

Fallopian tubes & broad ligament
Fallopian tube nontumor
Ectopic / tubal pregnancy
Editorial Board Member: Ricardo R. Lastra, M.D.
Deputy Editor-in-Chief: Jennifer A. Bennett, M.D.


Last author update: 28 October 2021
Last staff update: 28 October 2021
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Ectopic tubal pregnancy [TI]


Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2 | Board review style question #3 | Board review style answer #3Cite this page: Sorelle N, Chang R, Chen H. Ectopic / tubal pregnancy. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/fallopiantubesectopicpregnancy.html. Accessed May 12th, 2024.
Definition / general
- Extrauterine implantation of a fertilized egg
Essential features
- Extrauterine implantation of a fertilized egg
- > 95% occur in the fallopian tube
- Diagnosis based on visualization of an extrauterine gestational sac by transvaginal ultrasound (TVUS) or histologic confirmation
ICD coding
Epidemiology
- Approximately 2% of all reported pregnancies in the United States are ectopic (MMWR Morb Mortal Wkly Rep 1995;44:46, Fertil Steril 2014;102:1671, Obstet Gynecol 2010;115:495)
- 2.7% of pregnancy related mortalities attributed to ruptured ectopic (Obstet Gynecol 2017;130:366)
- Diagnosis increases with age: 0.29% (15 - 19 years old), ~0.5% (20 - 24 years old), ~0.58% (25 - 29 years old), ~0.7% (30 - 34 years old) and ~0.89% (35 - 44 years old) (South Med J 2017;110:18)
Sites
- Fallopian tube accounts for 95.5% of extrauterine implantation sites: 2.4% interstitial, 11.1% fimbrial, 12.0% isthmic and 70% ampullary (Hum Reprod 2002;17:3224)
- 4.5% are extratubal: 3.2% ovarian and 1.3% abdominal (Hum Reprod 2002;17:3224)
- May implant at any place on the abdominal viscera or peritoneal surface (Radiographics 2015;35:946):
- Cervix (J Emerg Med 2019;56:e123)
- Liver (Pathology 2018;50:478)
- Spleen (BMJ Case Rep 2016;2016:bcr2016218291)
- Prior cesarean scars (Clin Imaging 2020;66:26)
Pathophysiology
- 4 possible mechanisms of ectopic implantation (Sex Transm Infect 2020;96:322):
- Anatomic obstruction preventing passage of the zygote
- Abnormal conceptus
- Tubal motility abnormalities
- Zygote transperitoneal migration
Etiology
- Pelvic inflammatory disease
- Disruption of tubal anatomy caused by infection is the most likely cause; inflammation of the tube is present in up to 90% of tubal pregnancies, which is 6x more common than in normal tubes
- Cigarette smoking
- Prior fallopian tube pathology
- Infertility
- Intrauterine device
- Previous fallopian tube surgery
- Previous ectopic pregnancy
- Approximately half of ectopic pregnancy patients do not have any identifiable risk factors
- References: Clin Obstet Gynecol 2012;55:376, Fertil Steril 1996;65:1093, Obstet Gynecol 2018;131:e91
Clinical features
- Most common clinical presentationis first trimester vaginal bleeding or abdominal pain
- Symptoms usually appear 6 - 8 weeks after the patient’s last menstrual period but may occur even later, particularly if the pregnancy occurs outside of the fallopian tube
- No confirmed intrauterine pregnancy
Diagnosis
- Positive pregnancy test and visualization of an extrauterine gestational sac, with or without an embryo on transvaginal ultrasound
- Visualization at surgery with histologic confirmation
Laboratory
- Positive beta hCG
Radiology description
- Extrauterine gestational sac, with or without an embryo on transvaginal ultrasound
Radiology images
Contributed by Hao Chen, M.D., Ph.D.
