Colon
Polyps
Adenoma overview
Editorial Board Member: Monika Vyas, M.D.
Deputy Editor-in-Chief: Catherine E. Hagen, M.D.

Last author update: 31 January 2022
Last staff update: 31 January 2022
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Colon adenoma[TI] free full text[SB]

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Diagrams / tables | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Ding CKC, Wen KW. Adenoma overview. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/colontumoradenoma.html. Accessed September 22nd, 2025.
Definition / general
- Sometimes referred to as conventional adenoma to be distinguished from serrated lesions
- Serrated lesions are of different pathway and are not included in this topic
- Benign, premalignant neoplasm composed of dysplastic colorectal epithelium
Essential features
- Premalignant lesions
- At least low grade dysplasia; absence of true invasion
- Subtypes include tubular adenoma (most common), villous adenoma, tubulovillous adenoma and advanced adenoma
Terminology
- Conventional colorectal adenoma
ICD coding
- ICD-O:
- ICD-11: 2E92.4Y & XH7SY6 - other specified benign neoplasm of the large intestine & tubular adenoma, NOS
Epidemiology
- High incidence in populations with diets typical of high income countries with a sedentary lifestyle
- High risk population overlap with those of colorectal adenocarcinoma (see Etiology)
Sites
- Colon
Pathophysiology
- Adenoma - carcinoma sequence: genetic changes that occur before morphologically identifiable tumor formation, including a small set of driver genes (APC, CNNTB1, KRAS, SMAD4 and TP53) (Proc Natl Acad Sci U S A 2013;110:1999)
- APC genetic alteration results in reduced degradation of beta catenin and dysregulated WNT signaling (Science 1997;278:120)
- Inherited (constitutional) APC alterations lead to familial adenomatous polyposis
- Activating KRAS mutations leads to growth dysregulation through MAPK pathway (Br J Cancer 1997;75:341)
- SMAD deletion leads to disruption of TGFb growth inhibitory pathway
- Alteration of PTEN or activation of PIK3CA disrupts PI3K pathway, inhibits apoptosis and promotes neoplastic cell survival (Nat Commun 2016;7:11971, Nat Commun 2014;5:4961)
- Alteration of TP53 allows the cells to survive DNA damage and other cellular stresses (Int J Cancer 1995;64:47)
- APC genetic alteration results in reduced degradation of beta catenin and dysregulated WNT signaling (Science 1997;278:120)
- Small subset of adenoma acquires defect in DNA mismatch repair genes (predominantly hypermethylation of the MLH1 promoter) (Gastroenterol Hepatol Bed Bench 2017;10:S117)
Etiology
- Increased risk associated with consumption of processed and red meat, alcohol, excess body fat (Lancet Oncol 2015;16:1599, Ann Oncol 2017;28:1788, N Engl J Med 2016;375:794)
- Decreased risk associated with consumption of dietary fiber and dairy products, increased levels of physical activity (Ann Oncol 2017;28:1788, BMJ 2016;354:i3857)
Diagrams / tables
Images hosted on other servers:

Adenoma carcinoma sequence
Clinical features
- See Diagnosis
Diagnosis
Prognostic factors
- Most adenomas do not progress through the adenoma carcinoma sequence
- Risk is associated with:
- Higher number of lesions
- Larger size
- Higher proportion of villous architecture
- Extent of high grade dysplasia
Case reports
- 61 year old man with rectal bleeding for 1 week (Medicine (Baltimore) 2020;99:e20985)
- 66 year old woman with homogeneous segmental bowel wall thickening (BJR Case Rep 2020;6:20200016)
- 76 year old man with positive fecal occult blood test (Tokai J Exp Clin Med 2016;41:22)
Treatment
- Major treatment: endoscopic biopsy or resection
- According to NCCN Guidelines for Colorectal Cancer Screening (version 2.2021), if pathology identified:
- Low risk adenoma: < 2 polyps and < 1 cm
- Repeat colonoscopy in 7 - 10 years
- High risk polyp:
- High grade dysplasia present
- Villous / tubulovillous histology
- 3 - 10 adenomatous polyps (serrated lesions are discussed in different section)
- Repeat colonoscopy in 3 years; if negative, repeat colonoscopy in 5 years
- If positive, treat according to the pathology finding
- Large colorectal polyps (> 1 cm in size) without invasion:
