
Chemistry, toxicology & urinalysis
General chemistry
Paraproteins
Monoclonal gammopathy testing
Author: Jieli (Shirley) Li, M.D., Ph.D.
Deputy Editor-in-Chief: Patricia Tsang, M.D., M.B.A.

Last author update: 20 October 2022
Last staff update: 17 January 2023
Copyright: 2022-2024, PathologyOutlines.com, Inc.
PubMed Search: Monoclonal gammopathy testing
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Laboratory | Interpretation | Test limitations | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Li JS. Monoclonal gammopathy testing. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/chemistrymonoclonalgammopathy.html. Accessed April 26th, 2024.
Definition / general
- Monoclonal gammopathies are plasma cell disorders, ranging from benign monoclonal gammopathy of undetermined significance (MGUS) to malignant diseases of multiple myeloma (MM) and amyloid light chain (AL) amyloidosis, with characteristic excretion of a monoclonal immunoglobulin (M protein)
- Monoclonal protein (M protein) usually demonstrates a single restricted peak / dense band in the gamma, beta or alpha 2 region
- Immunofixation or immunosubtraction is used to identify the heavy chain and light chain types of the M spike
Essential features
- Interpretation of serum electrophoresis and immunoglobulin profiles forms an important part of the investigation of immune function
- Current available methods to detect M proteins include gel and capillary serum and urine protein electrophoresis (SPEP and UPEP), serum and urine immunofixation (sIFE and uIFE), immunosubtraction (ISUB) and mass spectrometry (MS)
- International Myeloma Working Group in 2014 and the College of American Pathologists in 2021 published a consensus and guidelines on diagnosis of multiple myeloma
- There are still challenges in different methodologies, although they have advantages and disadvantages, especially the potential interferences caused by therapeutic monoclonal antibodies
Terminology
- Monoclonal protein / spike (M protein / M spike)
- Immunoparesis (suppression of uninvolved immunoglobulin isotypes in myeloma)
- Serum / urine protein electrophoresis (SPEP / UPEP)
- Immunofixation electrophoresis (IFE)
- Immunosubtraction (ISUB)
Laboratory
- Protein electrophoresis can be performed on agarose gels, capillary electrophoresis (CE) and mass spectrometry; gel and capillary electrophoresis are FDA approved, while mass spectrometry (MALDI-TOF) electrophoresis is a laboratory developed test (LDT) (Blood Cancer J 2021;11:24)
- Immunosubtraction (ISUB), an alternative to immunofixation (IFE) on agarose gels, runs on CE
- Serum protein electrophoresis is performed either on gel or by capillary based technology in order to discover / monitor paraproteins