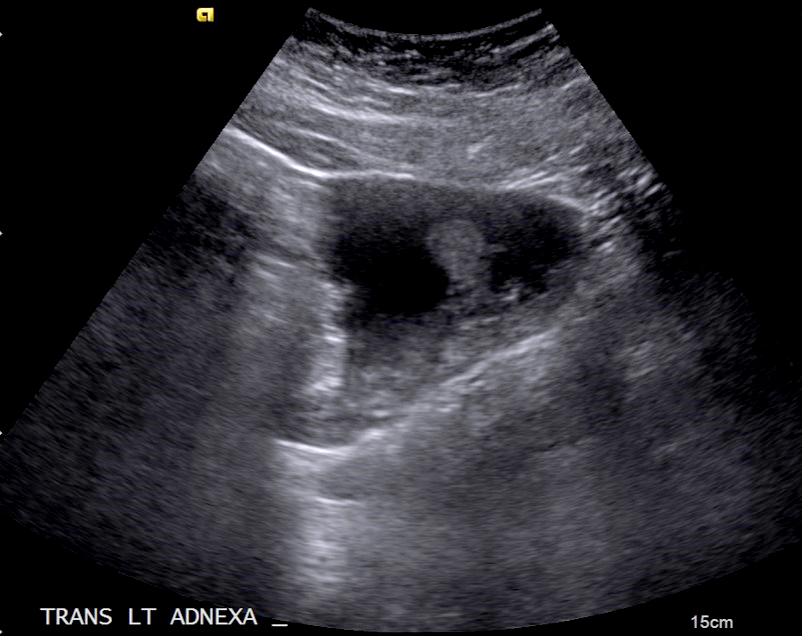
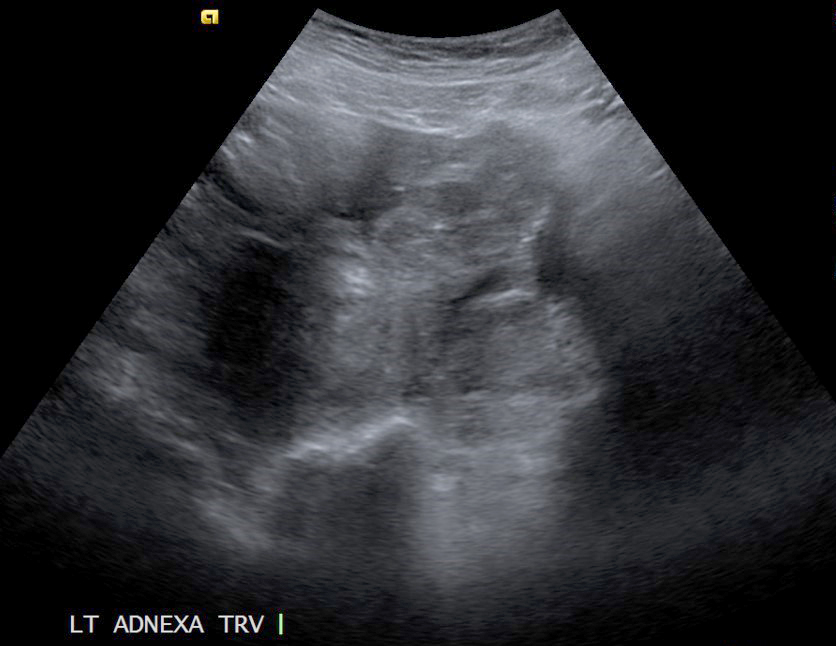
Left adnexal mass
Prognostic factors
- Significant risk of morbidity and mortality if not promptly recognized and treated
- Patients with earlier ectopic pregnancies and relatively modest beta hCG levels are more likely to have successful treatment with single dose methotrexate therapy (Clin Obstet Gynecol 2012;55:376)
- Following methotrexate therapy, patients not exhibiting at least a 15% decrease in beta hCG from day 4 - 7 are more likely to experience treatment failure (Reprod Biomed Online 2017;34:383)
Case reports
- 29 year old woman with vaginal bleeding and discharge (Radiol Case Rep 2019;14:354)
