Colon
Inflammatory bowel disease
Inflammatory bowel disease, indeterminate type
Editorial Board Member: Catherine E. Hagen, M.D.
Deputy Editor-in-Chief: Raul S. Gonzalez, M.D.


Last author update: 26 April 2021
Last staff update: 4 October 2021
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: indeterminate colitis [TI]

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Sites | Diagnosis | Laboratory | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Sample pathology report | Differential diagnosis | Practice question #1 | Practice answer #1Cite this page: Paulsen JD, Polydorides AD. Inflammatory bowel disease, indeterminate type. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/colonindeterminate.html. Accessed October 2nd, 2025.
Definition / general
- Inflammatory bowel disease (IBD), indeterminate type is a provisional term used to describe cases of IBD in which a definitive diagnosis of ulcerative colitis or Crohn's disease cannot be established on the basis of histopathological and clinical (including radiologic and endoscopic) data
- IBD, indeterminate type is not a specific disease entity and has no established diagnostic criteria (Mod Pathol 2015;28:S30, J Clin Pathol 2004;57:1233)
- Comprises 5 - 15% of IBD cases but most will eventually be declared as 1 of the 2 subtypes (only up to 15% thought to be Crohn's disease)
Essential features
- IBD, indeterminate type is a diagnosis of exclusion and should only be used in resection specimens when it is impossible to distinguish ulcerative colitis from Crohn's disease
- Term should be avoided in the following circumstances:
- Recognized IBD variants: appendiceal or cecal patch in left sided ulcerative colitis, patchy / segmental disease (including rectal sparing) in treated or longstanding ("burned out") ulcerative colitis, fulminant (severe or toxic) ulcerative colitis, ulcerative colitis with backwash ileitis, ulcerative colitis with cryptolytic granulomas, superficial (ulcerative colitis-like) Crohn's disease
- In the presence of convincing criteria for Crohn disease: nonnecrotizing, noninfectious epithelioid granulomas, true segmental colonic or small bowel disease, extensive transmural lymphoid aggregates underlying intact mucosa, definitive perianal or fistulizing disease
- Secondary or superimposed non-IBD colitides, e.g. infectious colitis, ischemic colitis, diverticular disease associated colitis, diversion colitis, microscopic colitis (i.e., lymphocytic or collagenous colitis), pseudomembranous colitis, colitis due to medication related injury (e.g. nonsteroidal anti-inflammatory drugs (NSAIDs), mycophenolate, immune checkpoint inhibitors), etc.
- In the setting of insufficient clinical, pathologic, radiologic or endoscopic data (e.g. on biopsy material in the absence of granulomas): use the term "IBD, unclassified" instead
- Even though up to 15% will ultimately receive a diagnosis of Crohn's disease, patients with IBD, indeterminate type are generally thought to have similar ileal pouch anal anastomosis (IPAA) failure rates as ulcerative colitis; therefore, IPAA surgery is probably warranted in most cases
- Higher rates of IBD, indeterminate type diagnosis are seen in the pediatric population, given the patchy disease distribution often seen in childhood ulcerative colitis
Terminology
- Indeterminate colitis (IC):
- Inexact and confusing term; not limited to IBD per se
- Used in some instances when the etiology of chronic colitis cannot be ascertained from clinicopathologic findings; in these cases, nonspecific colitis or chronic active colitis, type unknown is preferred, accompanied by a note as to the reason for the uncertainty and possible differential diagnoses
- Inflammatory bowel disease, unclassified (IBD-U):
- Primarily a temporary term used during colonoscopy when the pathologist or gastroenterologist favors a diagnosis of IBD but the histologic or endoscopic impression do not permit distinction between ulcerative colitis and Crohn's disease
- In most cases, a diagnosis of ulcerative colitis or Crohn's disease can be yielded upon evaluation of follow up resection specimens or additional clinical data
- Other terms:
- Colitis of uncertain type or etiology (CUTE) (Inflamm Bowel Dis 2008;14:850)
- IBD, NOS (not otherwise specified)
- IBD, unknown etiology
- Uncertain colitis
ICD coding
Sites
- Colon
Diagnosis
- IBD, indeterminate type is a diagnosis of exclusion and requires conflicting histopathological findings in a resection specimen or in the setting of contradictory clinical or radiological data
Laboratory
- Limited clinical utility of serological markers ASCA and pANCA
- ~50% of patients with IBD, indeterminate type are ASCA- / pANCA- (Gastroenterology 2002;122:1242)
- Only in a minority of patients do serologic markers help establish a definitive diagnosis of Crohn's disease (ASCA+ / pANCA-) or ulcerative colitis (ASCA- / pANCA+) (Gastroenterology 2002;122:1242)
Prognostic factors
- Similar ileal pouch anal anastomosis failure rates as ulcerative colitis (J Crohns Colitis 2020;14:1010, Am Surg 2016;82:977, J Gastrointest Surg 2017;21:56, Gastroenterol Hepatol (N Y) 2017;13:466)
- Higher overall ileal pouch anal anastomosis complication rates than ulcerative colitis, including pouch fistula, pelvic sepsis, abscess, perineal complications and ultimate diagnosis of Crohn's disease (J Crohns Colitis 2020;14:1010, J Gastrointest Surg 2017;21:56)
- ~15% of cases ultimately receive a diagnosis of Crohn's disease (Dis Colon Rectum 2000;43:1487)
- Higher rate of the diagnosis seen in the pediatric population, given frequent findings of rectal sparing and patchy disease in childhood ulcerative colitis that generates diagnostic difficulty (Inflamm Bowel Dis 2006;12:258, J Pediatr Gastroenterol Nutr 2007;44:653)
Case reports
- 3 year old boy with bloody diarrhea for 5 months (Am J Gastroenterol 1993;88:105)
- 21 year old woman with longstanding colitis (Semin Gastrointest Dis 2001;12:211)
- 22 year old man with watery diarrhea, fever and nausea (Z Gastroenterol 1997;35:481)
Treatment
- Same as IBD
- Given similar ileal pouch anal anastomosis failure rates as ulcerative colitis, ileal pouch anal anastomosis probably warranted (Gastroenterol Hepatol (N Y) 2017;13:466)
Gross description
- Ulcerative colitis-like colectomy specimen showing predominantly continuous, mucosa based inflammation but with 1 or more Crohn's disease-like features, such as:
- Rectal sparing (except when treated or longstanding colitis)
- Proximal skip lesions (except in pediatric population)
- Ulceration in small bowel (even in the setting of backwash ileitis)
- Deep fissuring ulceration (in the absence of fulminant colitis or history thereof)
- Focal wall thickening
- "Cobblestone" mucosa (deep linear ulcers with intervening normal mucosa)
- Left sided colitis with discontinuous cecal or appendiceal orifice involvement (so called “cecal patch” or “periappendiceal red patch”) is a well recognized variant of ulcerative colitis and should not be designated as IBD, indeterminate type
- References: Mod Pathol 2015;28:S30, J Clin Pathol 2004;57:1233, Histopathology 2007;50:83, J Clin Pathol 2009;62:201
Gross images
Contributed by John D. Paulsen, M.D. and Alexandros D. Polydorides, M.D., Ph.D.
