
27 May 2005 - Case #8
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Hind Warzecha (formerly Nassar), Wayne State University Department of Pathology, Detroit, Michigan, USA.
Case #8
Clinical history:
A 52 year old woman had a breast mass, which was excised. She also had two positive axillary lymph nodes.
Microscopic images:
What is your diagnosis?
Diagnosis: Secretory carcinoma of the breast
Discussion:
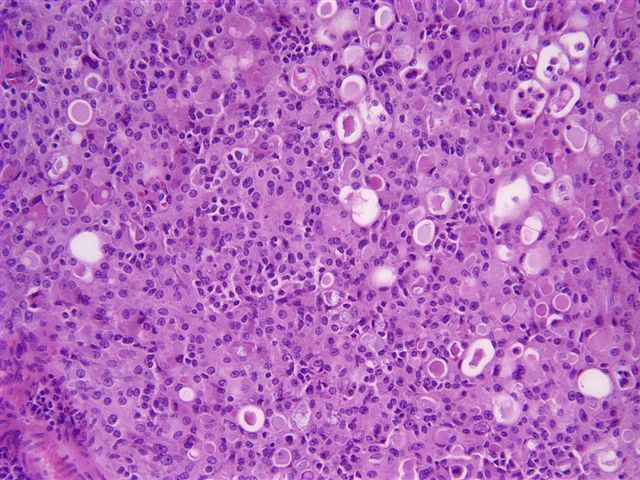
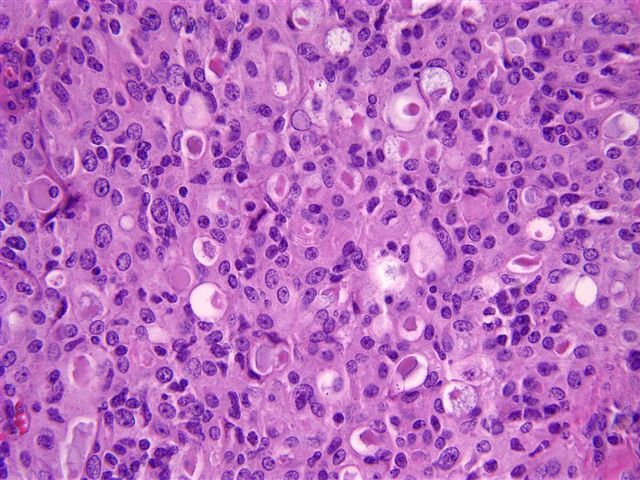
Secretory carcinoma of the breast is also known as juvenile carcinoma. It is a rare subtype of breast carcinoma in adults but is the most common form of breast carcinoma in children. The tumors are usually small and well circumscribed. Tumors are composed of tubuloalveolar or focal papillary formations of relatively bland cells with abundant pale to eosinophilic cytoplasm, often vacuolated. Nucleoli are frequently prominent. The most striking feature is the luminal eosinophilic secretions, which are PAS+ and diastase resistant (image). Mitotic figures are rare. It is often difficult to determine how much of the tumor represents in situ versus invasive disease. The tumors have pushing margins and often central hyalinization.
Tumor cells are immunoreactive for S100 and alpha lactalbumin with variable staining for GCDFP-15 and CEA. They are often negative for estrogen and progesterone receptors. Electron microscopy shows numerous membrane bound, intracytoplasmic secretory vacuoles.
Secretory carcinoma is important to recognize as a subtype because of its excellent prognosis, with a 5 year survival approaching 100% in children. In women age 30 years or older, the prognosis is less favorable, due to late local recurrence and nodal metastases but distant metastases and death due to disease are still rare. These tumors also differ from the usual invasive ductal carcinoma due to expression of a chimeric tyrosine kinase, encoded by a ETV6::NTRK3 fusion gene.
References: Hum Pathol 2003;34:1299, Semin Cancer Biol 2005;15:215, Genes Chromosomes Cancer 2004;40:152
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Hind Warzecha (formerly Nassar), Wayne State University Department of Pathology, Detroit, Michigan, USA.
Website news:
(1) This week's case is sponsored by our Management Page, with a link on our Home page under Clinical Pathology topics (or click here). The Management page presents information on business aspects of pathology practice, written by the experts, with new topics added monthly.
Visit and follow our Blog to see recent updates to the website.
(1) This week's case is sponsored by our Management Page, with a link on our Home page under Clinical Pathology topics (or click here). The Management page presents information on business aspects of pathology practice, written by the experts, with new topics added monthly.
Visit and follow our Blog to see recent updates to the website.
Case #8
Clinical history:
A 52 year old woman had a breast mass, which was excised. She also had two positive axillary lymph nodes.
Microscopic images:
Medium power
High power
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Secretory carcinoma of the breast
Discussion:
Secretory carcinoma of the breast is also known as juvenile carcinoma. It is a rare subtype of breast carcinoma in adults but is the most common form of breast carcinoma in children. The tumors are usually small and well circumscribed. Tumors are composed of tubuloalveolar or focal papillary formations of relatively bland cells with abundant pale to eosinophilic cytoplasm, often vacuolated. Nucleoli are frequently prominent. The most striking feature is the luminal eosinophilic secretions, which are PAS+ and diastase resistant (image). Mitotic figures are rare. It is often difficult to determine how much of the tumor represents in situ versus invasive disease. The tumors have pushing margins and often central hyalinization.
Tumor cells are immunoreactive for S100 and alpha lactalbumin with variable staining for GCDFP-15 and CEA. They are often negative for estrogen and progesterone receptors. Electron microscopy shows numerous membrane bound, intracytoplasmic secretory vacuoles.
Secretory carcinoma is important to recognize as a subtype because of its excellent prognosis, with a 5 year survival approaching 100% in children. In women age 30 years or older, the prognosis is less favorable, due to late local recurrence and nodal metastases but distant metastases and death due to disease are still rare. These tumors also differ from the usual invasive ductal carcinoma due to expression of a chimeric tyrosine kinase, encoded by a ETV6::NTRK3 fusion gene.
References: Hum Pathol 2003;34:1299, Semin Cancer Biol 2005;15:215, Genes Chromosomes Cancer 2004;40:152
