
Colon
Inflammatory bowel disease
Crohn's disease
Editorial Board Members: Aaron R. Huber, D.O., Naziheh Assarzadegan, M.D.


Last author update: 2 May 2022
Last staff update: 2 May 2022
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Crohn's disease [TI] colon pathology review [PT]

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Negative stains | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Ricuarte Archila L, Hagen CE. Crohn's disease. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/coloncrohns.html. Accessed April 26th, 2024.
Definition / general
- Chronic, relapsing, idiopathic inflammatory gastrointestinal disease
- Involvement of the upper and lower gastrointestinal tract in a discontinuous and transmural manner
Essential features
- Segmental, patchy inflammatory bowel disease, often involving the ileum, colon and upper GI tract
- Histologically characterized by chronic active colitis with associated transmural lymphoid aggregates and fissuring ulcers
- Noncaseating granulomas are characteristic but neither sensitive nor specific
- Main differential diagnosis: ulcerative colitis, indeterminate colitis and infectious colitis
Terminology
- Terminal ileitis
- Granulomatous enterocolitis
- Regional enteritis
Epidemiology
- Incidence: 0.003 - 0.02%
- Prevalence: 0.3%
- Slight female predominance in adult onset Crohn's disease
- Onset of disease at 20 - 40 years of age with a second peak described at the fifth to sixth decade of life
- More prevalent in Ashkenazi Jewish populations
- Incidence in Hispanic and Asian populations has increased in recent decades
- Incidence and prevalence are higher in high income countries and in urban areas, compared to low income countries and rural areas
- References: Mayo Clin Proc 2017;92:1088, Lancet 2017;389:1741
Sites
- Ileocolonic involvement: 30 - 40%
- Exclusive colon involvement: 30 - 40%, 50% rectal sparing
- Small bowel involvement: 80%
- Exclusive small bowel involvement: 30 - 40%
- Of patients with colon disease, 20% will develop ileal involvement in the next 10 years
- Of patients with ileal disease, 20% will develop colon involvement in the next 10 years
- 52% have right sided colitis, 40% have left sided colitis and 6% have pancolitis
- Approximately 25% have perianal complications, including fissures and fistulas
- Upper gastrointestinal complications are present in 5 - 30%, 50% in children and adolescents
- < 10% present with isolated perianal, upper gastrointestinal or extraintestinal complications
- Reference: Mod Pathol 2012;25:295
Pathophysiology
- Not fully understood
- Immunobiology: impaired intestinal barrier function and dysregulation of the innate and adaptative immune system responses, with an alteration of gut microbiota
- Deficient mucus biofilm barrier: decreased expression of mucin secretion genes (MUC1, MUC19 and PTGER4) in the terminal ileum in patients with Crohn's disease
- Permeability changes in the intestinal epithelium: altered expression of tight junction proteins (claudin)
- Paneth cell dysfunction
- Impaired autophagy of invasive microbes
- Imbalance of effector T cells and naturally regulatory T cells
- Recruitment and erratic retention of leukocytes
- Dysbiosis:
- Continuous alterations in intestinal microbiota resulting in clustering and reduced diversity in Firmicutes and Bacteroidetes phyla
- Reduction in Faecalibacterium prausnnitzii was associated with an increased recurrence of ileal Crohn's disease in the postoperative setting
- Genetic risk factors:
- Increased risk for individuals who have family history
- Concordance in monozygotic twins is 20 - 50% compared with 10% in dizygotic twins
- Wide genome association studies identified 200 loci associated to Crohn's disease; however, they contribute only a modest relative risk increase
- NOD2, ATG16L1, IL23R gene variants are responsible for some of the heritable risk
- Environmental risk factors:
- Cigarette smoking doubles the risk of developing Crohn's disease
- Reduced fiber dietary intake
- Antibiotic therapy during childhood increases the risk of developing Crohn's disease
- Other medications including nonsteroidal anti-inflammatory drugs, oral contraceptives and aspirin
- Breastfeeding appears to be a protective factor against the development of Crohn's disease
- References: Nat Rev Dis Primers 2020;6:22, Lancet 2012;380:1590
Etiology
- Idiopathic
Clinical features
- Signs and symptoms: abdominal pain, diarrhea, fatigue and weight loss
- Involvement of other GI sites can present as oral painful aphthous ulcers, odynophagia and dysphagia, postprandial vomiting and nausea, and malabsorption (including diarrhea and steatorrhea with associated nutritional deficiencies)
- 3 phenotypic clinical subtypes:
- Inflammatory phenotype: inflammation of the GI tract with no fistula or stenosing process; classic symptoms
- Stricturing phenotype: inflammation can progress to fibrosis and stenosis; symptoms are associated with bowel obstruction (i.e., lack of bowel movements, nausea and vomiting)
- Fistulizing phenotype: continuous transmural inflammation can cause sinus tract formation resulting in fistulas between bowel and other organs (vagina and bladder)
- Extraintestinal manifestations:
- Musculoskeletal: arthritis or arthropathy and bone loss
- Ocular: uveitis, iritis and episcleritis
- Cutaneous: erythema nodosum and pyoderma gangrenosum
- Hepatobiliary: primary sclerosing cholangitis, pyogenic liver abscess
- Renal: secondary amyloidosis leading to renal disease, calcium oxalate and uric acid renal stones
- Pulmonary: bronchiectasis, chronic bronchitis, interstitial lung disease, bronchiolitis obliterans with organizing pneumonia, sarcoidosis
- There are several clinical scoring systems that categorize patients into low and high risk (e.g., Crohn's disease activity index and Harvey-Bradshaw index)
- Endoscopic findings:
- Ileocolonoscopy is the gold standard for diagnosis
- Ulceration: small aphthous ulcers (< 5 mm) and transmural ulcers
- Cobblestone appearance: linear and serpiginous ulcers with intervening nonulcerated mucosa
- Skip lesions: discontinuous lesions surrounded by adjacent normal tissue