- If pedunculated, colonoscopy in 3 years
- Sessile morphology with no high risk endoscopic features for invasive cancer:
- If complete resection and no unfavorable risk factors, colonoscopy in 1 - 3 years
- If incomplete resection, referral for surgery evaluation or expertise in management of large colorectal polyps
- Sessile morphology with high risk endoscopic features, even if no invasive cancer identified by pathology - surgical evaluation or expertise in management of large colorectal polyps
- Low risk adenoma: < 2 polyps and < 1 cm
- Reference: National Comprehensive Cancer Network: NCCN Guidelines - Colorectal Cancer Screening [Accessed 18 October 2021]
Clinical images
Images hosted on other servers:

Giant villous adenoma

Several adenomas
Gross description
- Specimen is received in formalin, additionally labeled transverse colon polyps and consists of 2 soft, irregular, red-tan tissue fragments (0.5 x 0.3 x 0.2 cm in aggregate)
- Specimen is received in formalin, additionally labeled right colon and consists of multiple tan to white, soft, irregular mucosal tissue fragments (0.8 x 0.2 x 0.2 cm in aggregate)
Gross images
Images hosted on other servers:

Polypoid tumor with gyrated surface sitting on a short stalk

Polypoid tumor
Microscopic (histologic) description
- Tubular adenomas:
- Conserved crypt architecture with variable elongation of the crypts and an increased number of glands
- At least low grade dysplasia: hyperchromatic nuclei, nuclear spindling and stratification, loss of cell polarity
- Decreased numbers of goblet cells and absorptive cells
- Small (< 25%) villous component is acceptable
- Tubulovillous adenoma:
- Similar to tubular adenoma but with 25 - 75% of villous component
- Villous component: architecture that resemble small intestinal villi
- Villous adenoma:
- > 75% of villous component
- Advanced adenoma:
- All adenomas with a size > 10 mm
- With tubulovillous or villous architecture
- With or without high grade dysplasia
- Highest risk of synchronous of metachronous adenomas
- Rare subtypes:
- Paneth cell rich subtype (more common in proximal colon or in younger patients) (Hum Pathol 2009;40:872, Sci Rep 2016;6:26129)
- Squamous components might be present as morules or squamous metaplasia (Pathobiology 2005;72:269)
- Other rare morphological findings (Histopathology 2021;78:348):
- Clear cell metaplasia or clear cell change
- Note the clear or vacuolated cytoplasm are not mucin
- Osseous metaplasia or heterotopic ossification
- Neuroendocrine differentiation
- Neuroendocrine hyperplasia
- Neuroendocrine metaplasia
- Neuroendocrine cell proliferation
- Composite intestinal adenoma microcarcinoid
- Mixed neuroendocrine - nonneuroendocrine neoplasm (MiNEN)
- Mixed adenoma - neuroendocrine tumor (MANET)
- Signet ring cell-like lesion
- Clear cell metaplasia or clear cell change
- Histology grading:
- 2 tiered system: low grade versus high grade
- Criteria for high grade dysplasia:
- Architecture: marked complex glandular crowding with glandular irregularity; cribriform architecture; intraluminal necrosis; can be observed at low power
- Cytology: substantial loss of cell polarity, marked enlarged nuclei with prominent nucleoli, dispersed chromatin pattern, atypical mitotic figures (Eur J Gastroenterol Hepatol 2002;14:183, Colorectal Dis 2015;17:682)
- Should be no evidence for invasion, however, pseudoinvasion (epithelial misplacement) could sometimes be seen due to prolapse (Mod Pathol 2015;28:S88)
- Features favoring pseudoinvasion / epithelial misplacement:
- Signs suggestive of previous epithelial trauma (extracellular mucin, hemorrhage or hemosiderin)
- Focus appears to be continuous with the surface epithelium with similar cytology
- Signs of mucosal prolapse such as muscular proliferation
- Acute necrosis of the surface
- Features favoring adenocarcinoma:
- Isolated glands without accompanying lamina propria
- Budding
- Vascular invasion
- Poor differentiation in morphology
- Concurrent review by more than 1 GI pathologist is suggested if high grade dysplasia is present
- Features favoring pseudoinvasion / epithelial misplacement:
Microscopic (histologic) images
Contributed by Chien-Kuang Cornelia Ding, M.D., Ph.D., Kwun Wah Wen, M.D., Ph.D. and Enoch Kuo, M.D.