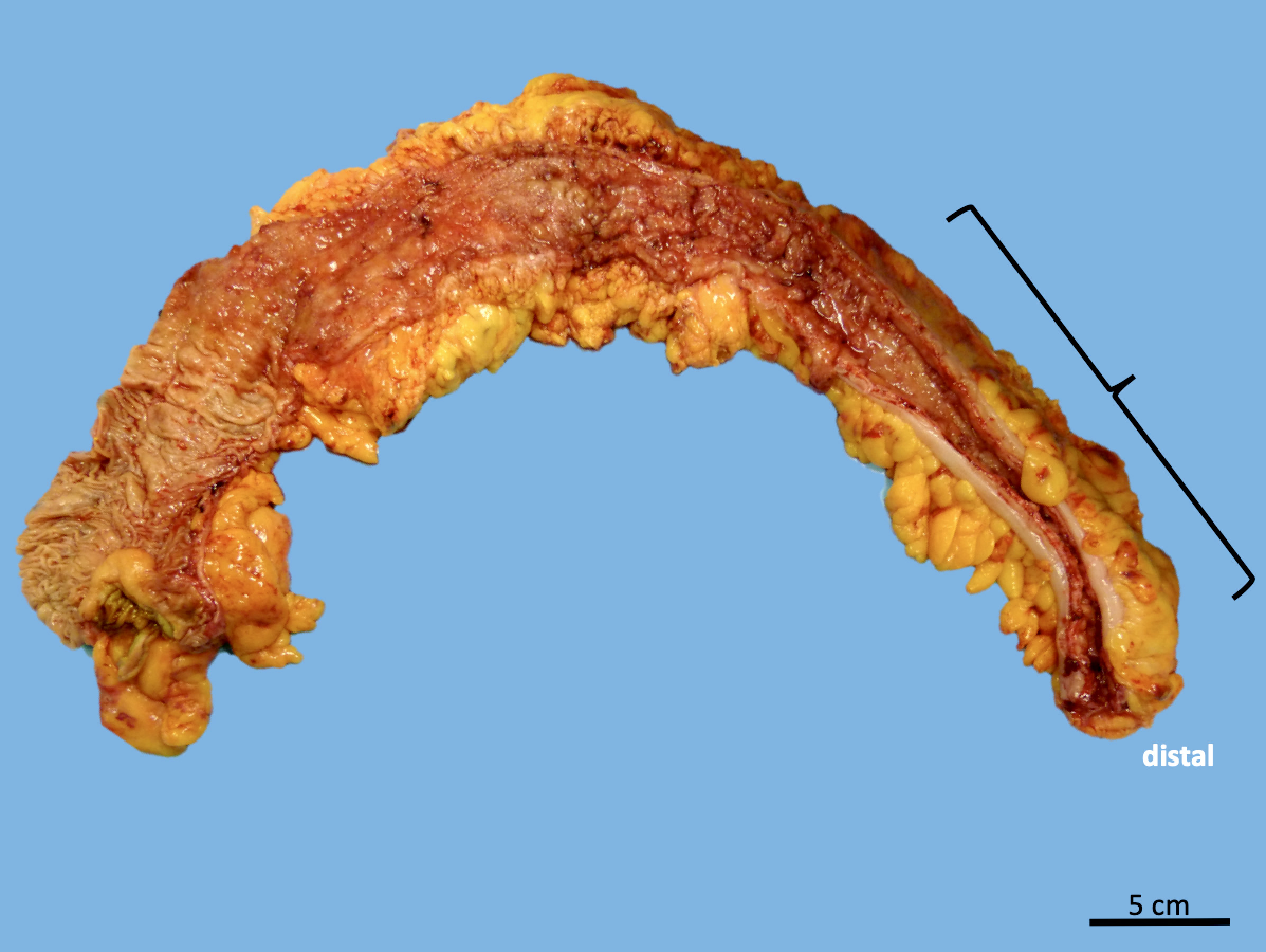
IBD, indeterminate type
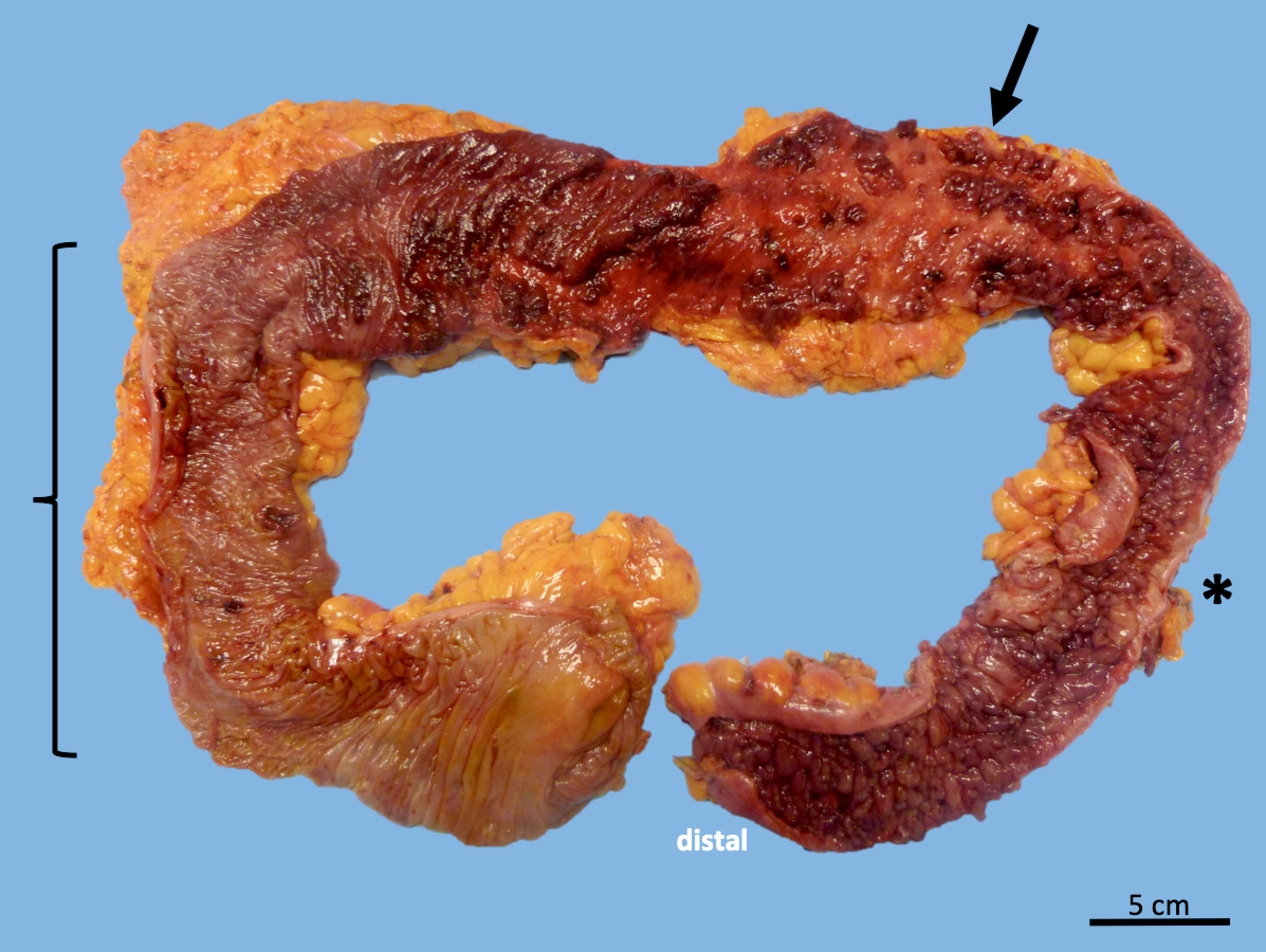
IBD, indeterminate type, favor Crohn's disease
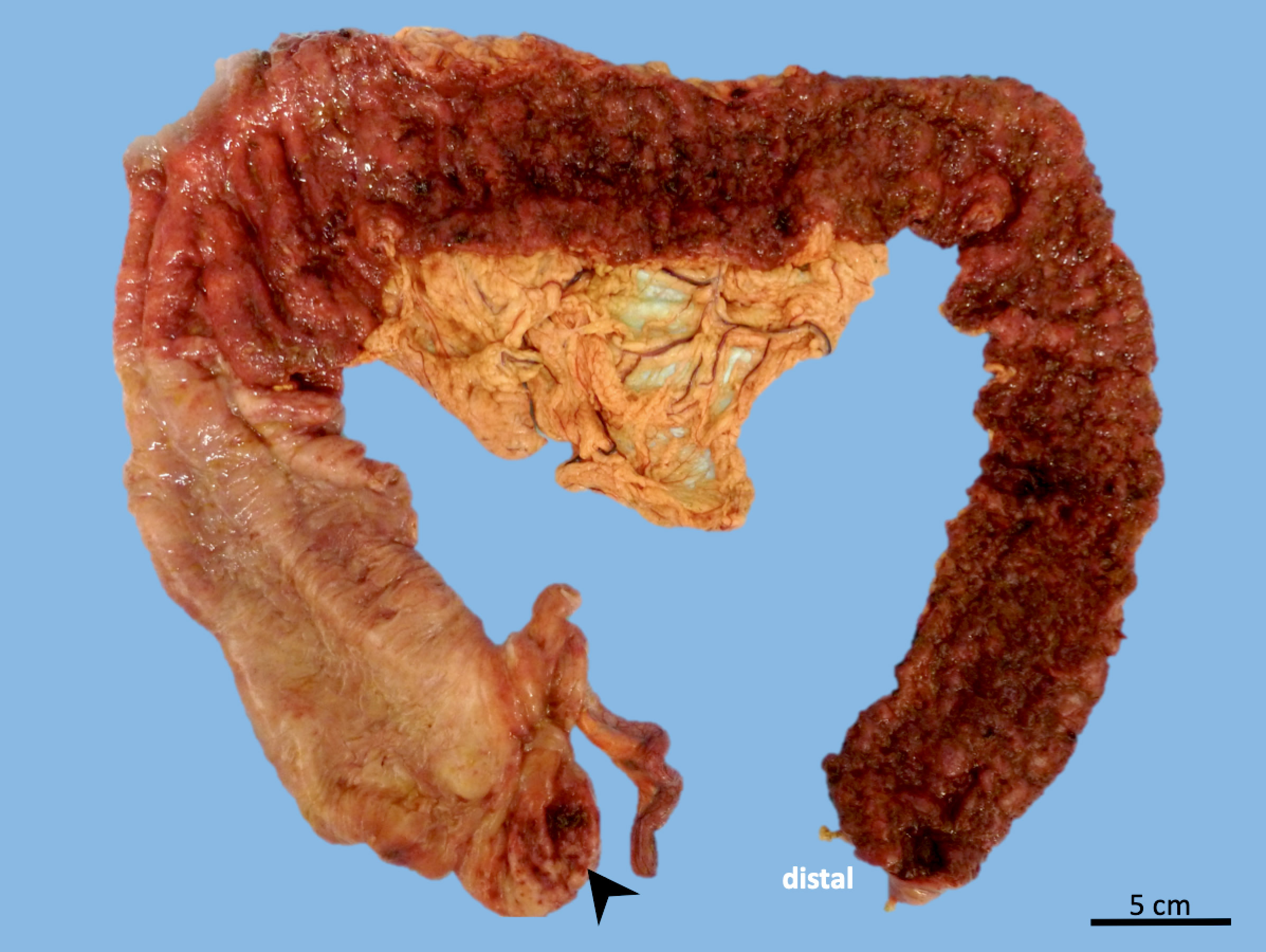
Mimic: ulcerative colitis with cecal patch
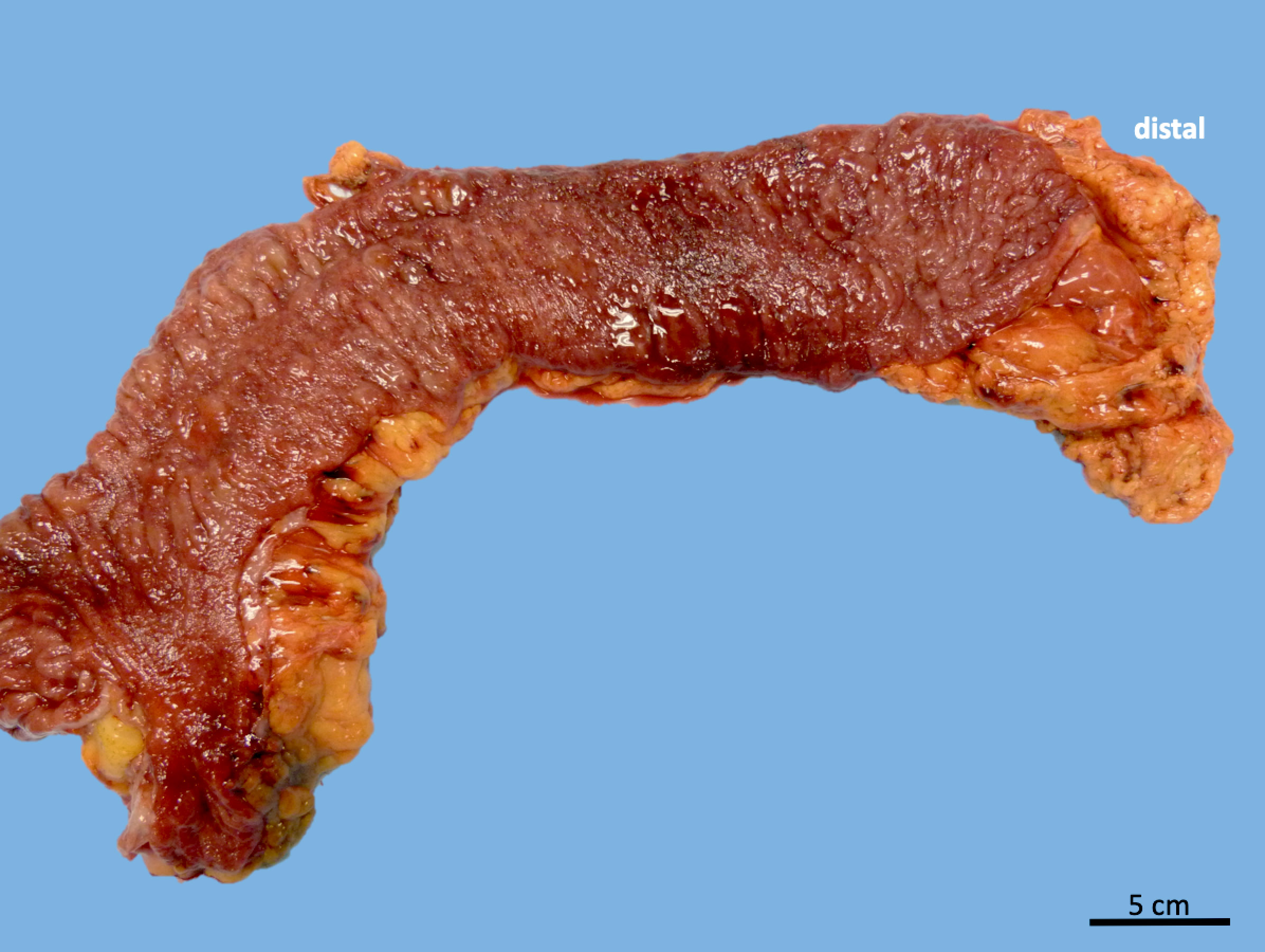
Mimic: superficial
(ulcerative
colitis-like)
Crohn's disease
Microscopic (histologic) description
- Active mucosal inflammation (same as IBD) (J Clin Pathol 2009;62:201):
- Cryptitis (neutrophilic infiltration of crypt epithelium)
- Crypt abscess (crypt with intraluminal aggregates of neutrophils)
- Erosions
- Ulceration
- Chronic mucosal inflammation (same as IBD) (J Clin Pathol 2009;62:201):