- Other (less specific) findings:
- Normal rectal mucosa
- Inflammation of the terminal ileum with no colonic inflammation
- Ileocolonoscopy is the gold standard for diagnosis
- References: Mayo Clin Proc 2017;92:1088, Inflamm Bowel Dis 2011;17:471, Gastroenterol Rep (Oxf) 2018;6:75
Diagnosis
- Diagnosis consists of a combination of clinical findings and complementary diagnostic tests including blood tests, stool tests, upper and lower endoscopic studies, radiologic imaging and histologic evaluation
- The aim is to exclude differential diagnoses, establish a diagnosis and classify the severity of the disease
Laboratory
- C reactive protein: nonspecific marker for acute inflammation; correlates with disease activity
- ASCA (anti-Saccharomyces cerevisiae antibodies): positive in 60 - 70% of patients with Crohn's disease, 10 - 15% of patients with ulcerative colitis and < 5% of patients without inflammatory bowel disease
- pANCA (perinuclear antineutrophil cytoplasmic antibodies): positive in 10 - 15% of patients with Crohn's disease, positive in 60 - 70% of patients with ulcerative colitis
- Patients with Crohn's disease with positive pANCA tend to have an ulcerative colitis resembling phenotype
- Fecal calprotectin: fecal biomarker used to distinguish between inflammatory bowel disease and functional bowel disease; elevated levels of fecal calprotectin indicate the need for further investigation for inflammatory bowel disease
- Reference: Lancet 2017;389:1741
Radiology description
- Frequently used to assess disease in the small bowel: bowel ultrasonography, CT scan and MRI are helpful for the assessment of the extent of the disease and presence of complications
- Small bowel findings:
- Asymmetrical segmental mural hyperenhancement: specific to Crohn's disease; other types of segmental mural hyperenhancement are less specific
- Wall thickening
- Intramural edema: indicative of bowel inflammation
- Strictures: more common with fibrosis and inflammation; proximal bowel dilation can correlate with higher fibrotic burden
- Ulcers: indicative of severe inflammation (Radiology 2018;286:776)
- Pelvic MRI: used to evaluate and define perianal fistula tracts (Radiology 2017;282:628)
Radiology images
Images hosted on other servers:

CT enterography, small bowel Crohn's disease

MRI of Crohn's disease patient with anovaginal fistula
Prognostic factors
- Associated with a 1.38 increase in mortality
- Recurrence in approximately 95% of patients after 10 years of diagnosis, most commonly as ileocolonic disease
- Postoperative recurrence is dependent on disease location
- Isolated ileal disease recurrence is proximal to anastomosis
- Ileocolitis disease recurrence frequently occurs both proximal and distal to the anastomosis (Gut 2012;61:1140)
- Increased risk for relapse, surgery or complications:
- Patient features:
- Young age at diagnosis (< 40 years)
- Smoking
- Disease features:
- High disease burden and prolonged duration of disease
- Perianal disease
- Stricturing disease
- Involvement of the upper GI tract
- Requiring corticosteroids during first flare
- Lack of epithelial healing after clinical remission
- Presence of deep ulcers
- Granulomas on biopsy specimen
- Laboratory tests:
- High C reactive protein and ASCA
- High fecal calprotectin levels
- Low serum levels of albumin and hemoglobin
- Patient features:
- Patients with Crohn's disease have an increased risk for:
- Colorectal cancer and death from colorectal cancer (Lancet Gastroenterol Hepatol 2020;5:475)
- Small bowel carcinoma (Ann Oncol 2009;20:574, Dig Liver Dis 2021;53:809)
- Anal squamous cell carcinoma (Cancers (Basel) 2021;13:1445, J Crohns Colitis 2017;11:1011)
- Lymphoproliferative disorders (Ann Oncol 2009;20:574, Dig Liver Dis 2021;53:809)
Case reports
- 3 year old boy with a case of early childhood Crohn's disease (Hosp Pediatr 2016;6:248)
- 12 year old girl with the cobblestone sign (Dtsch Arztebl Int 2017;114:472)
- 20 year old man with type 2 autoimmune pancreatitis with Crohn's disease (Intern Med 2018;57:2957)
- 31 year old man with pulmonary Crohn's disease (Dig Dis Sci 2017;62:64)
- 37 year old woman with unusual presentation of Crohn's disease (BMJ Case Rep 2021;14:e242703)
- 6 cases of colorectal cancer in Crohn's disease (Surg Case Rep 2021;7:152)
Treatment
- Mainstay of treatment is medical therapy with a goal to achieve clinical, endoscopic and histologic remission, demonstrated by complete mucosal healing
- Chosen based on disease stage, severity and location
- Low risk patients: step up therapy; initially less potent medications with better adverse effect profile are used, while more potent medications are reserved for patients who do not respond to the initial approach
- High risk patients: top down therapy; potent therapies, including biologic therapy and immunomodulators, are used early in the disease to prevent complications
- Medical therapies:
- Corticosteroids
- Thiopurines
- Methotrexate
- Anti-TNF agents
- Surgical therapy: approximately 50% of patients with Crohn's disease will have at least 1 surgical procedure due to disease complications
- Stricturing disease: irreversible with medical therapy; if obstructive symptoms are ongoing, surgery may be indicated
- Fistulizing disease: cases of enterovesicular, enterovaginal and enterocutaneous fistulas or sinus tract and abscess formation
- Perianal disease: perianal fistula or abscess
- Reference: Gastroenterology 2014;147:702
Clinical images
Images hosted on other servers:

Endoscopic features of Crohn's disease
Gross description
- Segmental involvement of the bowel
- Creeping fat due to transmural inflammation
- Thickened and fibrotic bowel walls with stricture formation
- Mucosal aphthous ulcers surrounded by hyperemia with eventual formation of a cobblestone appearing mucosa
- Inflammatory pseudopolyps
- Fissures, sinus and fistulous tracts and abscesses in the setting of complicated disease
- Perforations, rarely
- Reference: Odze and Goldblum: Surgical Pathology of the GI Tract, Liver, Biliary Tract and Pancreas, 3rd Edition, 2015
Gross images
Contributed by Elizabeth Heidi Cheek-Norgan, M.H.S., PA (ASCP) and Catherine E. Hagen, M.D.