- 30 year old woman with abdominal ectopic pregnancy after in vitro fertilization and single embryo transfer (Reprod Biol Endocrinol 2016;14:69)
- 38 year old woman with acute onset of lower abdominal pain associated with a history of amenorrhea (Cureus 2020;12:e10993)
Treatment
- Surgical management (typically salpingectomy or salpingotomy) for hemodynamically unstable patients
- Methotrexate may be administrated for hemodynamically stable patients (Clin Obstet Gynecol 2012;55:376)
Gross description
- Dilated tube with distended wall, with or without rupture
- Lumen contains blood clot, embryo, chorionic villi
Gross images
Contributed by Hao Chen, M.D., Ph.D. and AFIP

Placenta and fetus
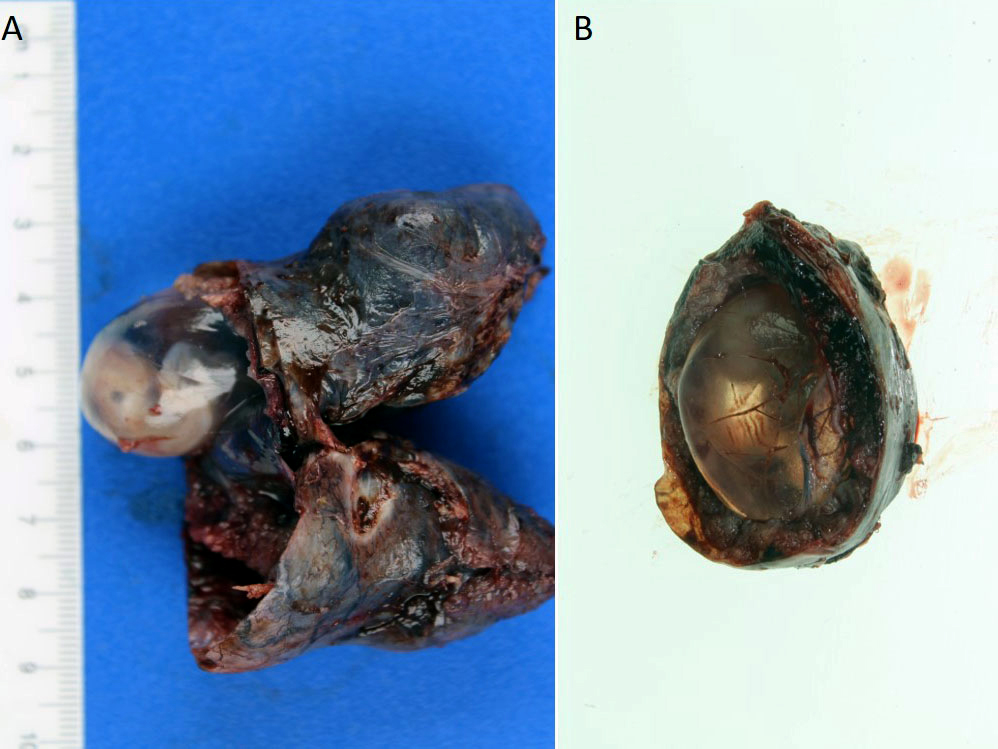