- Increased lymphoplasmacytic inflammation in the lamina propria with loss of gradient (i.e. lack of increased infiltrates near lumen)
- Basal plasmacytosis (so called crypt shortfall)
- Evidence of chronic injury (same as IBD) (J Clin Pathol 2009;62:201):
- Paneth cell metaplasia (Paneth cells are normally absent distal to the mid transverse colon)
- Crypt architectural distortion (branched, dilated and disorganized crypts)
- Microscopic features that are still compatible with ulcerative colitis and do not warrant a diagnosis of Crohn's disease or IBD, indeterminate type (Mod Pathol 2015;28:S30, J Clin Pathol 2004;57:1233):
- Cryptolytic granulomas
- Backwash ileitis: active inflammation in the terminal ileum in the setting of at least similar in intensity active inflammation in the cecum; usually there is minimal or no chronicity in the ileum
- Microscopic features considered major diagnostic criteria for Crohn's disease (Mod Pathol 2015;28:S30, J Clin Pathol 2004;57:1233):
- True segmental disease of the colon (in untreated patients)
- Absence of rectal involvement (in untreated patients)
- Transmural lymphoid aggregates (away from deep mucosal ulcers)
- Penetrating sinus tracts or fistulas (unrelated to other causes, e.g. diverticulitis)
- Nonnecrotizing epithelioid cell granuloma (unrelated to infection or crypt rupture)
- True small intestinal involvement unrelated to backwash ileitis
- Perianal disease unrelated to other causes
