
11 March 2015 - Case of the Week #345
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Ankur Sangoi, El Camino Hospital, California (USA), for contributing this case.
Advertisement
Case #345
Clinical history:
A 49 year old woman had a hysterectomy for leiomyomas (fibroids) of the uterus.
Microscopic images:

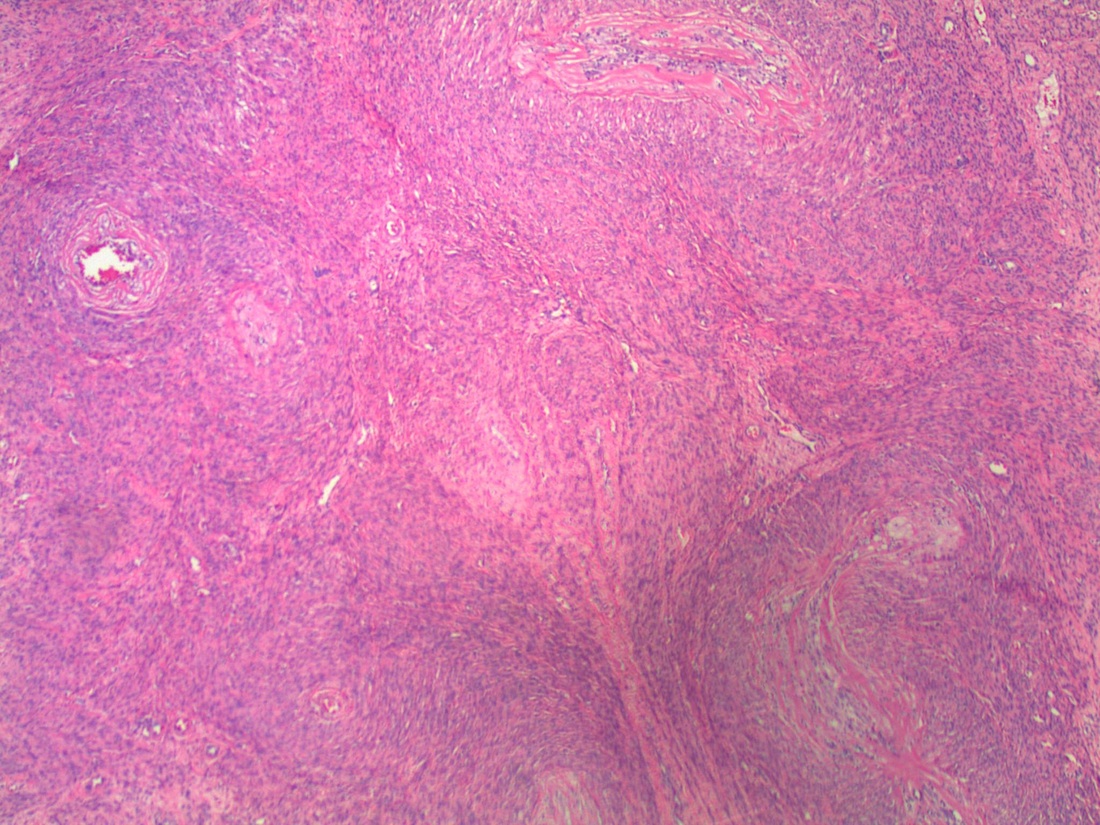
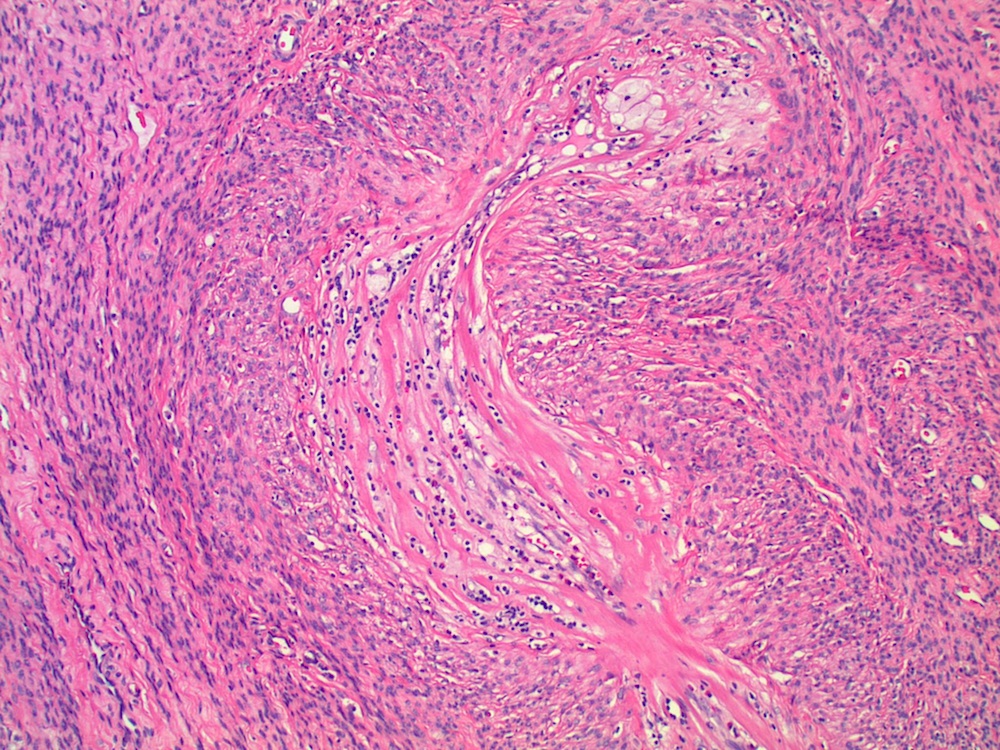
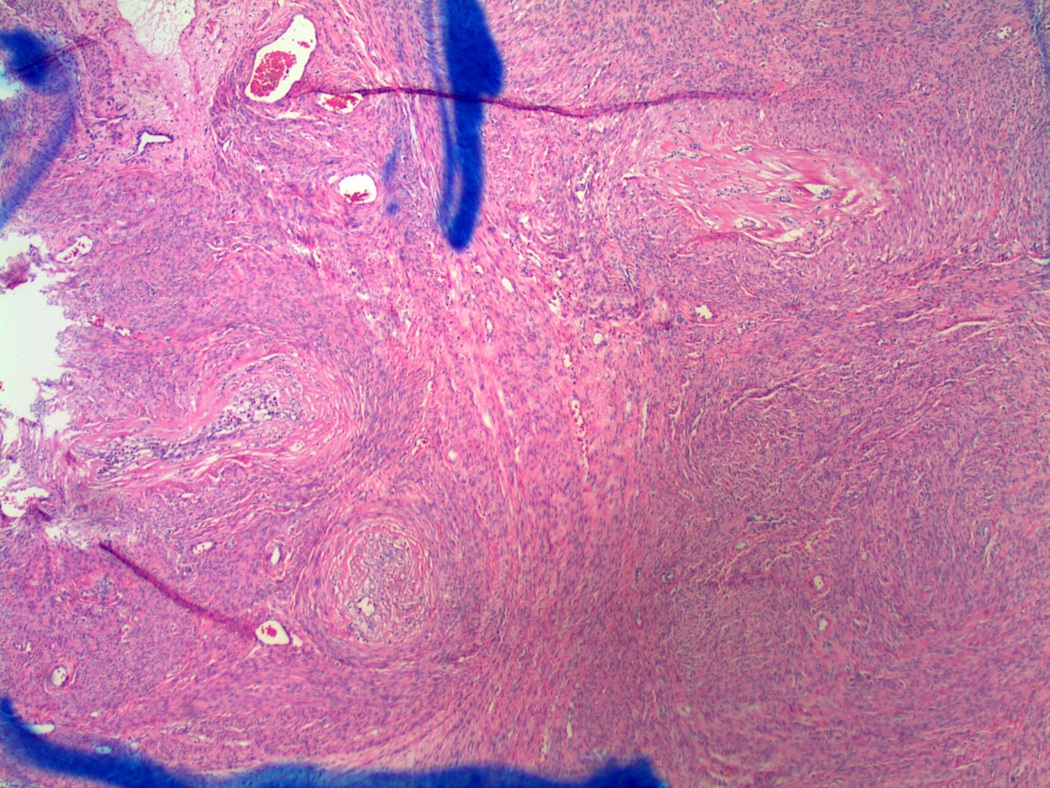

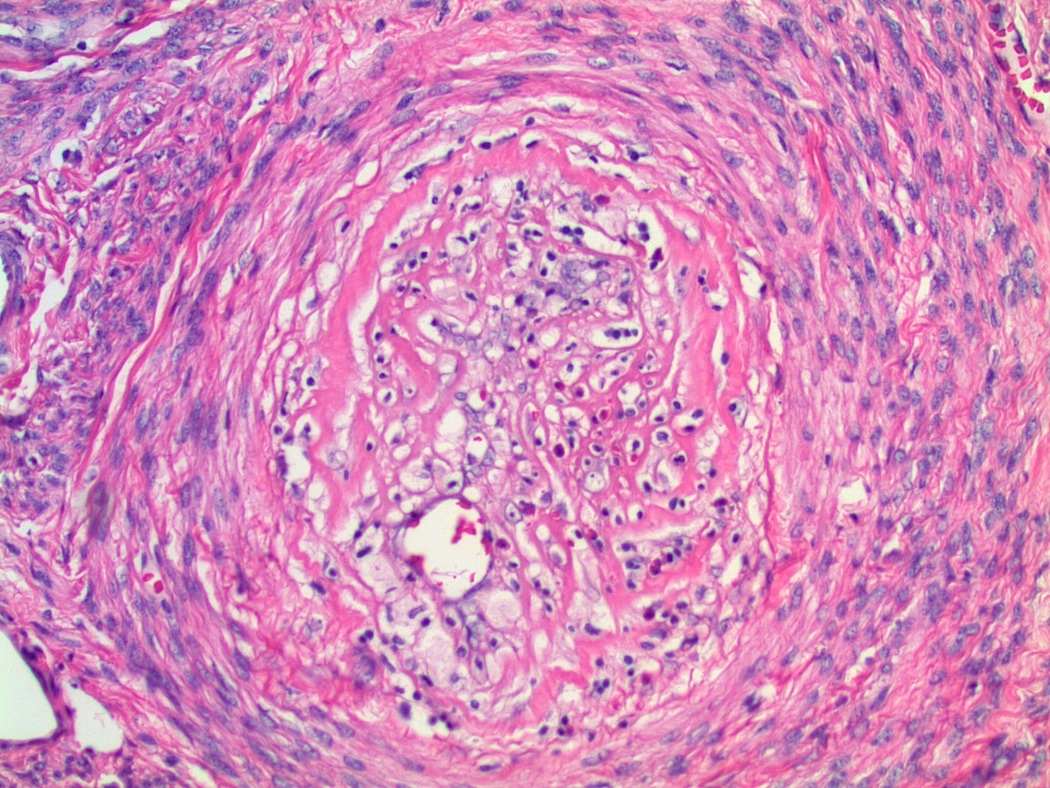

What is your diagnosis?
Diagnosis: Leiomyoma with vasculitis secondary to Lupron
Discussion:
Since the 1980's, gonadotropin releasing hormone (GnRH) agonists such as Leuprorelin (Lupron®) have been used to treat uterine leiomyoma, leading to shrinkage of the leiomyoma and uterus, which facilitates easier surgical treatment (vaginal instead of abdominal hysterectomy, myomectomy instead of hysterectomy) (Wikipedia: Leuprorelin [Accessed 13 November 2023]). The mechanism is initial GnRH stimulation of pituitary LH and FSH production, followed by decreased production as the pituitary becomes desensitized to GnRH. This leads to reduced estrogen production, associated with reduction in size of the estrogen dependent leiomyoma (Int J Surg Pathol 2003;11:339, Int J Gynecol Pathol 1995;14:235). GnRH agonists are used only temporarily, because their anti-estrogen side effects include menopausal symptoms and bone loss, and upon withdrawal, the leiomyomas rapidly regrow.