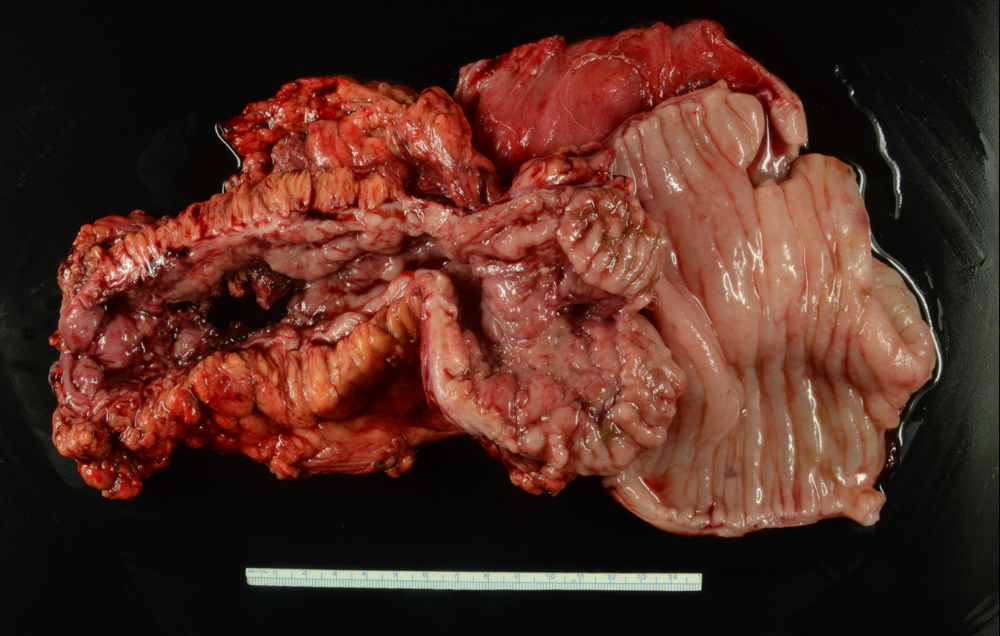
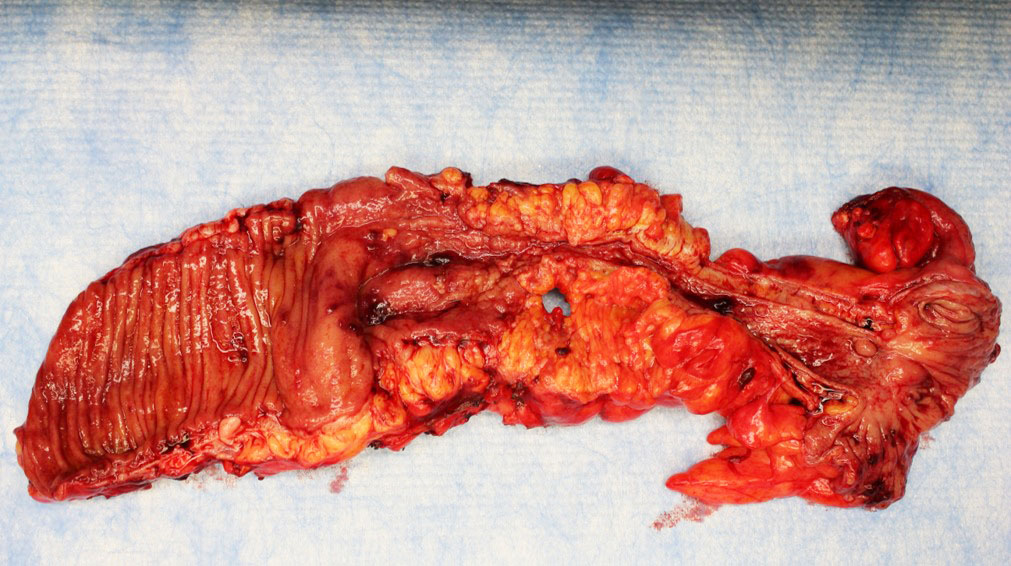
Stricture
Microscopic (histologic) description
- Similar to ulcerative colitis, untreated cases typically show features of active chronic colitis
- Features of chronicity include:
- Crypt architectural distortion
- Inflammatory expansion of the lamina propria with basal lymphoplasmacytosis
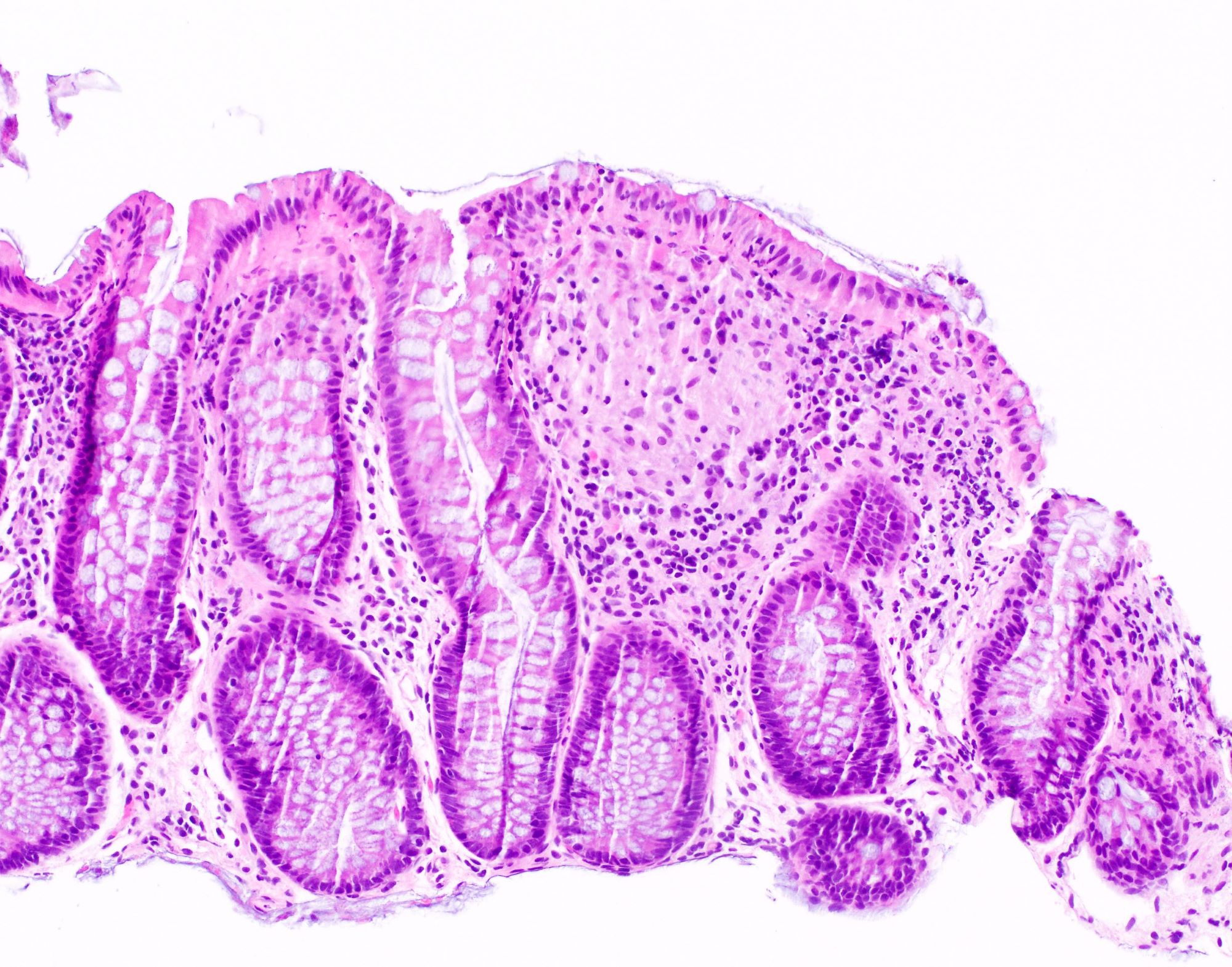
- Paneth cell metaplasia or hyperplasia
- Pyloric gland metaplasia of small bowel and right colon
- Features of activity include neutrophilic inflammation with cryptitis, crypt abscess and ulceration
- Patchy and segmental distribution with skip lesions
- Aphthous ulcers and deep fissuring ulcers
