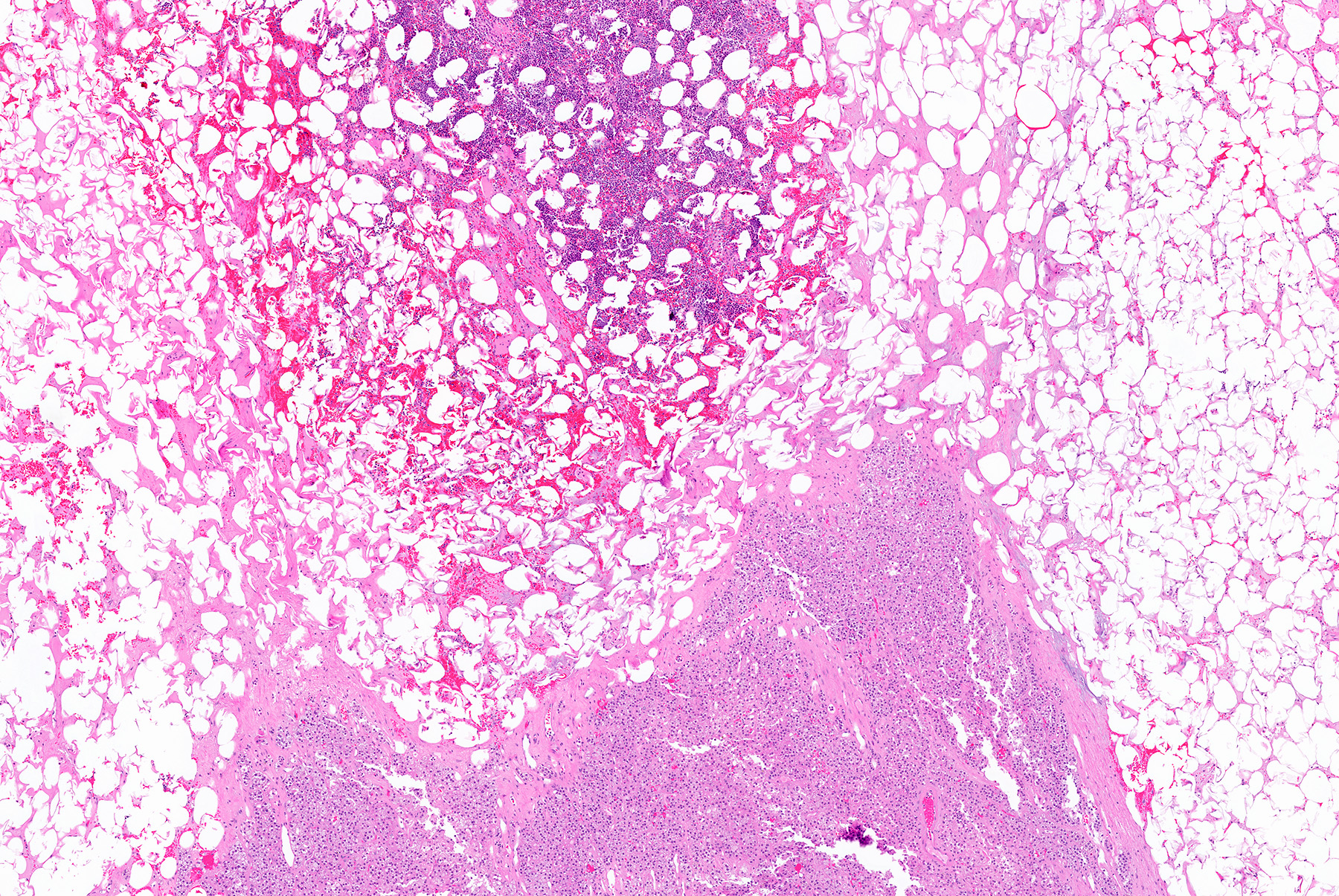
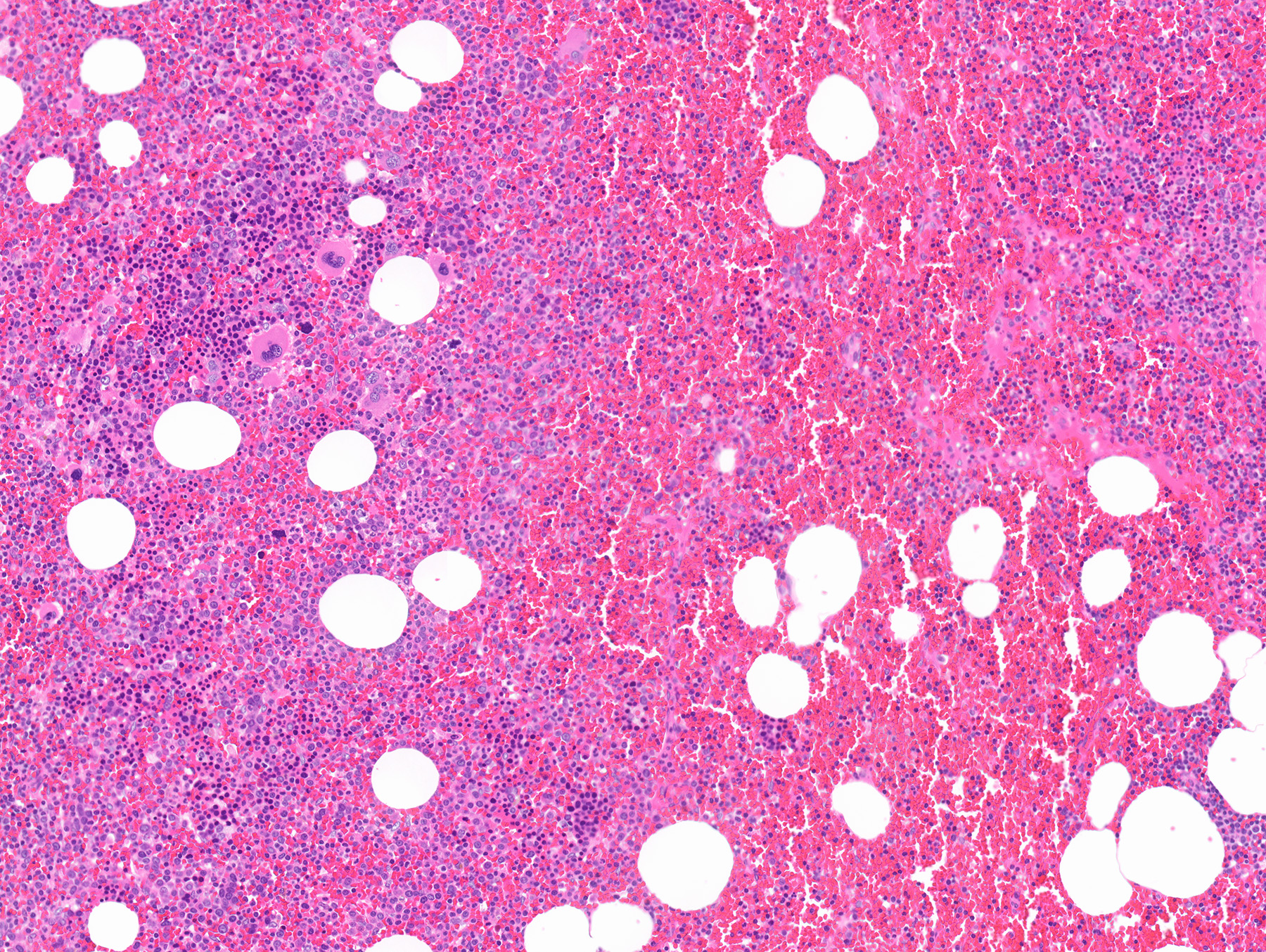
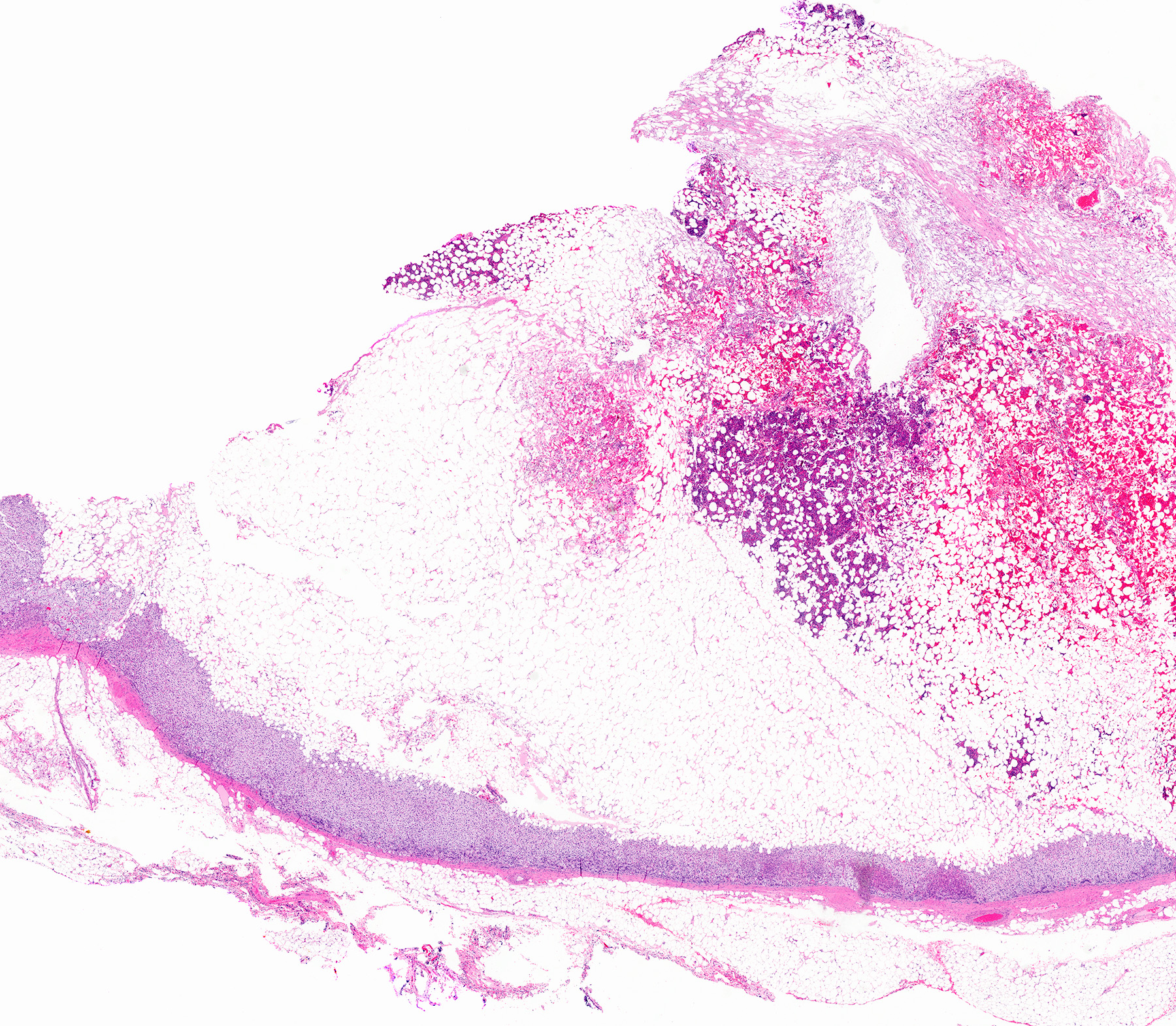
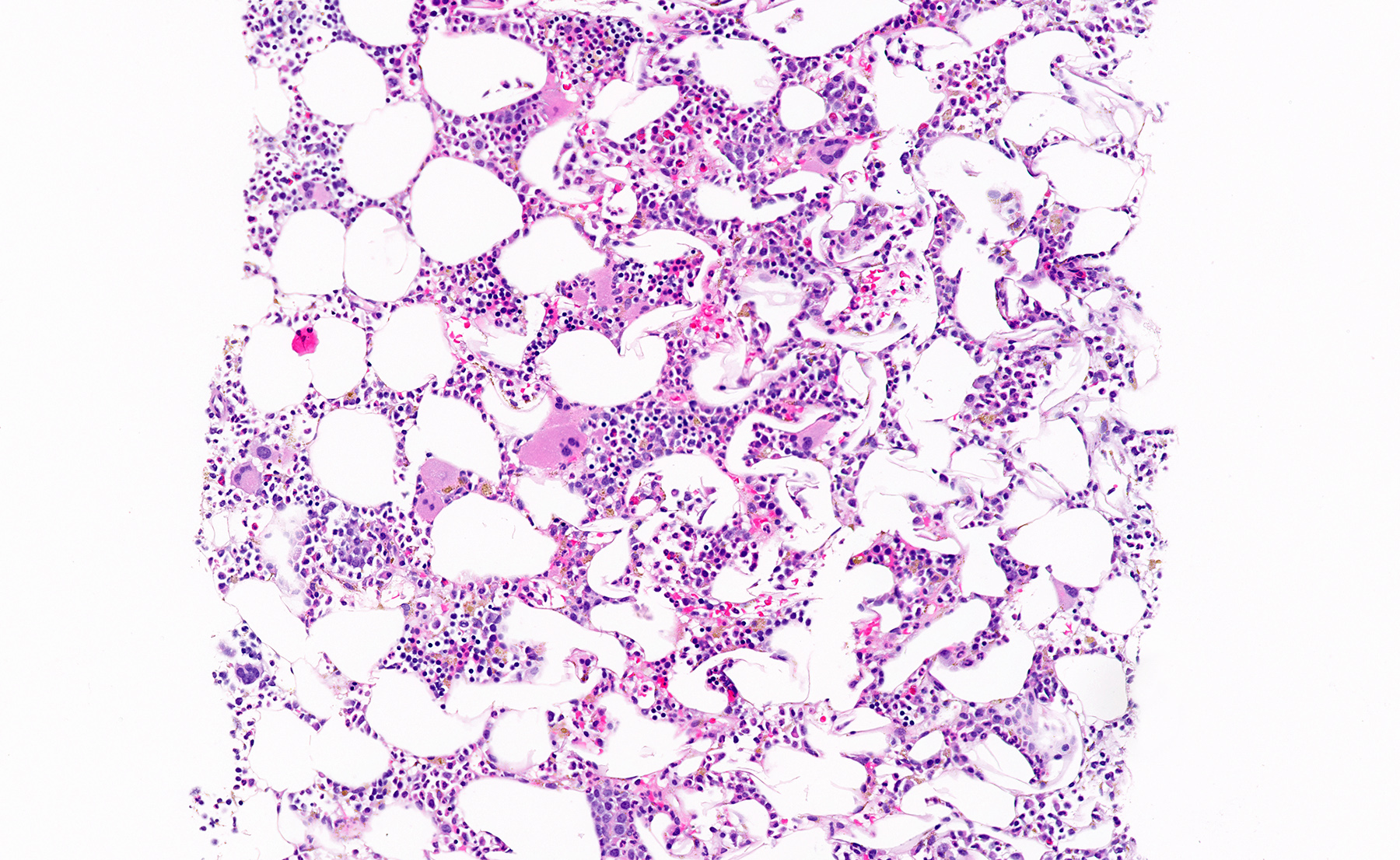
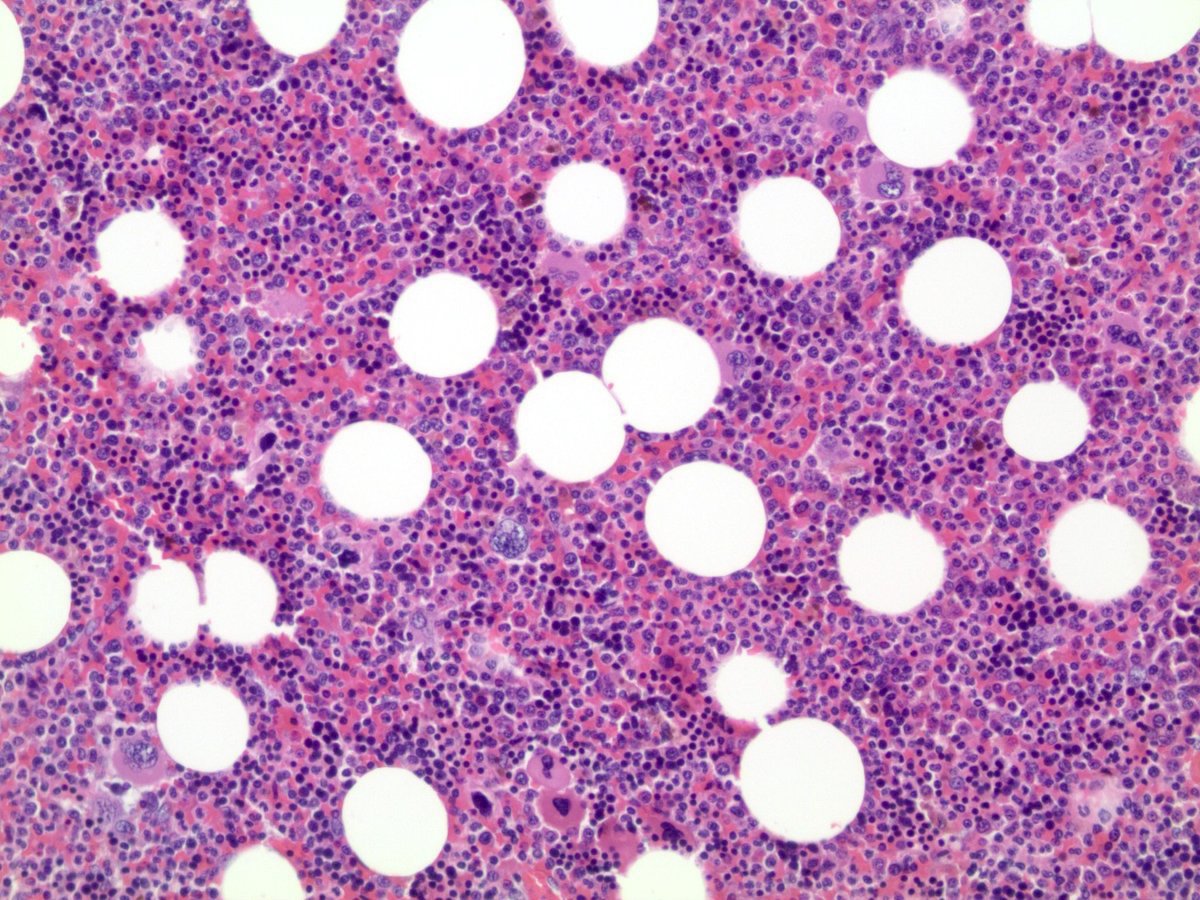
- Mixture of mature adipocytes and extramedullary trilineage hematopoietic cells with full maturation (similar to a hypercellular bone marrow) but often with a markedly increased number of megakaryocytes (Am J Surg Pathol 2006;30:838)