- Urine protein electrophoresis is performed either on gel or by capillary based technology in order to discover / monitor free light chains (Bence Jones protein) in light chain myeloma or intact monoclonal immunoglobulin, particularly in poor renal function
- Cerebrospinal fluid (CSF) protein electrophoresis is performed mostly using gel based technique for the diagnosis of tumors in the central nervous system or neurological illness; a serum protein electrophoresis should be performed simultaneously to rule out potential elevated CSF proteins from systemic production
- IFE / ISUB is performed to identify / distinguish monoclonal proteins in serum / CSF or Bence Jones proteins in urine
- Nephelometric immunoassay techniques are performed to detect either an intact immunoglobulin M protein or a monoclonal free light chain
IFE (Sebia) ISUB (Sebia) MALDI-TOF MS (Mass Fix) Gel Yes No No Band / peak Present Absent Present Automated No Yes Yes Technically demanding More Less More Labor intensive Very much Much less (automated) In between FDA approved Yes Yes No IgD and IgE Yes No No
Interpretation
- IgG is the major immunoglobulin in the γ region
- Elevations of IgG occur with infections, liver disease, autoimmune disease and multiple myeloma (accounting for 52%)
- Reduction of IgG may indicate genetic immunodeficiency, nonsecretory myeloma or amyloid AL
- IgA is the other major isotype of dimer immunoglobulin
- Elevations of IgA occur with cirrhosis, mucosal infections and malignancy (multiple myeloma accounting for 21%)
- Elevations of IgA usually cause increase in the β and β-γ regions, which is termed β-γ bridging
- IgA deficiency is most commonly seen in congenital immunodeficiencies
- IgM is a pentamer immunoglobulin
- Elevations of IgM may occur with infections or malignancy (multiple myeloma accounting for 0.5%)
- Majority of lymphoplasmacytic lymphoma (Waldenström macroglobulinemia)
- IgM deficiency rarely happens
- IgD is one of the major isotypes of immunoglobulin in lymphocytes
- Elevations of IgD may occur with hyper IgD syndrome or malignancy
- IgD multiple myeloma accounts for around 2%
- IgE is another isotype of immunoglobulin
- IgE multiple myeloma is rarely seen (< 0.1%) (Adv Lab Med 2022;3:79)
- Serum free light chains (sFLC) (free light chain only monoclonal proteins accounting for 20%) are important biomarkers for the diagnosis and management of plasma cell disorders such as multiple myeloma (Arch Pathol Lab Med 2022;146:575)
- Diagnosis of multiple myeloma:
- 2014 International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma (Lancet Oncol 2014;15:e538):
- Clonal bone marrow plasma cells ≥ 10% or biopsy proven bony or extramedullary plasmacytoma