- Granulomas are characteristic but only present in approximately 50% of patients (Colorectal Dis 2011;13:1142)
- Often well formed and sarcoid-like but may be poorly formed or consist of giant cells
- Should be distinguished from crypt rupture granuloma
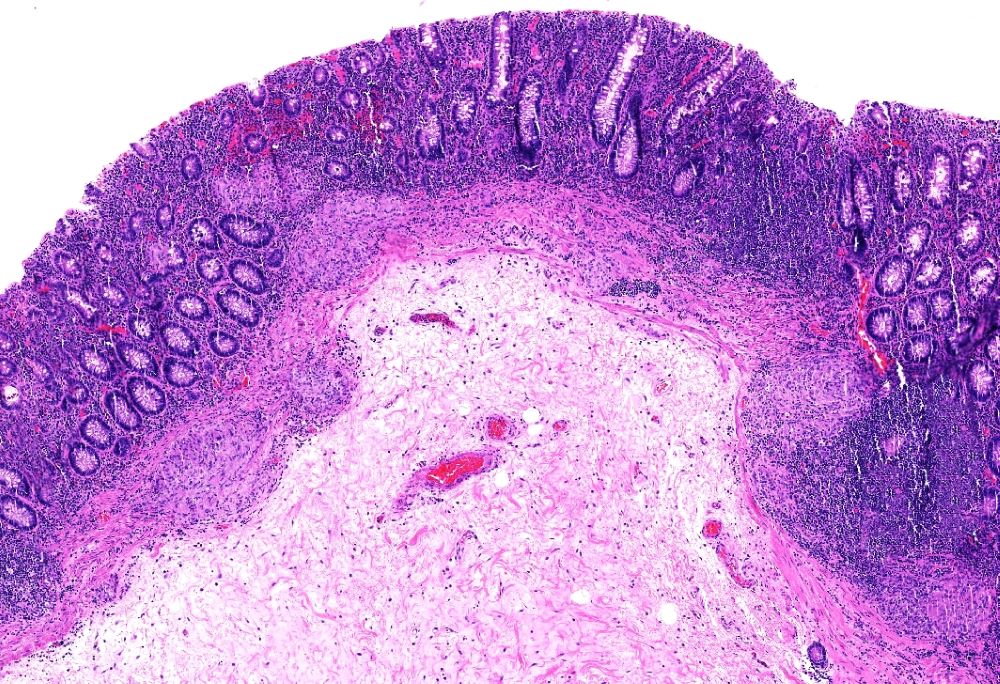
- Transmural inflammation with lymphoid aggregates in the subserosal adipose tissue
- Sinus tracts and fistula formation
- Biopsies are limited in determining the depth and distribution of inflammation; therefore, diagnosis is often reliant on clinical correlation or examination of the resection specimen (Histopathology 2014;64:317)
- Dysplasia may be present in patients with longstanding disease
- Activity is usually graded similar to ulcerative colitis (Gastroenterology 2007;133:1099):