- Superficial (ulcerative colitis-like) Crohn's disease: nonnecrotizing epithelioid cell granulomas (unassociated with infection or crypt rupture) in the mucosa or lymph node of a specimen that is otherwise suggestive of ulcerative colitis (i.e. mucosa based chronic active colitis); a diagnosis of IBD, indeterminate type is preferred by some authors in these cases but an explanation as to the reason of the uncertainty should be included
- Dysplasia / carcinoma: same as IBD (Inflamm Bowel Dis 2009;15:1076)
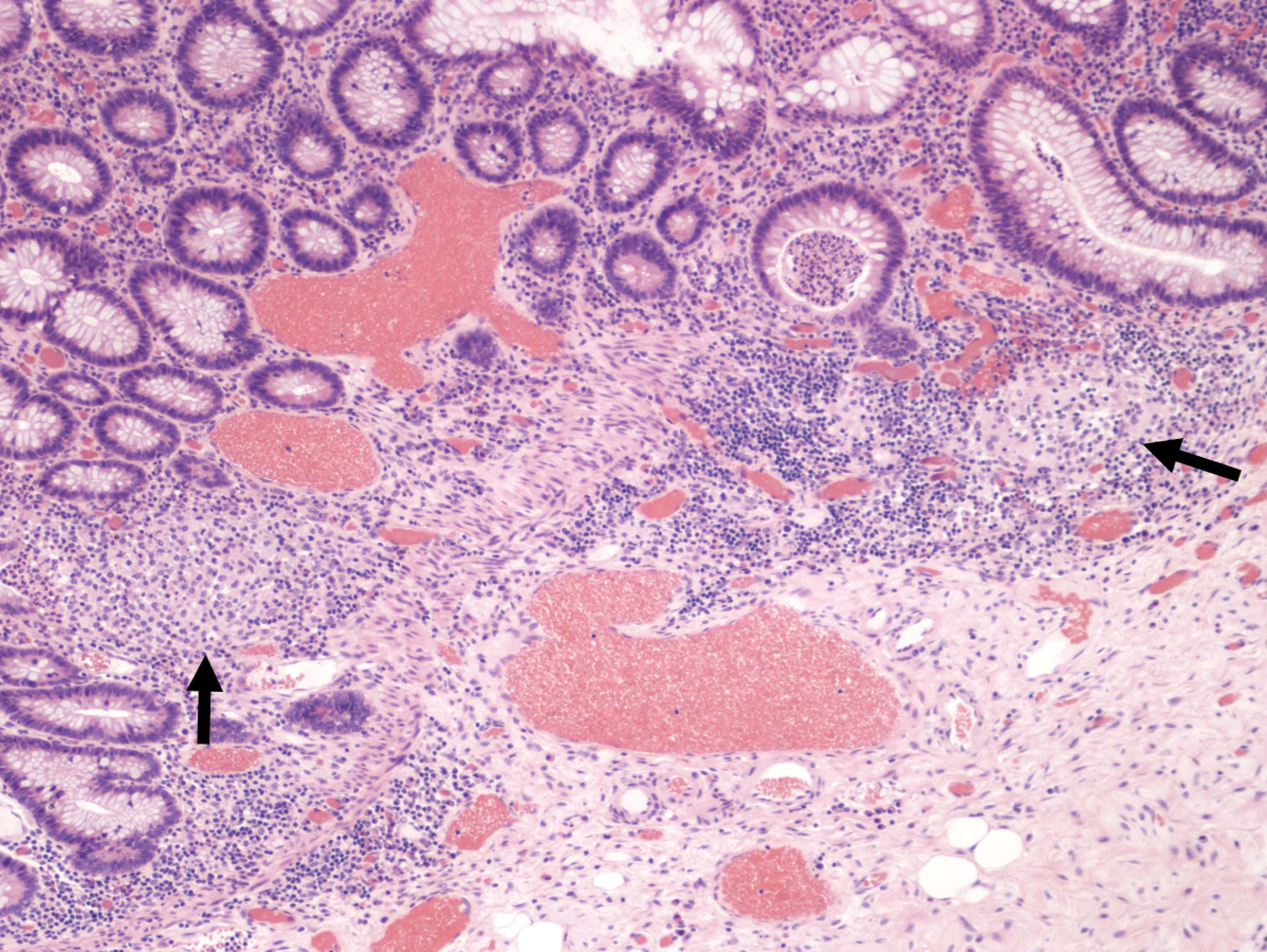
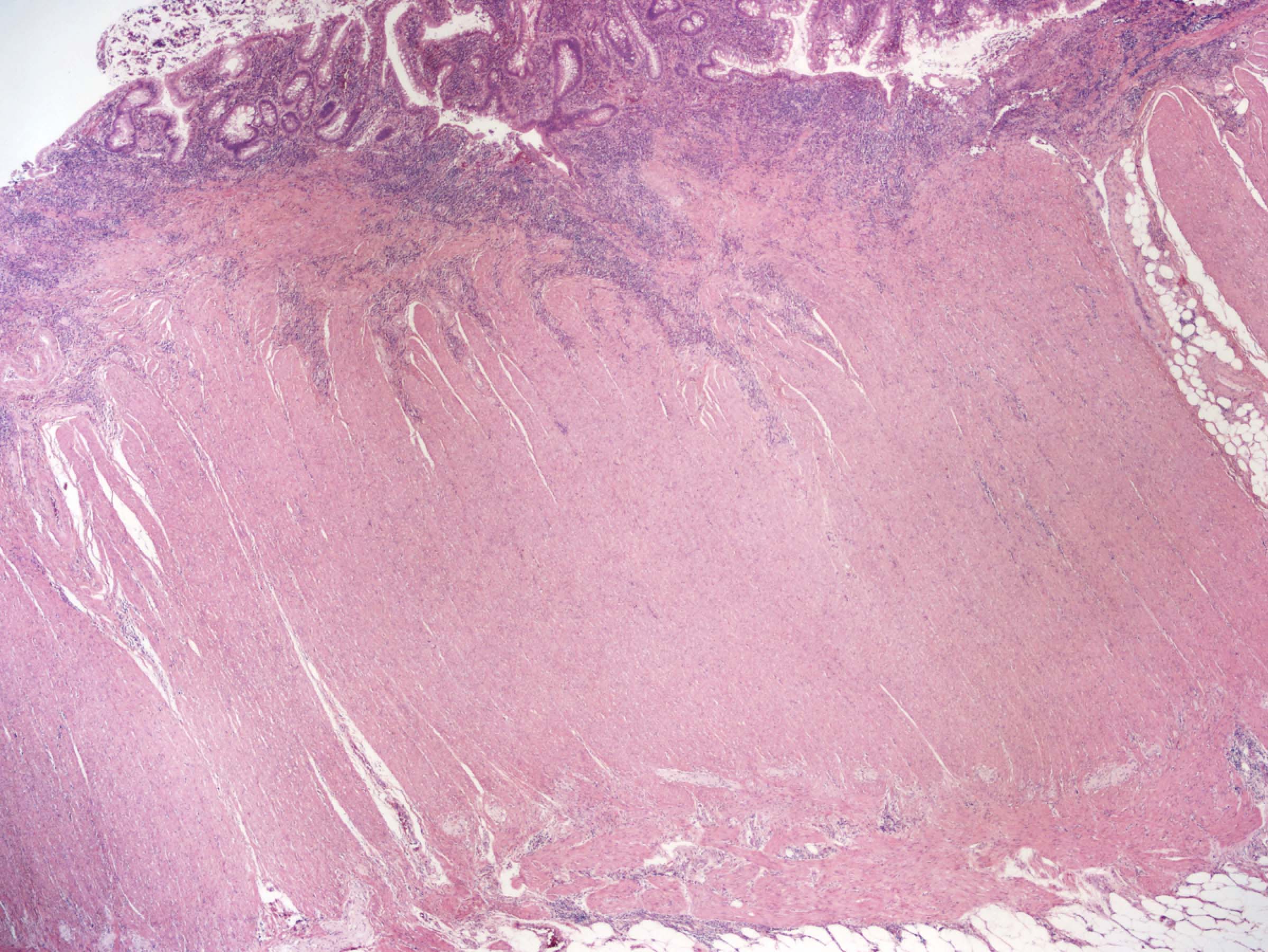
Microscopic (histologic) images
Contributed by John D. Paulsen, M.D. and Alexandros D. Polydorides, M.D., Ph.D.