- Evidence of end organ damage that can be attributed to the underlying plasma cell proliferative disorder (CRAB - hypercalcemia, renal failure, anemia and bone lesions)
- FLC κ/λ ≥ 100
- > 1 focal lesion (≥ 5 mm) on MRI studies
- 2014 International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma (Lancet Oncol 2014;15:e538):
2021 College of American Pathologists laboratory detection and initial diagnosis of monoclonal gammopathies: guideline from the College of American Pathologists in collaboration with the American Association for Clinical Chemistry and the American Society for Clinical Pathology (Arch Pathol Lab Med 2022;146:575)
| Guideline statement | Strength of recommendation |
| 1. Clinical care providers should order both serum protein electrophoresis (SPEP) and serum free light chains (sFLC) for the initial detection of monoclonal immunoglobulin protein (M protein) in all patients with suspected monoclonal gammopathies | Strong recommendation |
| 2. Laboratorians should confirm a SPEP abnormality suspicious for an M protein with additional testing by serum immunofixation electrophoresis (sIFE) or alternative method with similar sensitivity | Strong recommendation |
| 3. Laboratorians or clinical care providers should follow up an abnormal sFLC ratio for the presence of an M protein with a serum IFE or alternative method with similar sensitivity | Conditional recommendation |
| 4. Clinical care providers should order SPEP, sFLC, serum IFE and urine IFE for the initial detection of M protein in all patients with suspected amyloid light chain (AL) amyloidosis | Strong recommendation |
| 5. Clinical care providers should not order heavy / light chain isotype assay (hlc) for initial detection of M protein in patients with suspected monoclonal gammopathies | Strong recommendation |
| 6. Clinical care providers should not use total / intact light chains for the quantitation of M proteins in patients with suspected myeloma | Strong recommendation |
| 7. In patients with intact M proteins outside the gamma region by SPEP, laboratories should use total immunoglobulin (IgA, IgG or IgM) for the quantitation of the M proteins; quantitation of a band in the beta region by SPEP can be performed if the M protein is distinguished from background normal protein bands | Conditional recommendation |
| 8. Laboratorians should report both quantitative levels of free kappa and free lambda and the rFLC when the sFLC assay is performed | Strong recommendation |
| 9. Clinical care providers may use rFLC, IgM isotype, M protein > 1.5 g/dL and immunoparesis as risk factors for progression to MM or a B cell lymphoproliferative disorder | Conditional recommendation |
Test limitations
- Despite major advances over the last decade, there are still challenges in routine practice of monoclonal gammopathy measurements