Histologically, there is often initially edema and necrosis, followed by hyalinization and lymphocytic infiltrate (B and T cells). In this case, there was a prominent vasculitis. The patient had no history of a prior vasculitis and at follow up 3 years later, there was no evidence of vasculitis.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Ankur Sangoi, El Camino Hospital, California (USA), for contributing this case.

- Sternberg's Diagnostic Surgical Pathology (2015) by Stacey Mills, Joel Greenson, Jason Hornick, Teri Longacre and Victor Reuter. Visually stunning and thoroughly up to date, the sixth edition of Sternberg's Diagnostic Surgical Pathology continues to set the standard for differential diagnosis of the surgical specimen. Offering the latest information on all currently known diseases, this classic two-volume reference presents advanced diagnostic techniques from a virtual "who's who" of experts in the field - pathologists who provide authoritative guidance on the diagnostic evaluation of every type of specimen from every anatomic site. No matter what your level of training or experience, keeping Sternberg's near your microscope is the next best thing to a personal consultation with a trusted colleague.
- Sternberg's Diagnostic Surgical Pathology Review (2015) by Pier Luigi Di Patre and Darryl Carter. Based on the sixth edition of Sternberg's Diagnostic Surgical Pathology, this multiple choice question and answer resource covers all aspects of Surgical Pathology and is an ideal review tool for board preparation, recertification exams or just brushing up. Now significantly revised, it includes more than 1,000 questions and answers that emphasize differential diagnostic aspects of problem solving, accompanied by more than 600 full-color illustrations.
For more information, visit our New Books page.
Website news:
(1) Our Feature page for March is Tissue Processors / Other Histology and highlights our advertiser Milestone Medical. It also contains an original short article, "Tissue Histology: Preserving Information from Molecules", by Jaleh Mansouri, M.D.
(2) Thanks to you, we set record average daily traffic of 21,430 visits per day in February! As always, please let us know how we can be more useful to you.
Visit and follow our Blog to see recent updates to the website.
(1) Our Feature page for March is Tissue Processors / Other Histology and highlights our advertiser Milestone Medical. It also contains an original short article, "Tissue Histology: Preserving Information from Molecules", by Jaleh Mansouri, M.D.
(2) Thanks to you, we set record average daily traffic of 21,430 visits per day in February! As always, please let us know how we can be more useful to you.
Visit and follow our Blog to see recent updates to the website.
Case #345
Clinical history:
A 49 year old woman had a hysterectomy for leiomyomas (fibroids) of the uterus.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Leiomyoma with vasculitis secondary to Lupron
Discussion:
Since the 1980's, gonadotropin releasing hormone (GnRH) agonists such as Leuprorelin (Lupron®) have been used to treat uterine leiomyoma, leading to shrinkage of the leiomyoma and uterus, which facilitates easier surgical treatment (vaginal instead of abdominal hysterectomy, myomectomy instead of hysterectomy) (Wikipedia: Leuprorelin [Accessed 13 November 2023]). The mechanism is initial GnRH stimulation of pituitary LH and FSH production, followed by decreased production as the pituitary becomes desensitized to GnRH. This leads to reduced estrogen production, associated with reduction in size of the estrogen dependent leiomyoma (Int J Surg Pathol 2003;11:339, Int J Gynecol Pathol 1995;14:235). GnRH agonists are used only temporarily, because their anti-estrogen side effects include menopausal symptoms and bone loss, and upon withdrawal, the leiomyomas rapidly regrow.
Histologically, there is often initially edema and necrosis, followed by hyalinization and lymphocytic infiltrate (B and T cells). In this case, there was a prominent vasculitis. The patient had no history of a prior vasculitis and at follow up 3 years later, there was no evidence of vasculitis.