- Calcification, osseous metaplasia and fibrosis can occur
- Rarely may have areas of fibromyxoid degeneration resembling low grade fibromyxoid sarcoma
- Can develop in combination with adrenal cortical tumors, ganglioneuroma, hibernoma, bilateral macronodular adrenocortical disease and congenital adrenal hyperplasia
Microscopic (histologic) images
Contributed by Debra L. Zynger, M.D., Anil Parwani, M.D., Ph.D., O. Hans Iwenofu, M.D., Ph.D. and @ThatGlassTho on Twitter
Hematopoietic cells
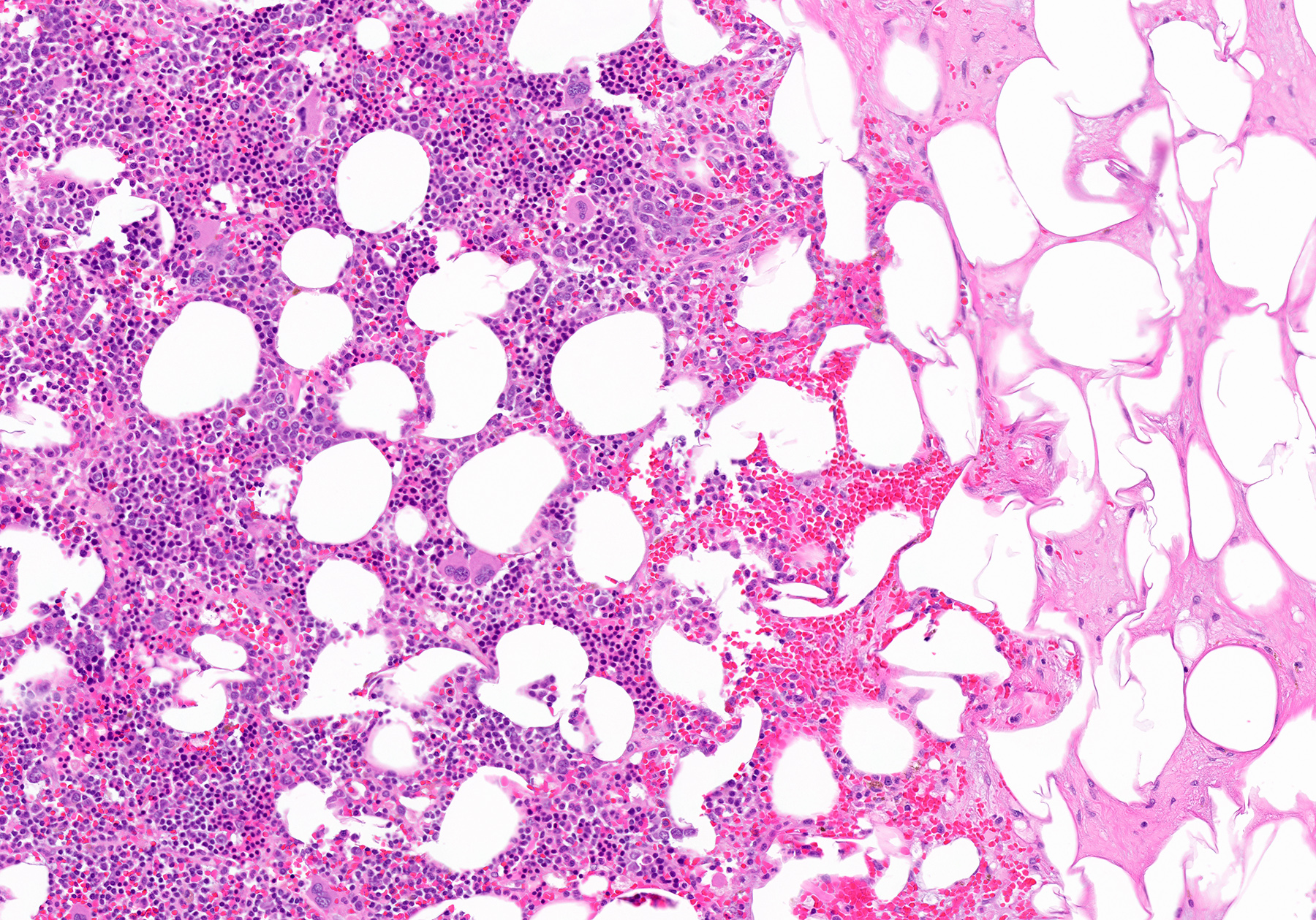
Increased megakaryocytes
Hematopoietic cells and mature fat
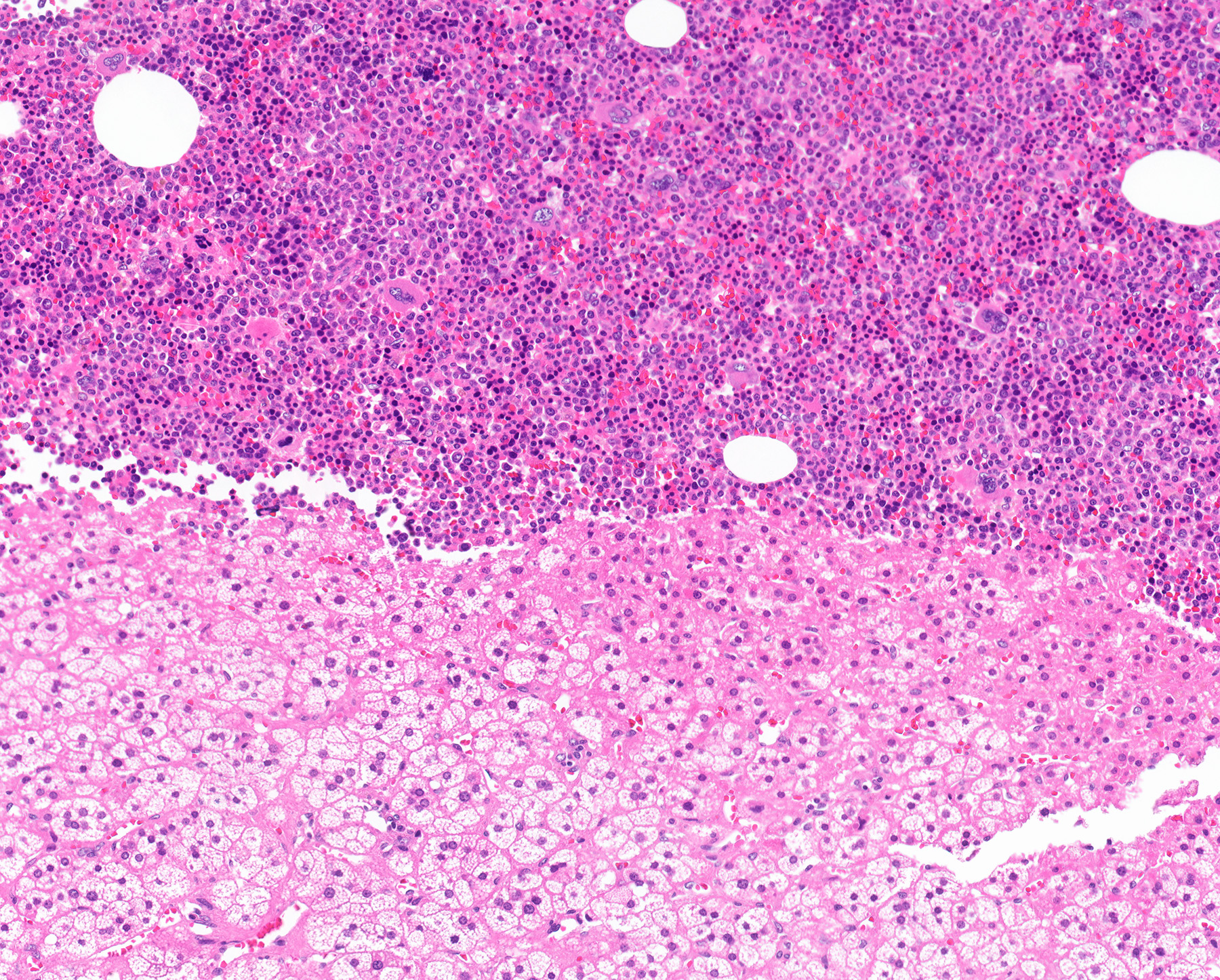
Hematopoietic cells and adrenal cortex

Myelolipoma in adrenal gland
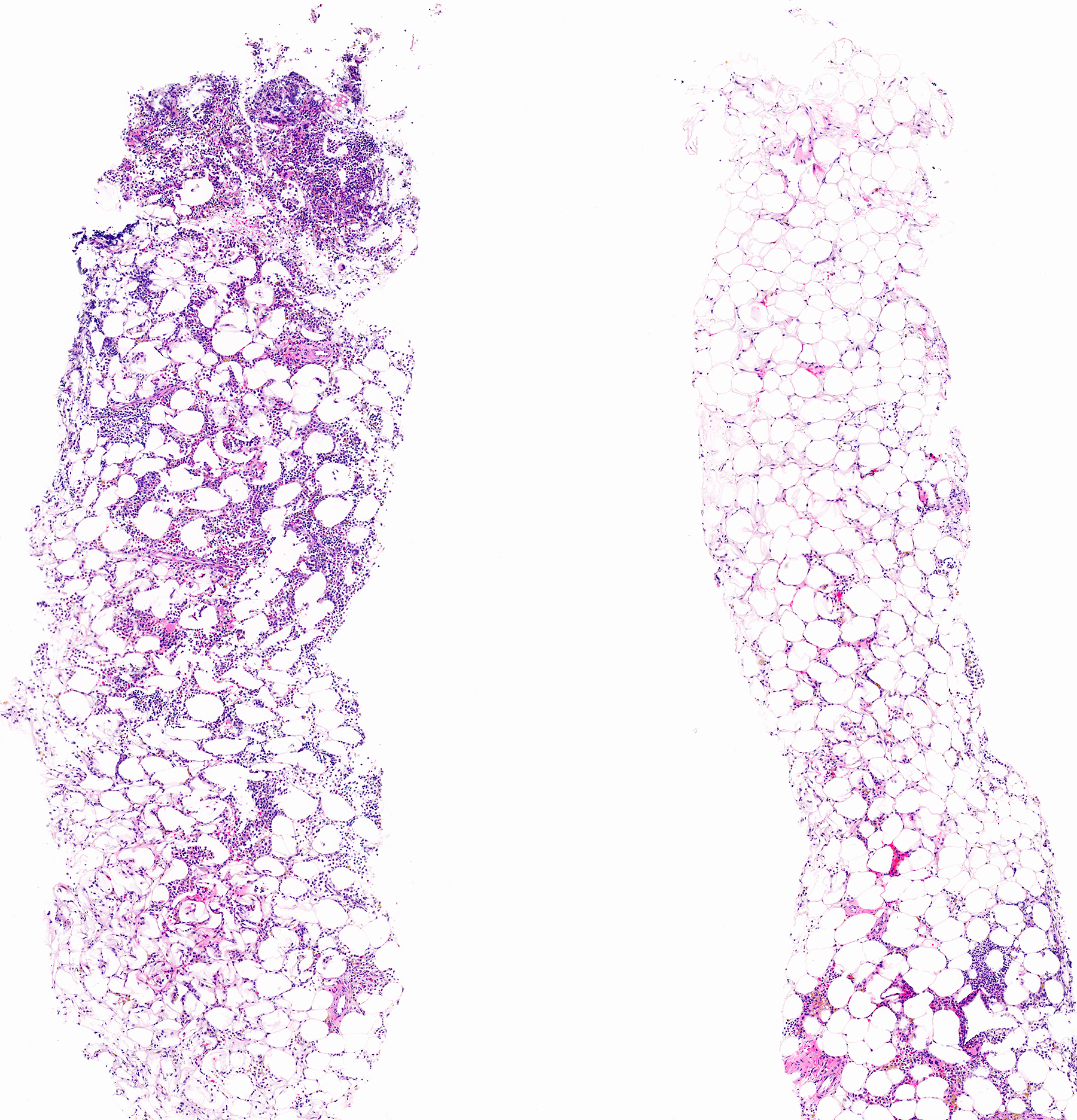
Hematopoietic cells on core biopsy