- Inactive: absence of neutrophils
- Mild: activity involving < 50% of the mucosa
- Moderate: activity involving > 50% of the mucosa; crypt abscesses often seen
- Severe: presence of surface ulceration or erosion
- References: Histopathology 2014;64:317, Best Pract Res Clin Gastroenterol 2019;38:101601
Microscopic (histologic) images
Contributed by Catherine E. Hagen, M.D. and Luisa Ricaurte Archila, M.D.
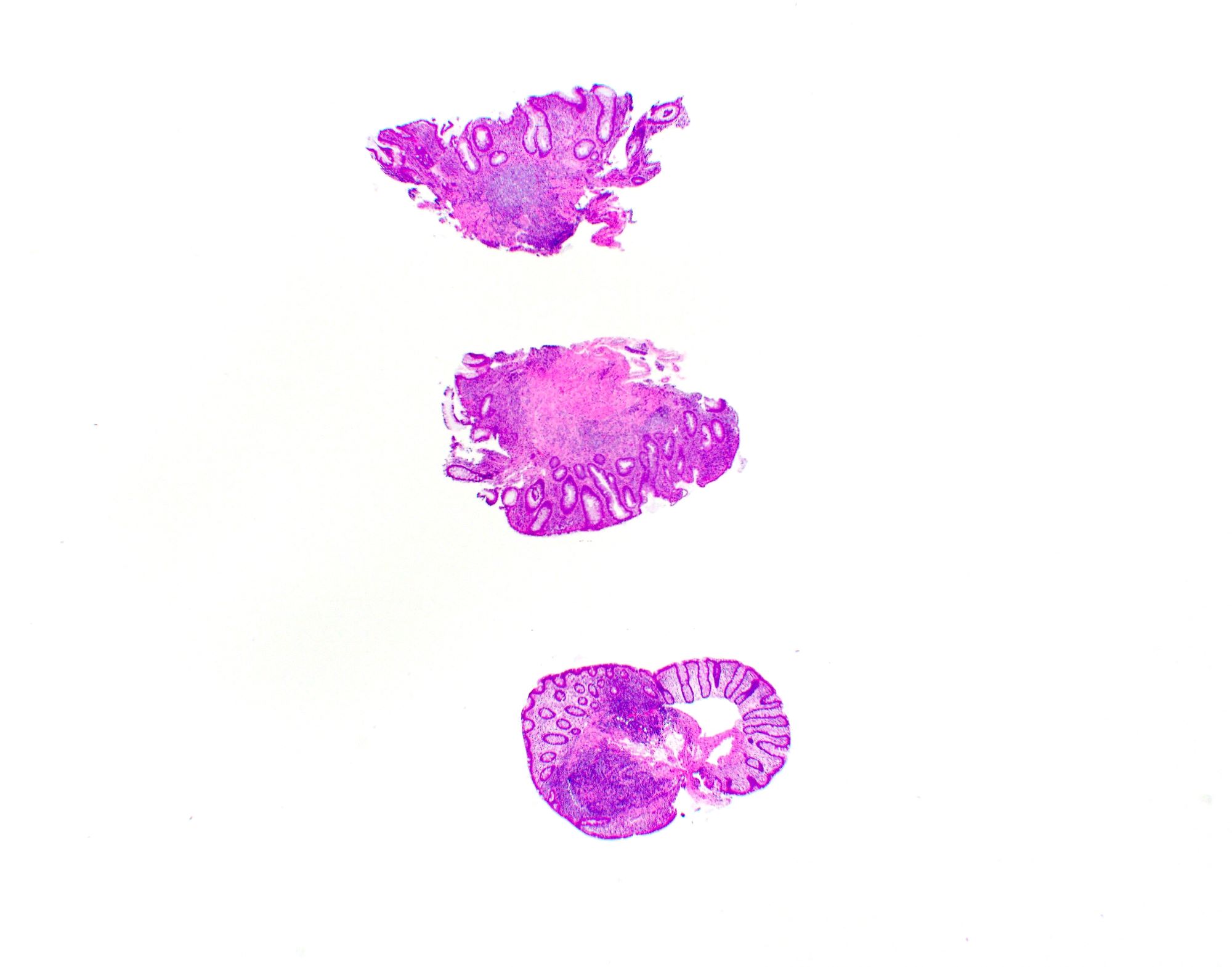
Patchy involvement
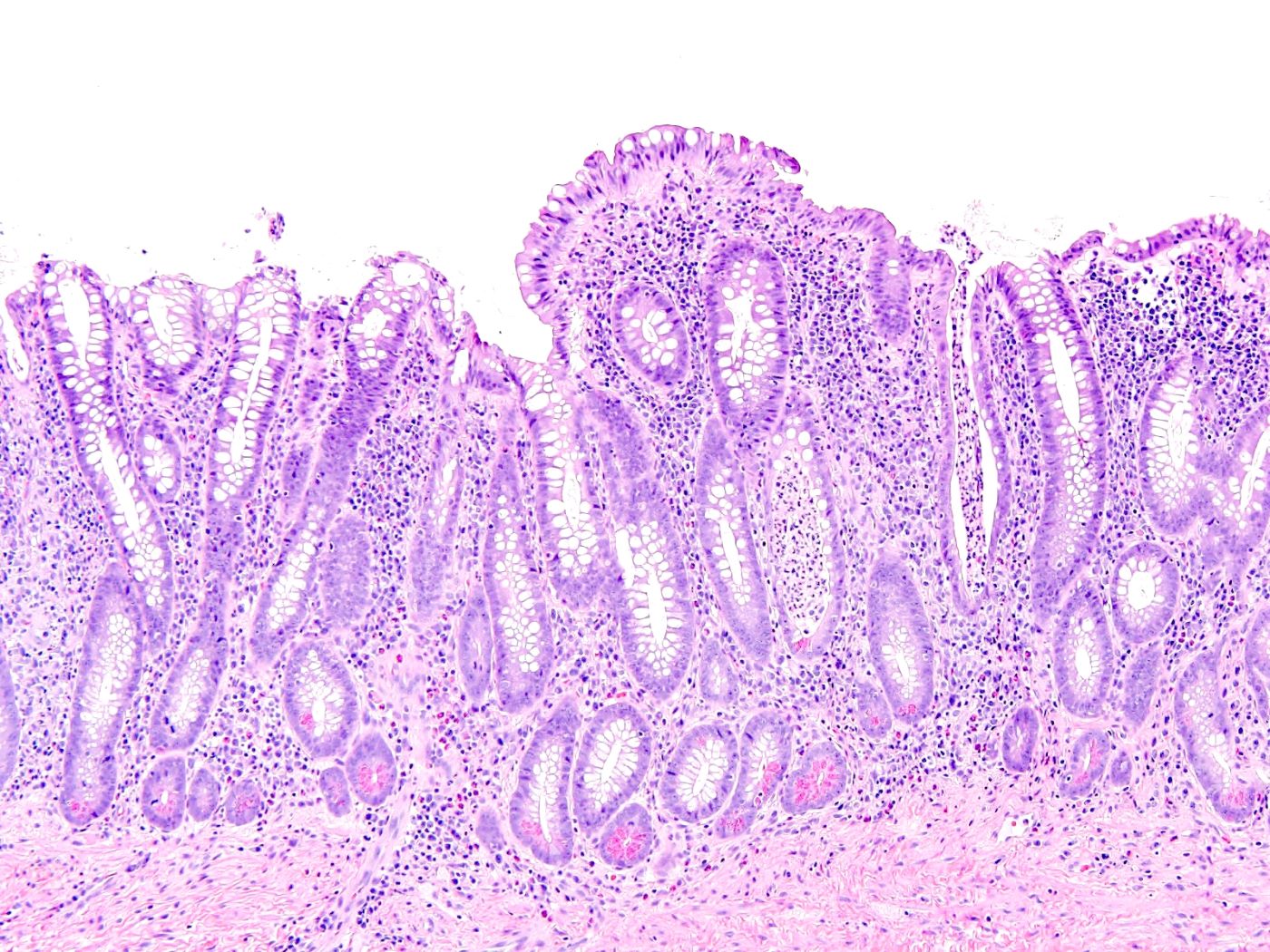
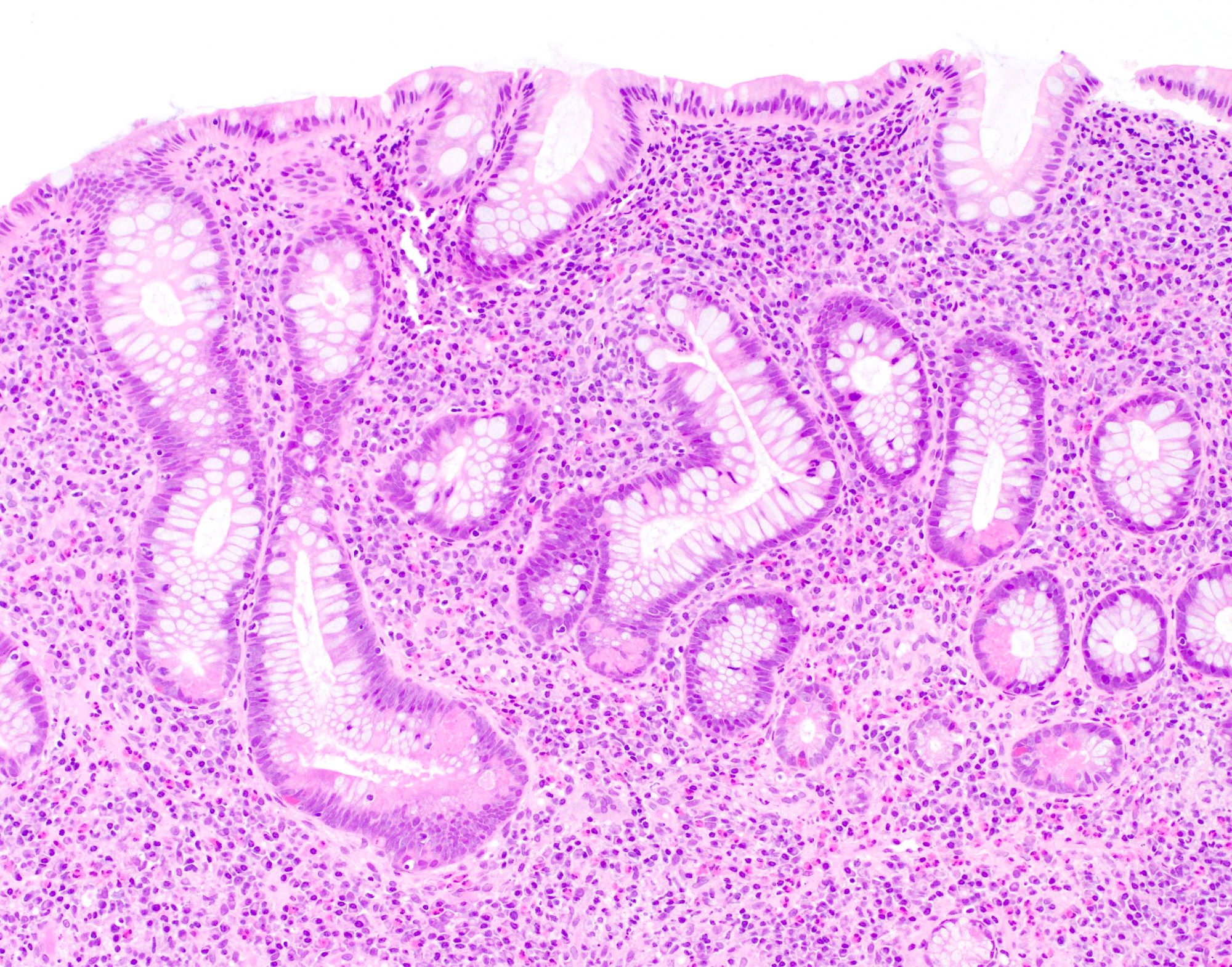
Active chronic colitis
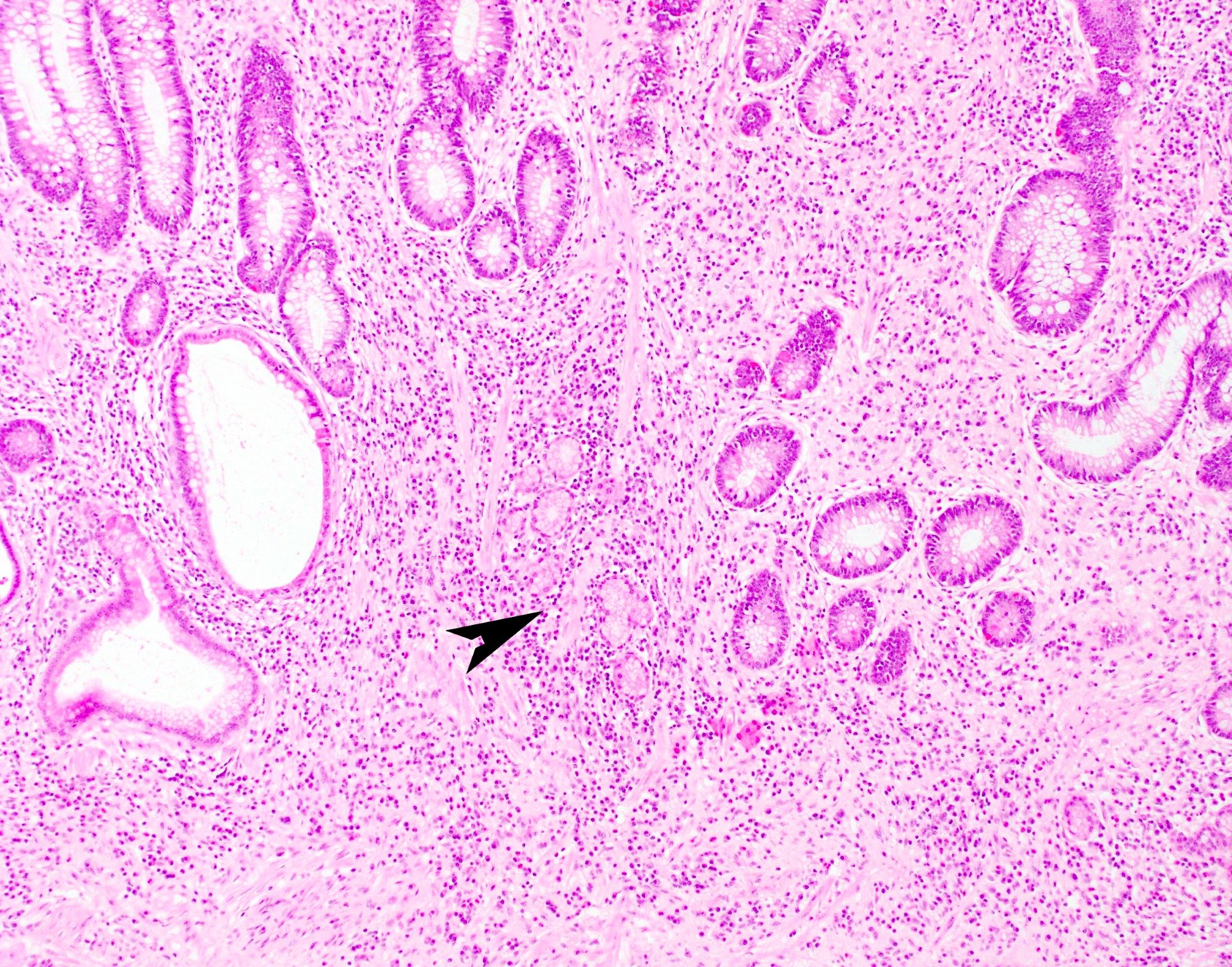
Pyloric gland metaplasia
Granuloma
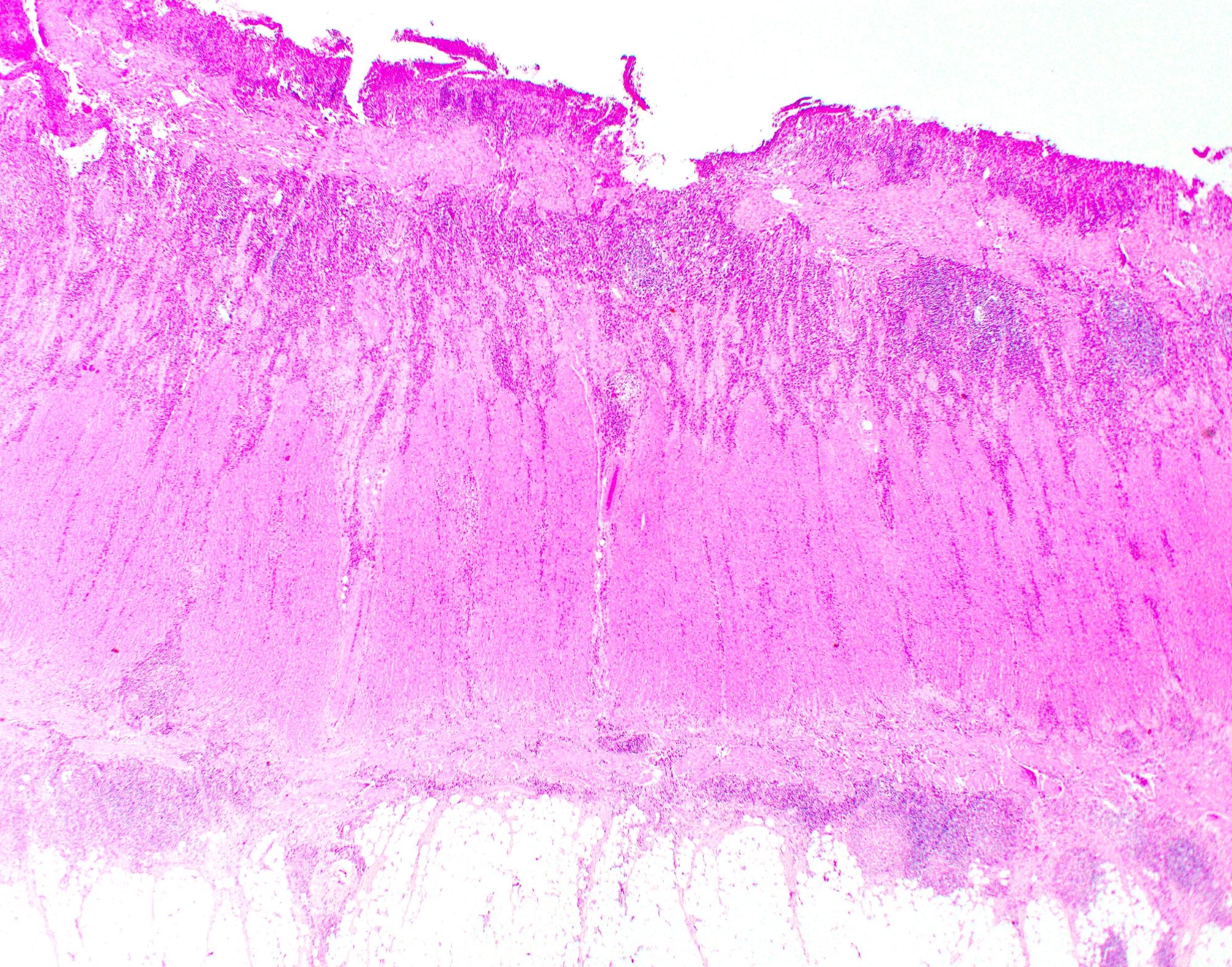
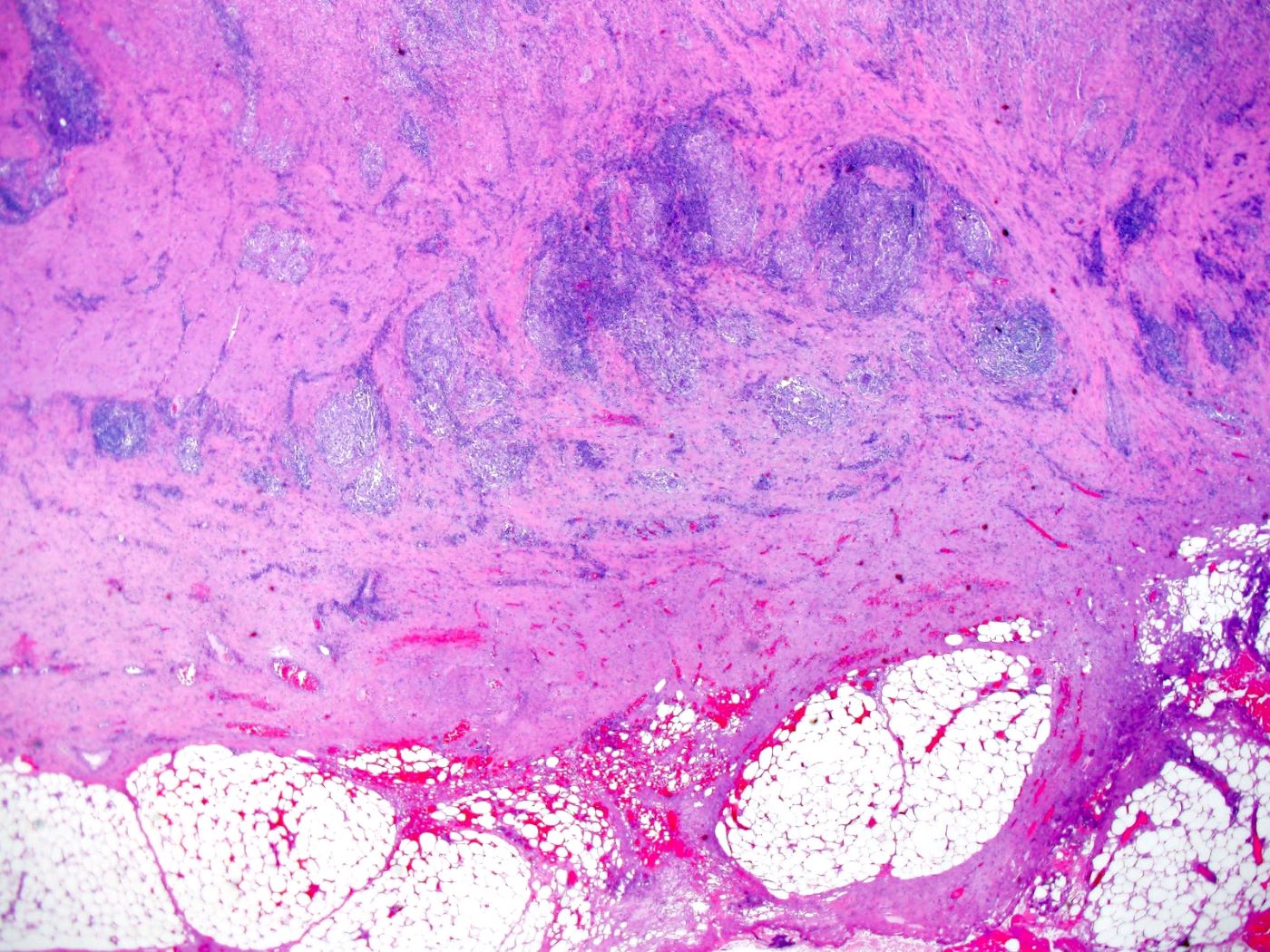