Gestational sac and embryo
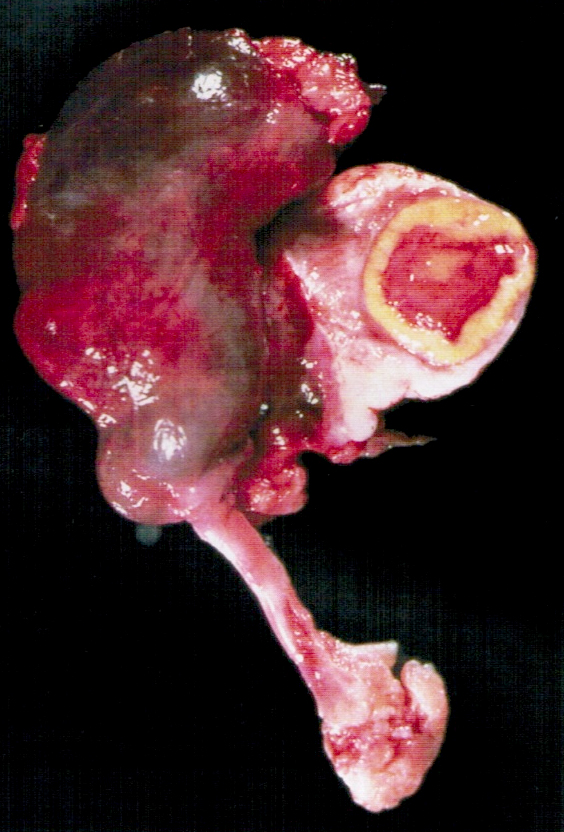

Ectopic pregnancy
Images hosted on other servers

Hemorrhage and placental tissue with fetal part

Rupture and hemoperitoneum
Microscopic (histologic) description
- Presence of extrauterine chorionic villi or extravillous trophoblast is needed for diagnosis
- Fetal tissue may be present
- Endometrial stromal decidualization in isolation is not diagnostic of ectopic pregnancy
- Mesothelial reactive changes, often reactive mesothelial proliferation, may be present (on the surface of the fallopian tube or the closest peritoneum to the site of the ectopic pregnancy); of note, the exaggerated cytological changes and mesothelial proliferation should not be confused with atypical mesothelial proliferation