Myelolipoma
Cytology description
- Scattered hematopoietic cells admixed with mature fat cells
Sample pathology report
- Left adrenal gland, laparoscopic hand assisted adrenalectomy:
- Myelolipoma, 5.3 cm in greatest dimension
- Surgical margins are negative for tumor.
Differential diagnosis
- Adrenal lipoma:
- Mature fat cells
- No hematopoietic elements
- Angiomyolipoma:
- Classic triphasic appearance, including myoid spindle cells, mature adipocytes and thick walled hyalinized blood vessels
- No hematopoietic elements
- Vascular cyst:
- Mimicker in cases with extensive hemorrhage
- No adipocytes (but adipocytes may be seen in surrounding adrenal cortex with adipose metaplasia)
- No hematopoietic elements
- Liposarcoma:
- Mature adipocytes with atypical spindle cells embedded in fibrous stroma
- No hematopoietic elements
- Myeloid sarcoma:
- Usually associated with acute leukemia
Board review style question #1
The biopsy shown was taken from a 5 cm incidental mass in the adrenal gland of a 56 year old woman with no clinical symptoms. Which of the following is the patient’s diagnosis?
- Adrenal lipoma
- Angiomyolipoma
- Liposarcoma
- Myelolipoma
Board review style answer #1
Board review style question #2
Which of the following are the microscopic features of adrenal myelolipoma?
- Mature adipocytes with atypical spindle cells embedded in fibrous stroma
- Mature adipocytes with nuclear vacuolization
- Mature fat cells with trilineage hematopoiesis with markedly increased megakaryocytes
- Sheets of myeloid blasts with effacement of normal architecture
Board review style answer #2
C. Mature fat cells with trilineage hematopoiesis with markedly increased megakaryocytes. Mature adipocytes with atypical spindle cells embedded in fibrous stroma is associated with liposarcoma. Mature adipocytes with nuclear vacuolization is associated with lipoma. Sheets of myeloid blasts with effacement of normal architecture is associated with myeloid sarcoma.
Comment Here
Reference: Myelolipoma
Comment Here
Reference: Myelolipoma