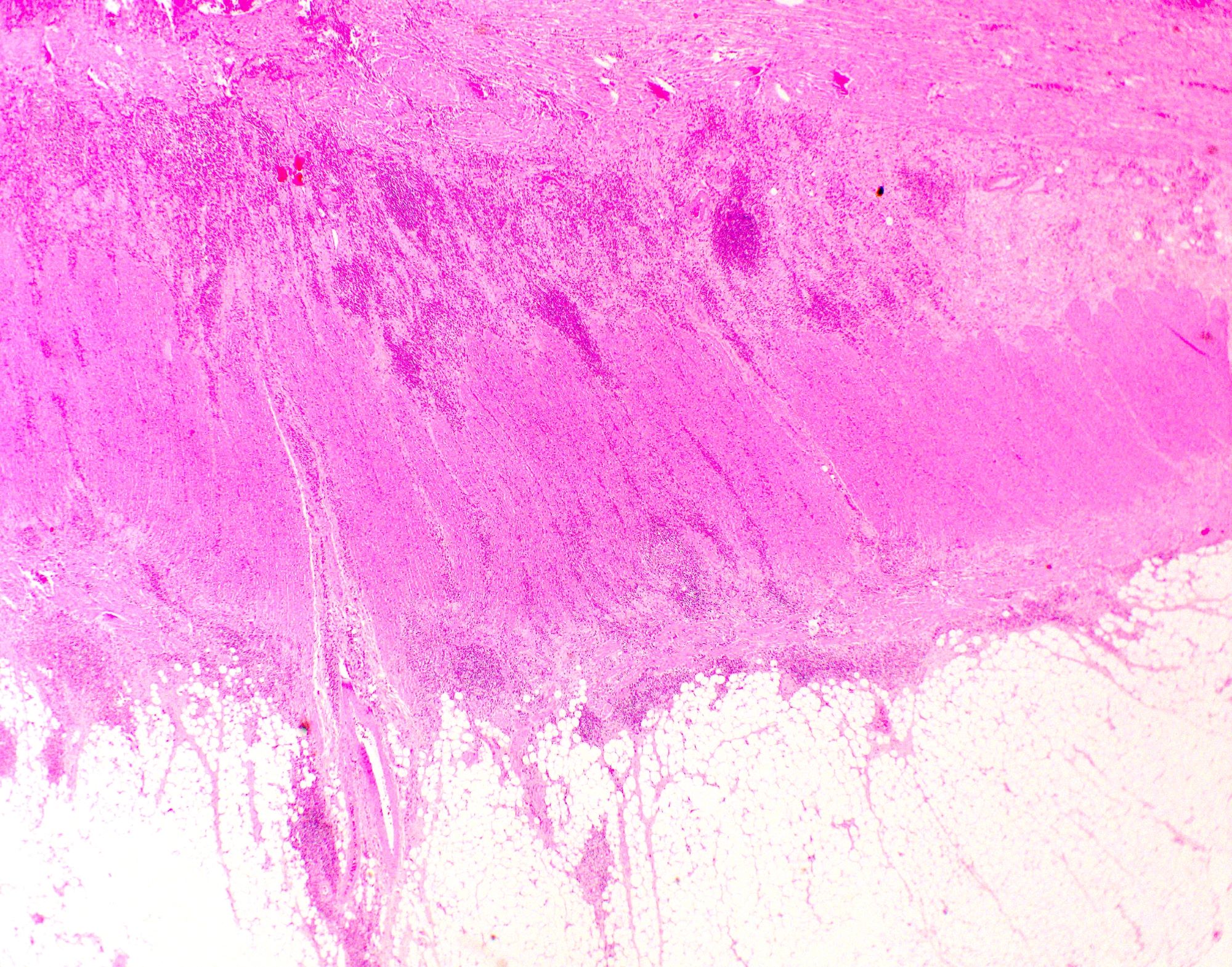
Transmural inflammation
Negative stains
Sample pathology report
- Colon, biopsy:
- Mildly active chronic colitis with multiple nonnecrotizing granulomas (see comment)
- Comment: The histologic findings are suggestive of idiopathic inflammatory bowel disease. Presence of multiple nonnecrotizing granulomas favors Crohn's disease over ulcerative colitis but clinical correlation with distribution of disease is required.
- Colon, resection:
- Severely active chronic colitis with transmural inflammation and fissuring ulcers compatible with Crohn's colitis; no dysplasia or malignancy
Differential diagnosis
- Ulcerative colitis:
- Diffuse involvement of the colon and rectum
- Absence of skip lesions, except in treated cases