Microscopic (histologic) images
Contributed by Hao Chen, M.D., Ph.D.
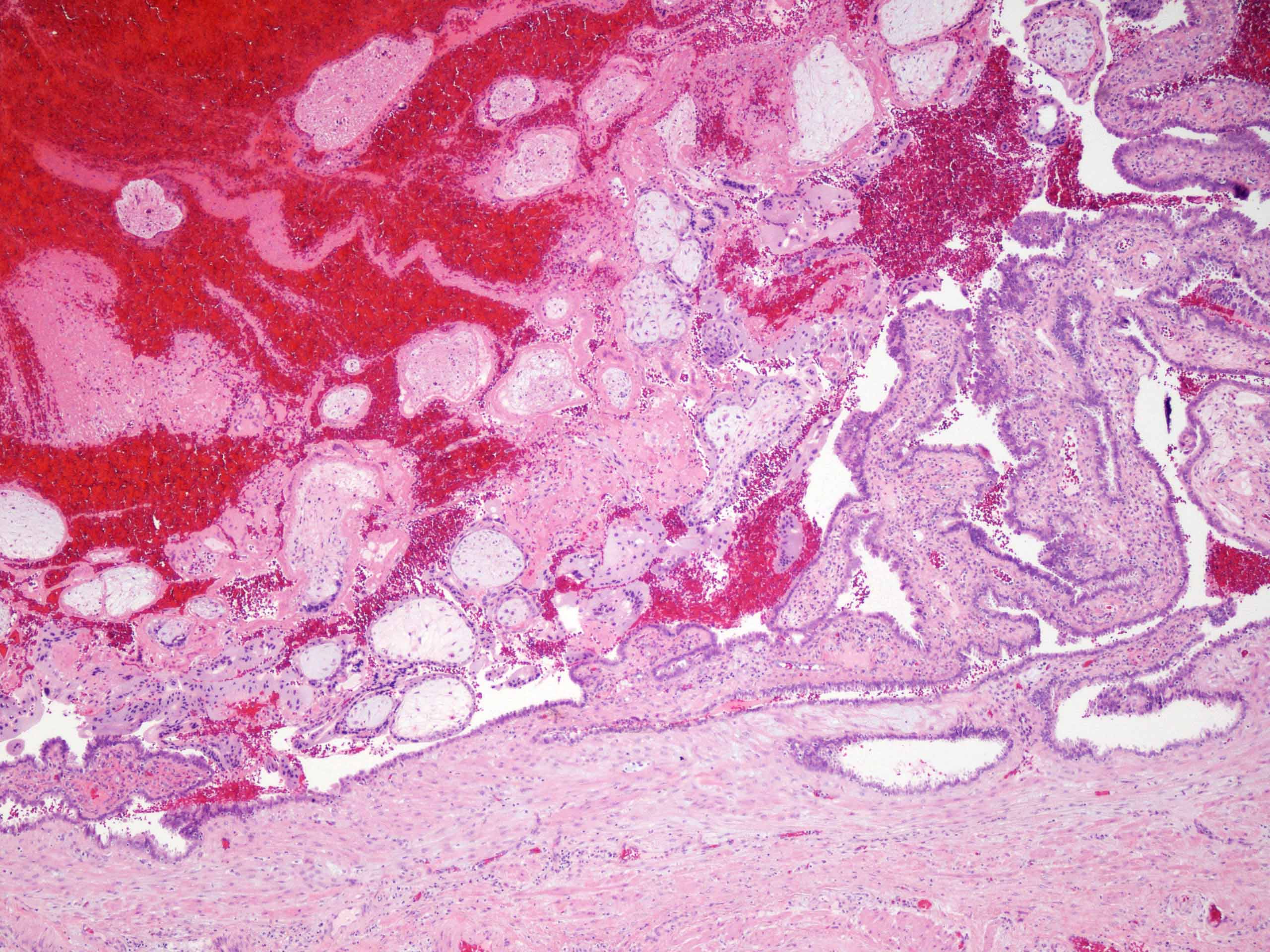
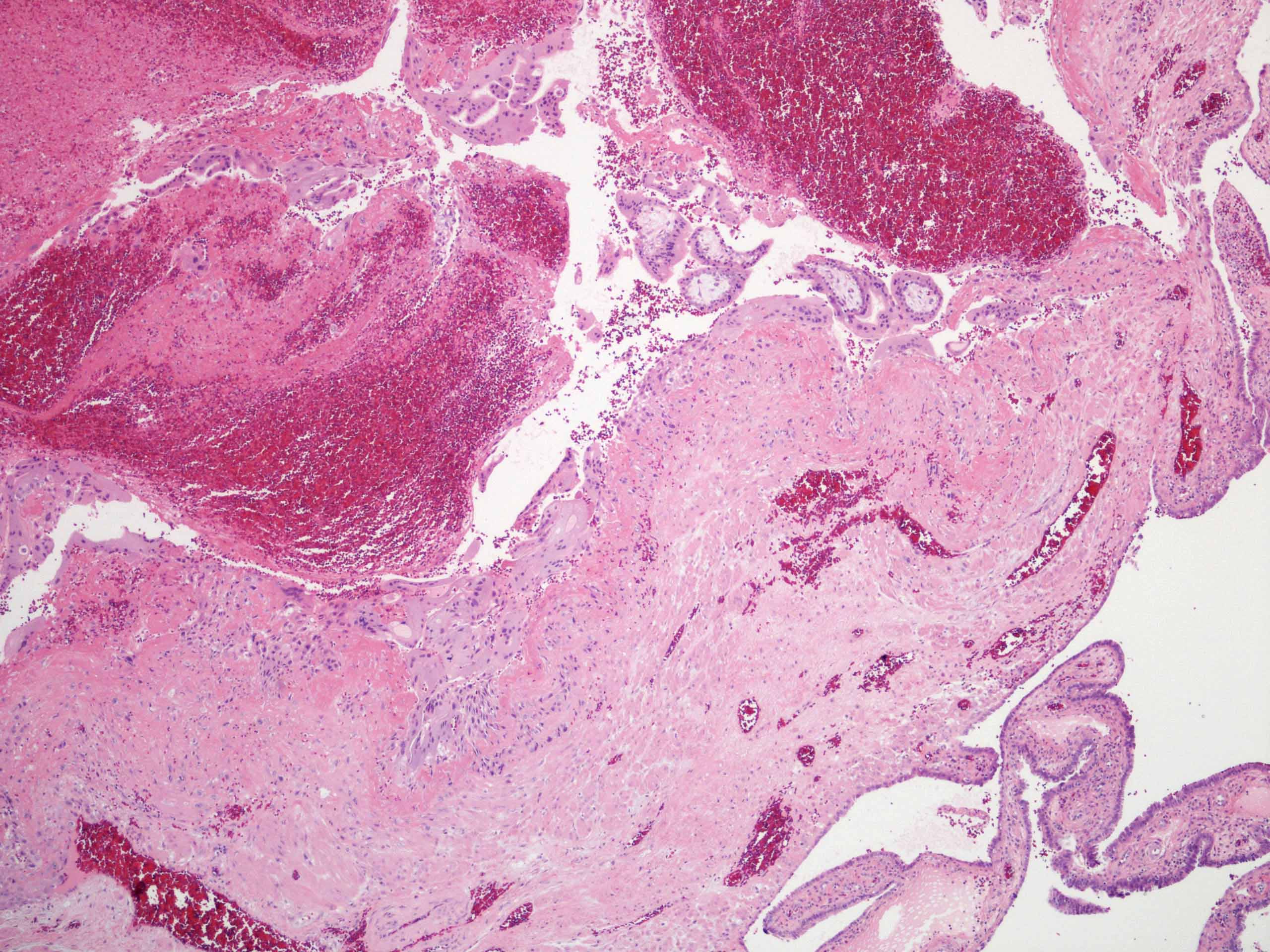
Intraluminal chorionic villi
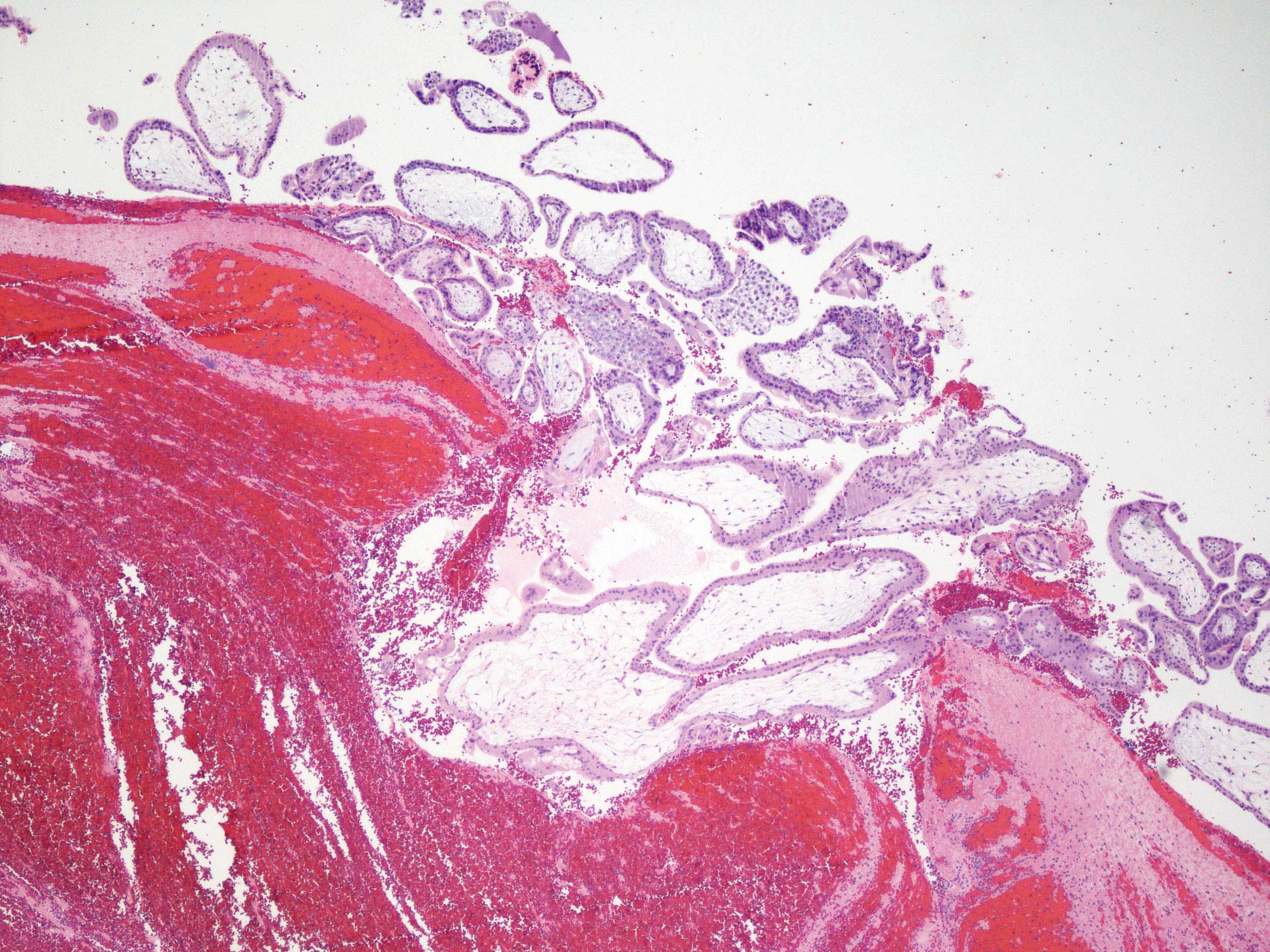
Chorionic villi and blood
Sample pathology report
- Fallopian tube, salpingectomy:
- Fallopian tube with intraluminal immature chorionic villi, consistent with ectopic (tubal) pregnancy
Differential diagnosis
- Spontaneous abortion:
- Identification of product of conceptions in expelled uterine tissue or endometrial curettage tissue
- Lack of evidence of extrauterine gestational sac / embryo by either transvaginal ultrasound or histological confirmation