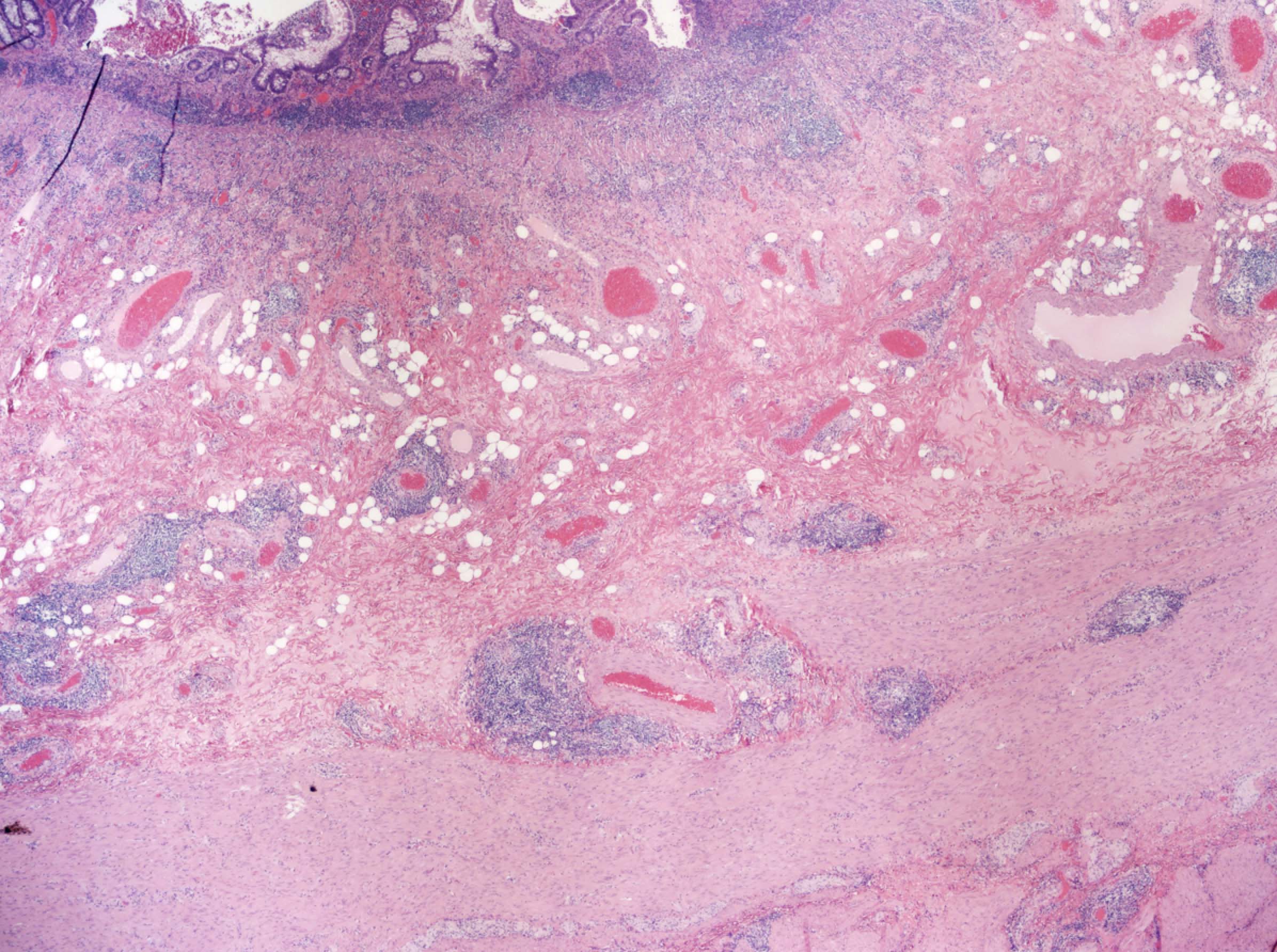
Transmural chronic inflammation
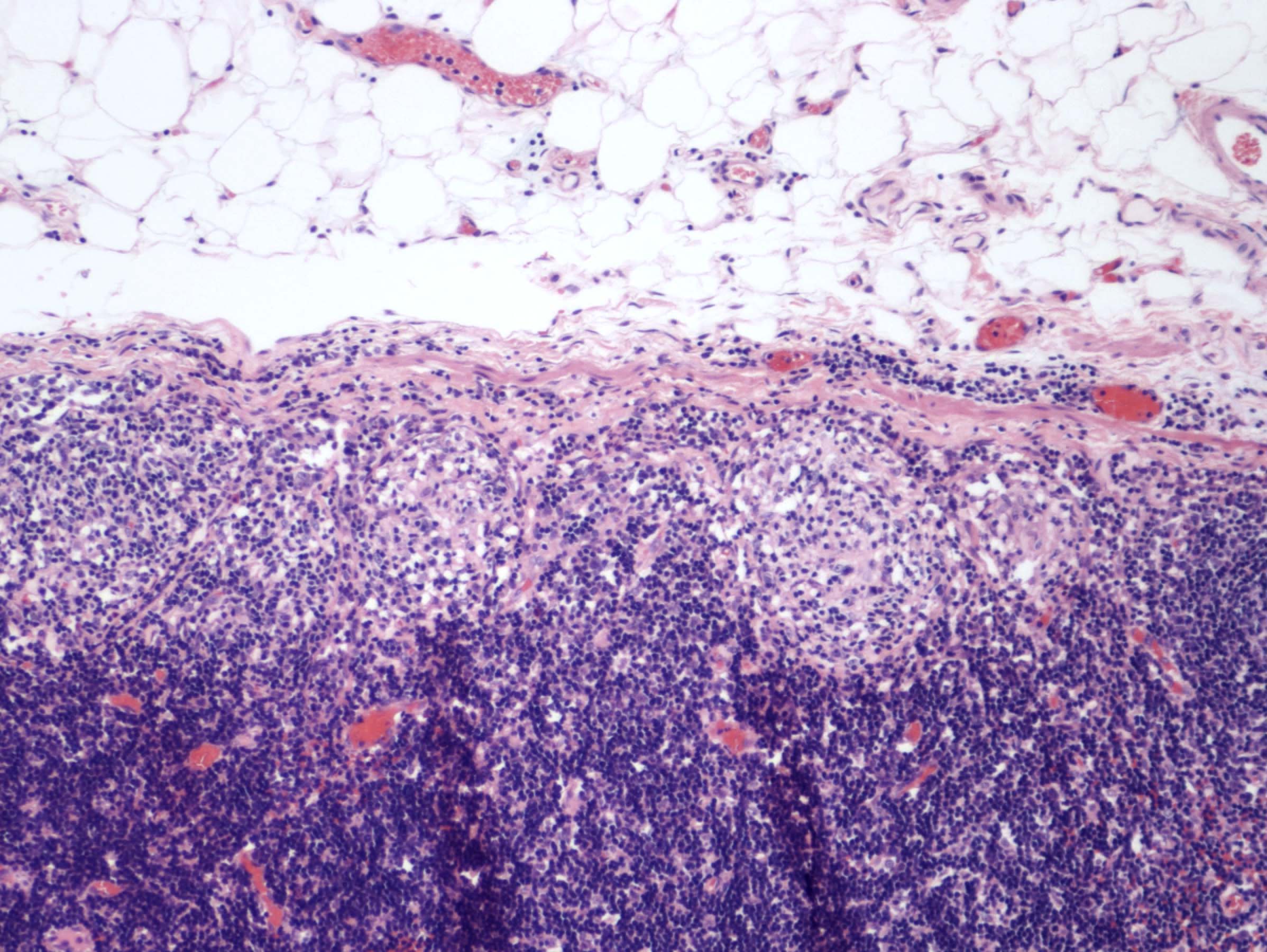
Granuloma, pericolonic lymph node
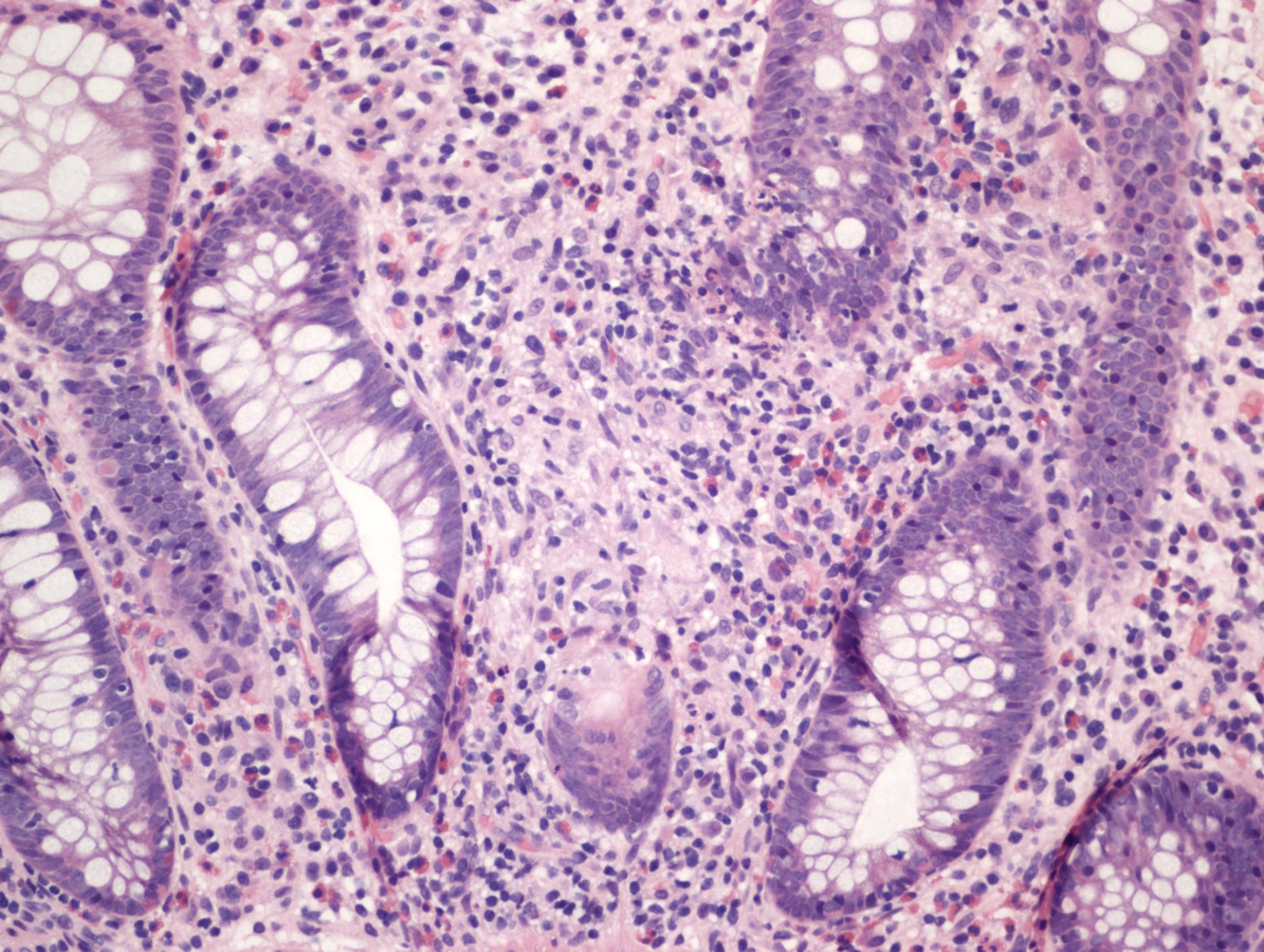
Mimic: cryptolytic granuloma, ulcerative colitis
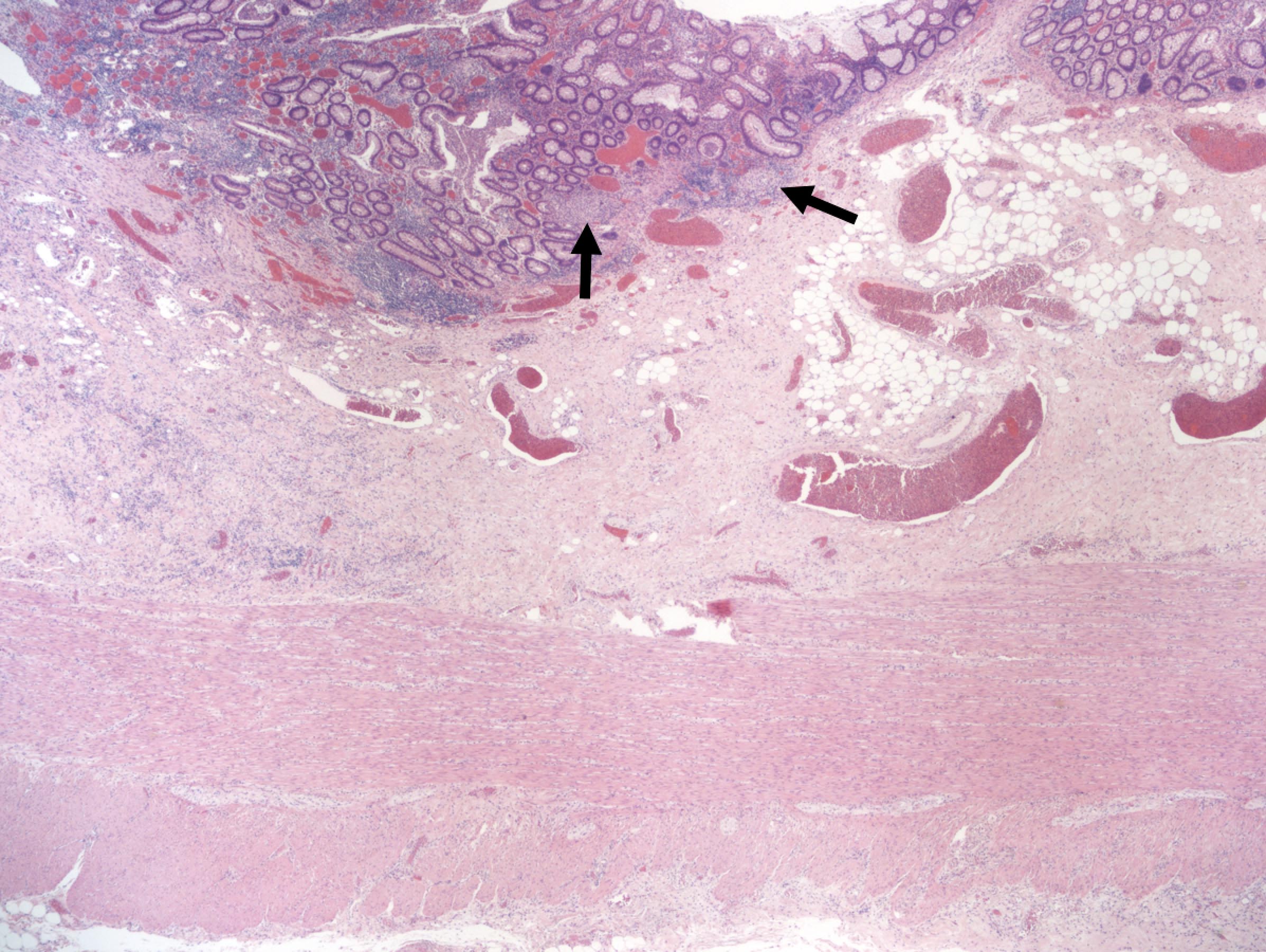
Mimic: superficial (ulcerative colitis-like) Crohn's disease
Mimic: fulminant ulcerative colitis
Sample pathology report
- Terminal ileum, cecum, appendix and colon, total abdominal colectomy:
- Severely active chronic colitis with continuous retrograde extension to the hepatic flexure (see comment)
- Comment: The inflammation is generally mucosa based with extensive ulceration and associated transmural disease but diagnostic characteristics of Crohn's disease are lacking. Rectal sparing has been described clinically but should be confirmed histologically, if possible. The ileal segment and appendix are unremarkable.
- The findings are best classified as inflammatory bowel disease, indeterminate type.
Differential diagnosis
- Ulcerative colitis:
- Diffuse mucosa based / superficial involvement of the colorectum
- Well recognized patterns of ulcerative colitis with Crohn's-like features: cecal patch, cryptolytic granulomas, fulminant ulcerative colitis with transmural inflammation in areas of ulceration
- Crohn's disease:
- Transmural lymphoid aggregates in areas of nonulcerated mucosa, nonnecrotizing epithelioid cell granuloma (not associated with ruptured crypts), fissuring ulcers
- Ischemic colitis:
- Involvement of watershed areas (e.g. splenic flexure) mostly
- Surface active inflammation / necrosis
- Hyalinized lamina propria
- Withered / shrunken crypts
- Diversion colitis:
- Prominent mucosa / submucosal follicular lymphoid hyperplasia
- History of fecal stream diversion
- Segmental colitis associated with diverticular disease (SCAD):
- Limited to areas of the colon with known diverticulosis
Practice question #1
A 26 year old woman with no significant past medical history is found to have severe colitis and undergoes total abdominal colectomy. The gross examination of the resection specimen reveals a predominantly left sided colitis with discontinuous involvement of the cecal and periappendiceal mucosa, as shown in the image above. Microscopic evaluation demonstrates a mucosa based, active chronic colitis without evidence of transmural inflammation. Several nonnecrotizing epithelioid cell granuloma associated with ruptured crypts are identified. Which of the following is true regarding the patient’s pathologic diagnosis?
- A diagnosis of Crohn's disease is warranted due to the presence of discontinuous colitis
- The findings are best classified as inflammatory bowel disease (IBD), type indeterminate because the specimen shows overlapping features of Crohn's disease and ulcerative colitis
- The findings are consistent with a recognized variant of ulcerative colitis
- The presence of nonnecrotizing epithelioid cell granuloma precludes a diagnosis of ulcerative colitis in this case
Practice answer #1
C. The findings are consistent with a recognized variant of ulcerative colitis
The photograph shows a total abdominal colectomy specimen with a predominantly left sided colitis and discontinuous involvement of the cecal or periappendiceal mucosa. The gross and microscopic findings are convincing for a diagnosis of ulcerative colitis. It is well