- Absence of granulomas, except when associated with ruptured crypts
- Backwash ileitis: in the setting of severe cecal disease, frequently without severe activity or chronic changes
- Indeterminate colitis:
- Diagnosis of exclusion when it is impossible to distinguish between ulcerative colitis and Crohn's disease
- This term is only used when a resection specimen is available
- Infectious colitis:
- Presence of noncaseating granulomas
- Yersinia:
- Central necrosis within granulomas and lack of transmural inflammation
- Salmonella and Campylobacter:
- Poorly circumscribed microgranulomas
- Tuberculosis:
- Florid coalescent granulomatous inflammation, extensive caseous necrosis and nodal granulomas with no intramural granulomas
- Segmental colitis associated with diverticulitis:
- Inflammation limited to segment of colon with diverticulosis
Board review style question #1
A 45 year old woman underwent ileocolectomy for fulminant colitis. Representative sections were submitted for histology (shown above). What is the most likely diagnosis based on the histologic features?
- Collagenous colitis
- Crohn's disease
- Ischemic colitis
- Ulcerative colitis
Board review style answer #1
Board review style question #2
Which of the following features favors Crohn's disease over ulcerative colitis?
- Crypt architectural distortion
- Diffuse, continuous involvement of colon
- Nonnecrotizing granulomas
- Superficial, broad based ulceration
Board review style answer #2