Board review style question #1
The most common site of ectopic tubal pregnancy is
- Ampulla
- Fimbria
- Interstitial
- Isthmic
Board review style answer #1
A. Ampulla. 70% of tubal pregnancies are ampullary, followed by isthmic (12.0%), fimbrial (11%) and interstitial (2.4%).
Comment Here
Reference: Ectopic / tubal pregnancy
Comment Here
Reference: Ectopic / tubal pregnancy
Board review style question #2
The most common cause of ectopic pregnancy is
- Idiopathic
- Infertility
- Intrauterine device
- Pelvic inflammatory disease
Board review style answer #2
A. Idiopathic. Approximately half of ectopic pregnancy patients do not have any identifiable risk factors.
Comment Here
Reference: Ectopic / tubal pregnancy
Comment Here
Reference: Ectopic / tubal pregnancy
Board review style question #3
A 28 year old woman presented with acute onset abdominal pain and vaginal bleeding. Pregnancy test was positive. Transvaginal ultrasound showed left adnexal mass. Left salpingectomy was performed. The histological findings were as showed in the above image. The diagnosis is
- Chronic salpingitis
- Ectopic tubal pregnancy
- Tubo-ovarian abscess
- Tubo-ovarian torsion
Board review style answer #3
B. Ectopic tubal pregnancy. Intraluminal chorionic villi, implantation site (upper left). Of note, tubal epithelia is located at lower right corner.
Comment Here
Reference: Ectopic / tubal pregnancy
Comment Here
Reference: Ectopic / tubal pregnancy