- Hidden light chains in monoclonal proteins have been recognized on gel based immunofixation, as may be seen as a separate large clonal heavy chain without a comigrating light chain band
- Reason for hidden light chains may be the inaccessible light chain epitopes in the folded tertiary or quaternary structure of some monoclonal proteins; one of the possible approaches to revealing the hidden light chain band is to use the chemical reduction agent 2-mercaptoethanol or dithiothreitol in serum samples by breaking up disulfide bonds
- There have been quite a few cases reporting the detection of therapeutic antibodies at their high dose, including daratumumab, siltuximab, ofatumumab, elotuzumab, pembrolizumab and belantamab mafodotin; as a result, the likelihood of encountering interferences from therapeutic antibodies in the clinical laboratory has been increasing
- With current technologies used in most clinical laboratories for the detection, identification and isotyping of M proteins, there is limited ability to recognize the presence of monoclonal antibody therapeutics at the analytical phase of testing
- Given the limited analytical solutions to the problem of monoclonal antibody interferences, newer approaches, such as robust mass spectrometry, are needed to overcome the challenges
- Reference: Keren: Protein Electrophoresis in Clinical Diagnosis, 1st Edition, 2012
Board review style question #1
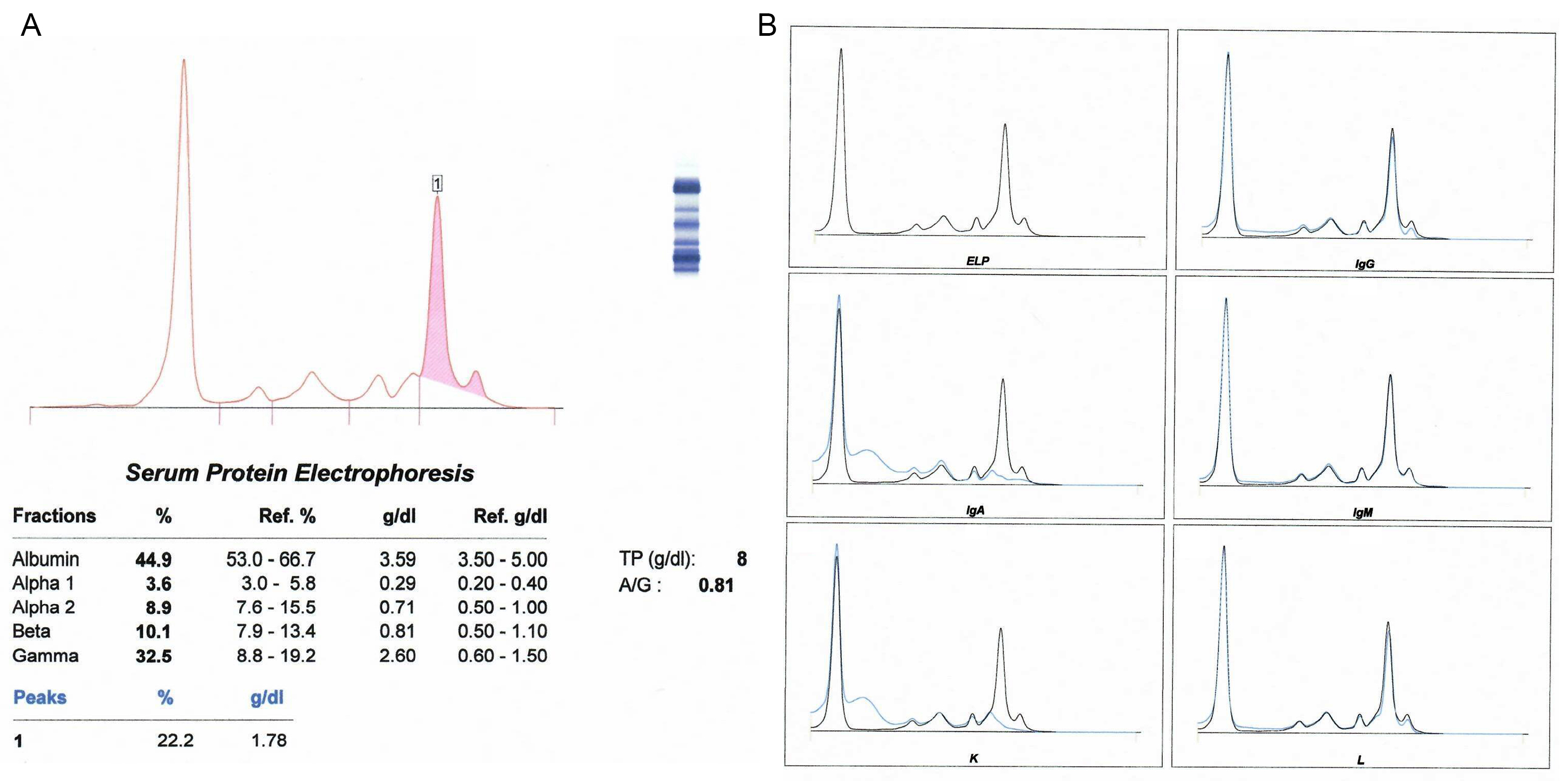
A 74 year old man was admitted to the hospital due to complications from chronic heart failure disease. Skeletal Xrays revealed diffuse areas of patchy demineralization that could represent osteoporosis. Serum protein electrophoresis (A) was performed with capillary electrophoresis results shown above. For the serum protein electrophoresis (SPEP), measured protein was 8 g/dL (reference interval: 6.4 - 8.3 g/dL) and the shaded area has a density estimate of 1.78 g/dL, indicating possible abnormalities in the gamma region. The sample was reflexed to immunosubtraction (B). What is the most probable explanation for these findings?
- Monoclonal protein free kappa is present
- Monoclonal protein IgA kappa is present
- Oligoclonal protein is present
- Polyclonal protein IgA kappa is present
Board review style answer #1
B. Monoclonal protein IgA kappa is present. The serum protein electropherogram result suggests 2 monoclonal gammopathies in the γ globulin region. Immunofixation electrophoresis (IFE) identified these as IgA kappa. The Xrays suggest the possibility of lytic lesions. The chronic heart failure is unrelated. The patient has multiple myeloma with IgA kappa monoclonal proteins.
Comment Here