documented that patients with left sided ulcerative colitis may have discontinuous involvement of the periappendiceal or cecal mucosa, known as a cecal patch. A diagnosis of IBD, indeterminate type should be avoided when dealing with well recognized variants of IBD, such as ulcerative colitis with cecal patch and superficial (ulcerative colitis-like) Crohn's disease. Nonnecrotizing epithelioid cell granulomas associated with ruptured crypts (cryptolytic granulomas) are known to occur in cases of ulcerative colitis and often result in diagnostic difficulties; however, this finding should not preclude a diagnosis of ulcerative colitis.
Comment Here
Reference: Inflammatory bowel disease, indeterminate type
The photograph shows a total abdominal colectomy specimen with a predominantly left sided colitis and discontinuous involvement of the cecal or periappendiceal mucosa. The gross and microscopic findings are convincing for a diagnosis of ulcerative colitis. It is well documented that patients with left sided ulcerative colitis may have discontinuous involvement of the periappendiceal or cecal mucosa, known as a cecal patch. A diagnosis of IBD, indeterminate type should be avoided when dealing with well recognized variants of IBD, such as ulcerative colitis with cecal patch and superficial (ulcerative colitis-like) Crohn's disease. Nonnecrotizing epithelioid cell granulomas associated with ruptured crypts (cryptolytic granulomas) are known to occur in cases of ulcerative colitis and often result in diagnostic difficulties; however, this finding should not preclude a diagnosis of ulcerative colitis.
Comment Here
Reference: Inflammatory bowel disease, indeterminate type