Reference: Monoclonal gammopathy testing
Comment Here
Reference: Monoclonal gammopathy testing
Board review style question #2
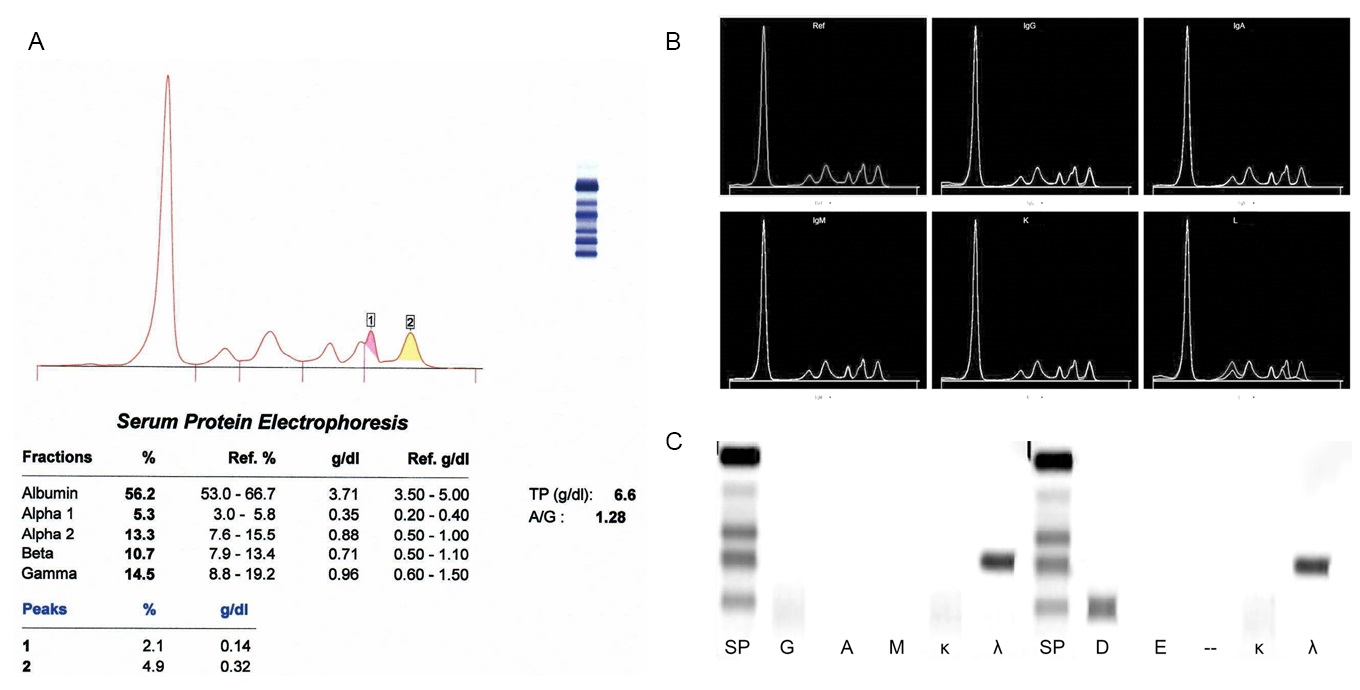
An 84 year old woman was seen in the emergency department after experiencing the sudden onset of severe pain in the left femoral region. She declined history of falling or trauma. She also denied back pain. Skeletal Xrays revealed a fracture of the left femoral region and a compression fracture of a lower lumbar vertebra. Skeletal Xrays also showed multiple punched out lesions. Serum protein electrophoresis (A) was performed with capillary electrophoresis results shown above. For the serum protein electrophoresis (SPEP), measured protein was 6.6 g/dL (reference interval: 6.4 - 8.3 g/dL) and the shaded area has a density estimate of 0.14 g/dL and 0.32 g/dL in the beta 2 and gamma region, respectively, indicating possible abnormalities in the beta 2 and gamma regions. The sample was reflexed to immunosubtraction (B) to identify the subtype of monoclonal proteins. The immunosubtraction results showed subtraction for λ light chain only in both peaks, suggesting 2 monoclonal λ light chains but no corresponding heavy chains subtracted. Due to lack of anti-IgD and E antisera for immunosubtraction, immunofixation (C) was performed to identify the subtype of monoclonal proteins. Immunofixation against D and E antisera confirmed the presence of an IgD monoclonal protein in the gamma region. The D and λ bands migrate separately, D is in gamma region while λ is in beta region, which is discrepant with the findings of 2 monoclonal λ light chains in immunosubtraction. For the discrepancy between immunofixation and immunosubtraction results, what else can be done using immunofixation to further evaluate this specimen?
- No need to repeat immunofixation because it is monoclonal IgD only + free λ
- Repeat immunofixation after bringing specimen to 37 °C
- Repeat immunofixation after chemical reduction of serum specimen with 2-mercaptoethanol
- Repeat immunofixation with higher dilution of serum to get the concentration lower
Board review style answer #2
C. Repeat immunofixation after chemical reduction of serum specimen with 2-mercaptoethanol. The medical laboratories should be aware of the described scenario. The failure to detect light chains of certain intact M proteins is most likely due to the structural inaccessibility of light chains. It is recommended that treatment with reduction agents or use of an alternative methodology or immunosubtraction might be helpful for investigating suspected heavy chain only cases, due to the limitation of conventional methodology.
Comment Here
Reference: Monoclonal gammopathy testing
Comment Here
Reference: Monoclonal gammopathy testing