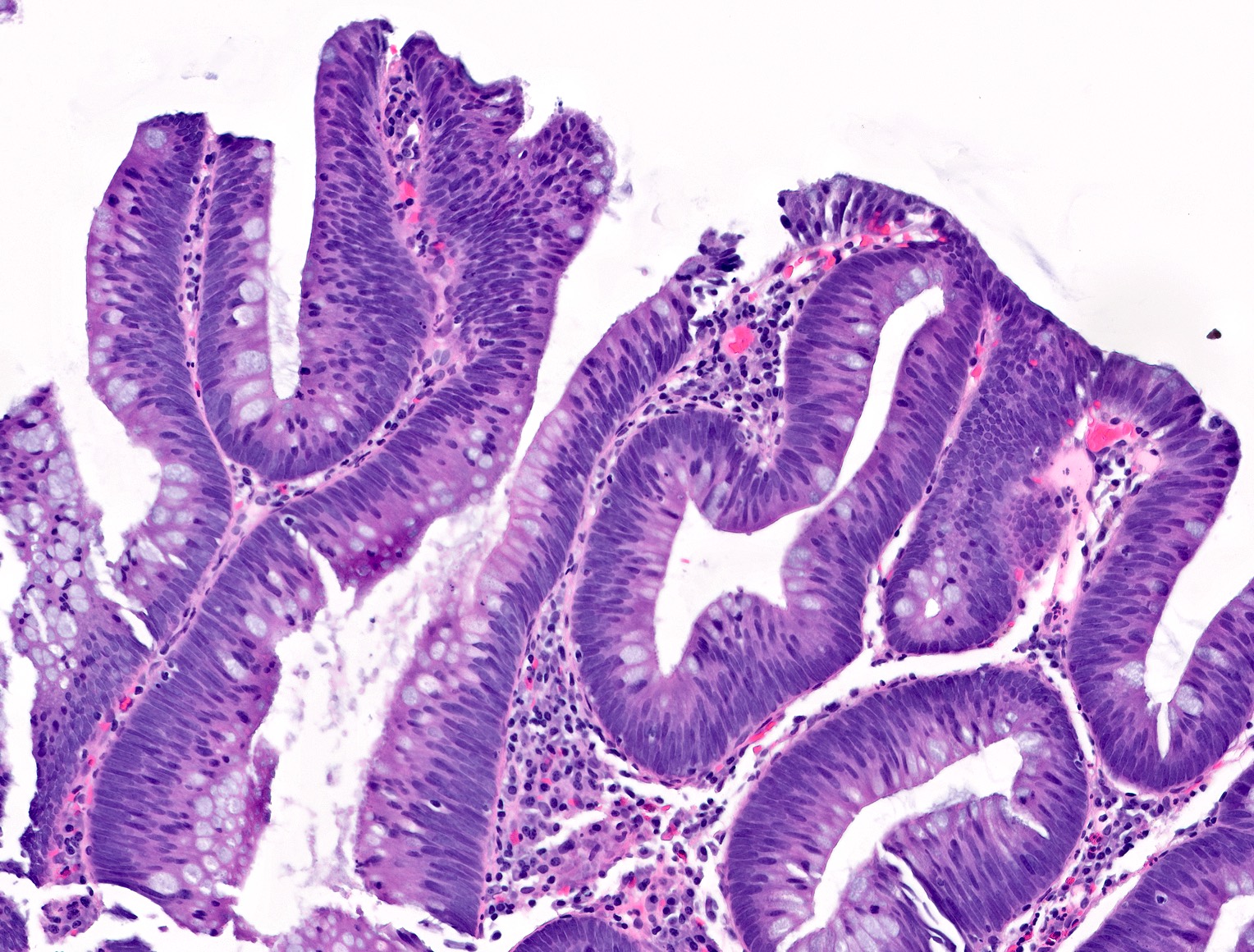
Tubular adenoma
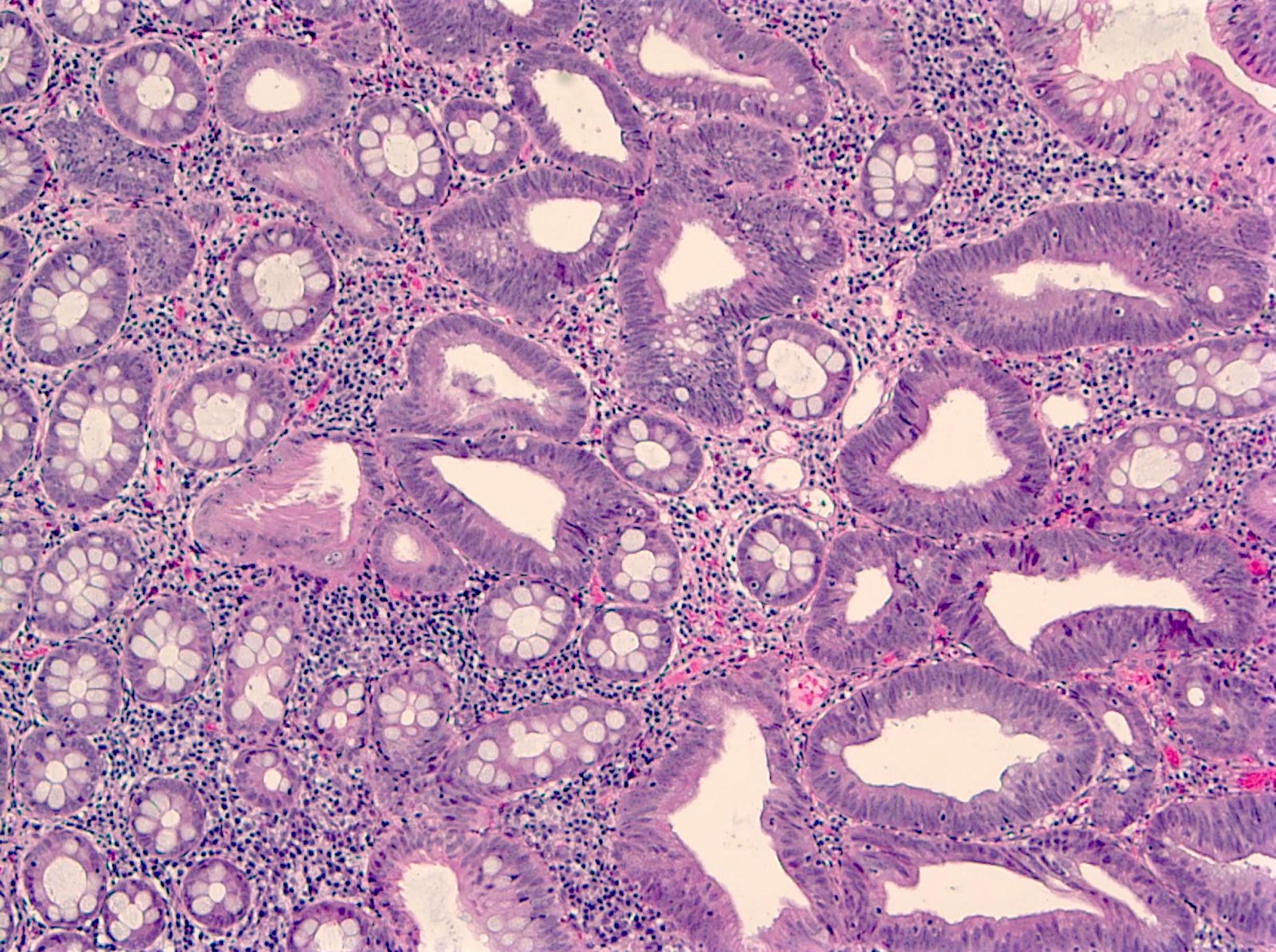
Low grade tubular adenoma
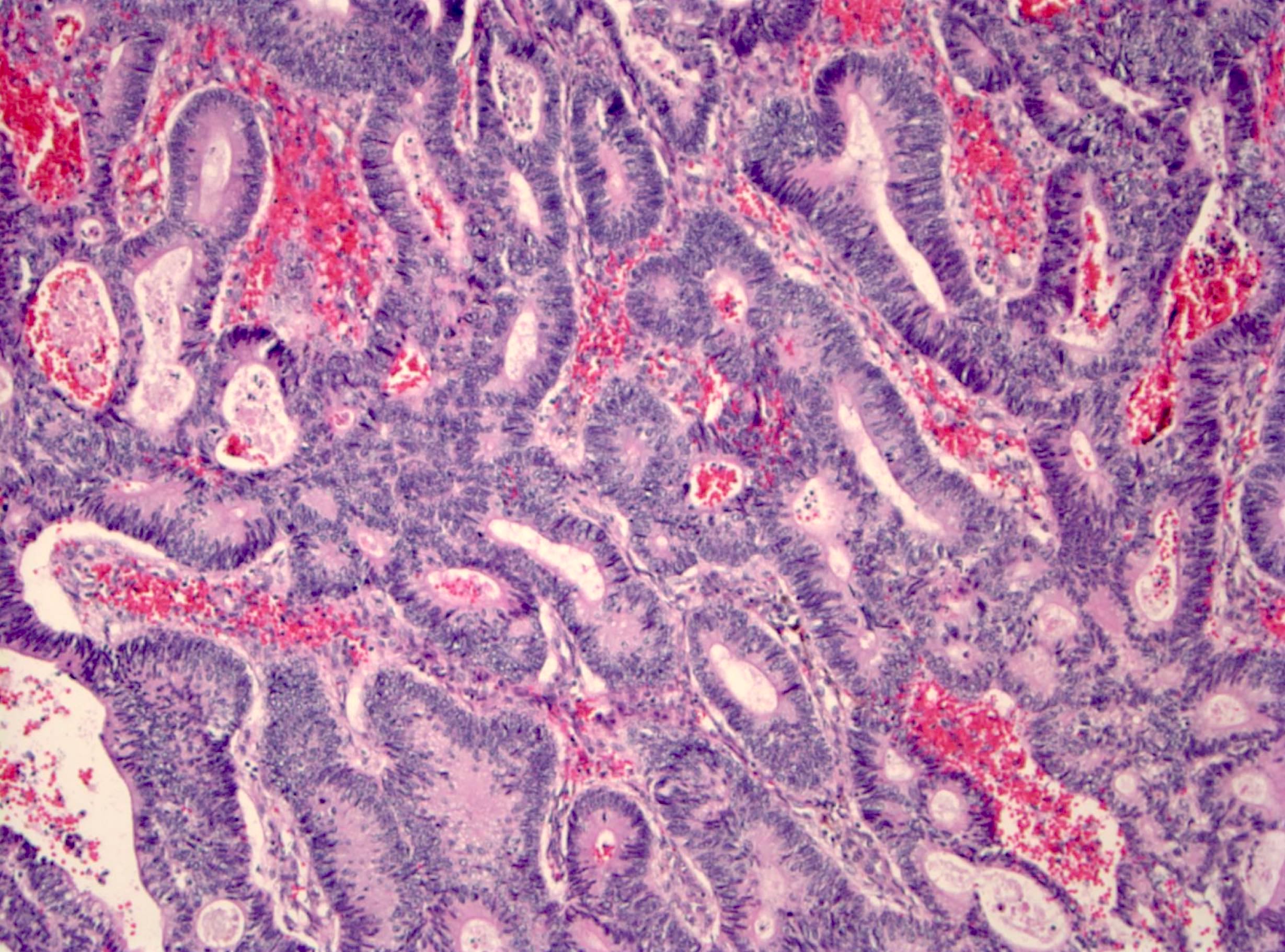
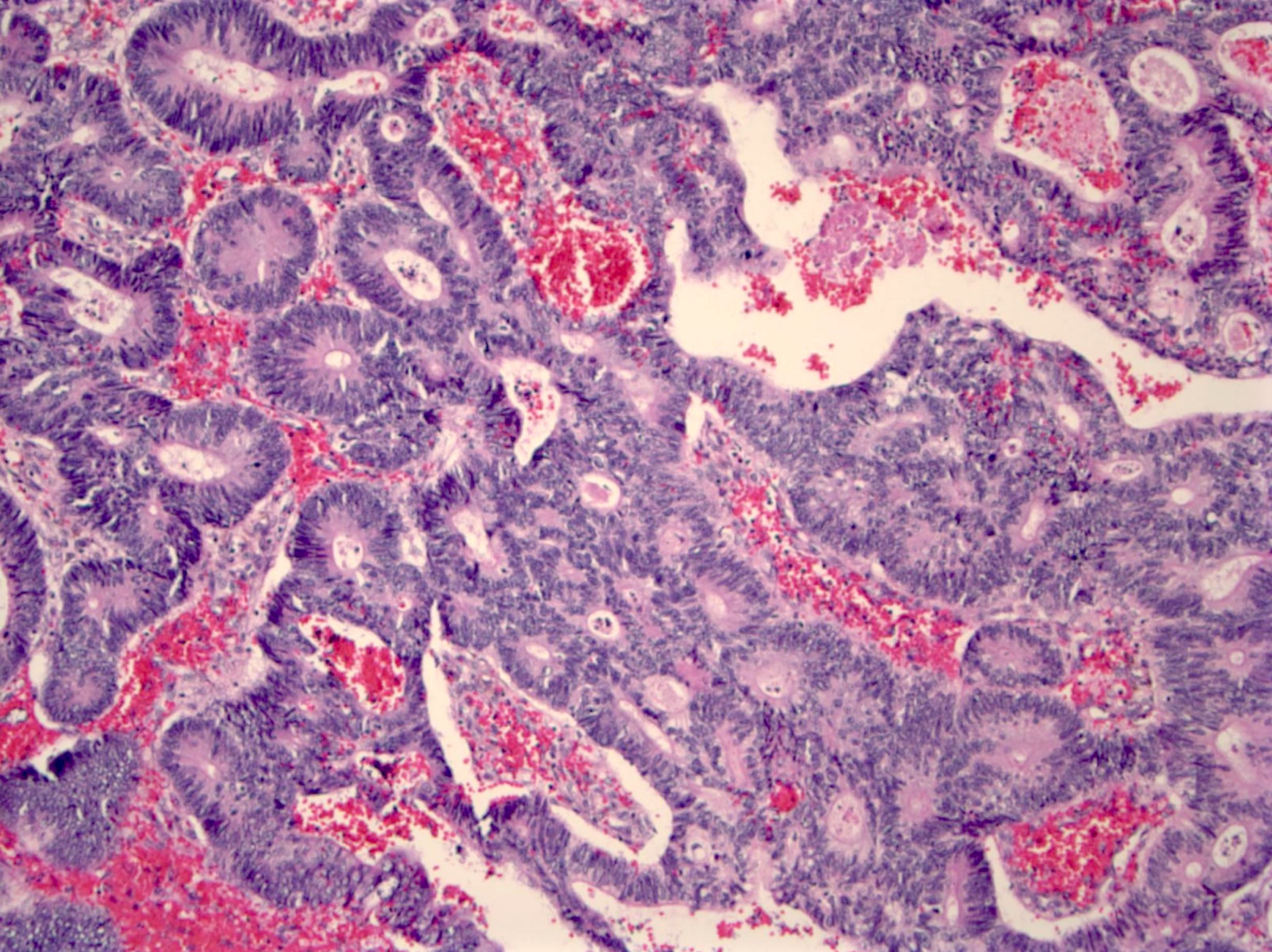
Tubular adenoma with high grade dysplasia
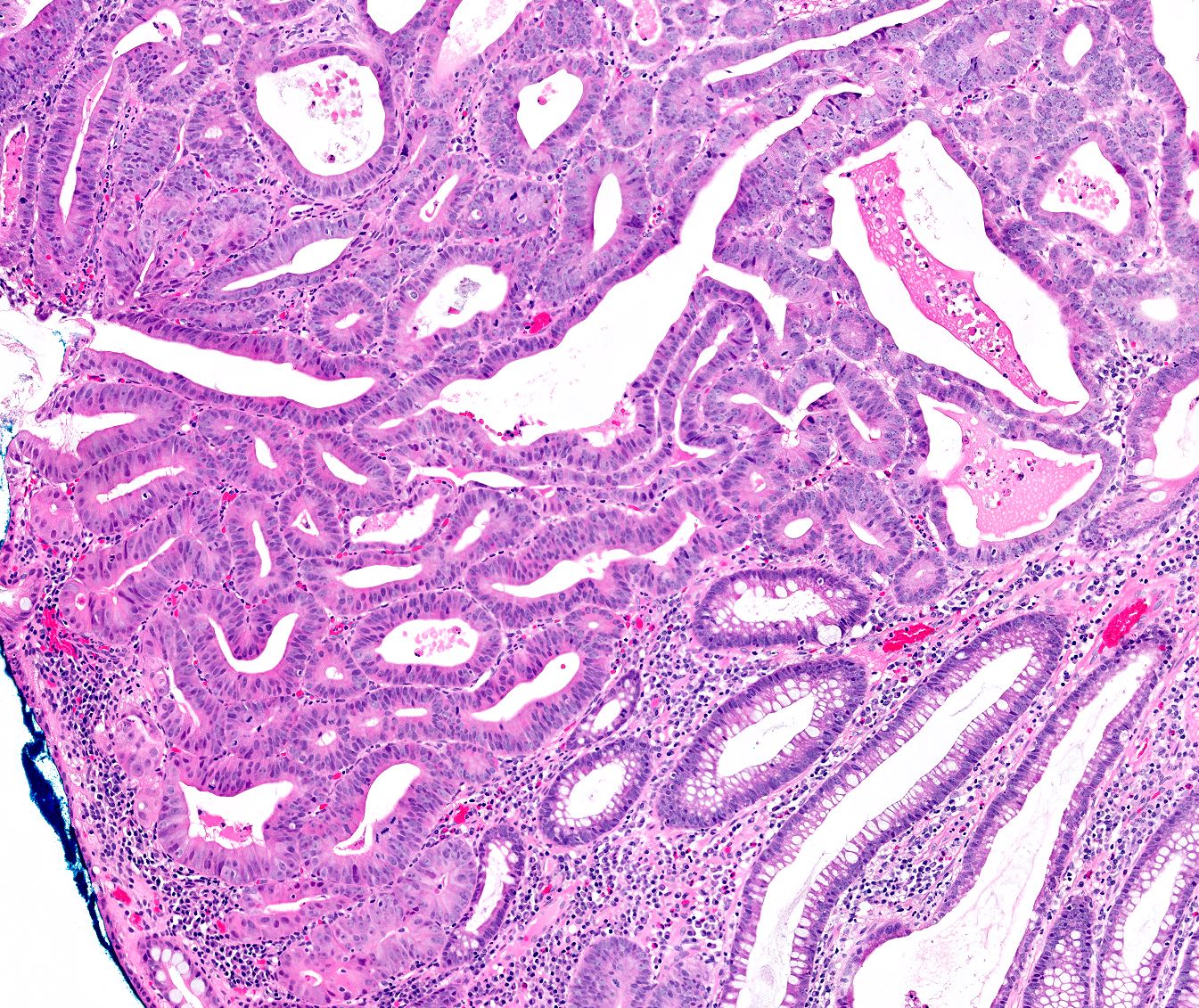
Focal high grade dysplasia
Virtual slides
Images hosted on other servers:

Tubulovillous adenoma

High grade dysplasia
Molecular / cytogenetics description
- Not routinely performed, although majority of cases will have chromosomal instability; a subset (~25%) of cases will show TP53 mutations
Videos
Tubular adenoma
Colon dysplasia
Villous adenoma
Sample pathology report
- Colon, hepatic flexure polyp, biopsy:
- Tubular adenoma with focal high grade dysplasia
- Ascending colon, polyp, endoscopic mucosal resection:
- Fragments of tubulovillous adenoma (see comment)
- Comment: No high grade dysplasia is identified. Specimen fragmentation precludes assessment of specimen margins.
Differential diagnosis
- Reactive colonic mucosa:
- Smaller nuclei with basal orientation
- No or less significant hyperchromasia or pseudostratification
- More abundant cytoplasm and mucin
- Invasive adenocarcinoma:
- At least invasion through muscularis mucosa into the submucosa
- Desmoplasia, single cells
- Traditional serrated adenoma:
- Sawtooth luminal / surface contour
- Ectopic crypts characterized by aberrant budding crypts
Practice question #1
Which of the following genetic changes is considered a driver mutation in colonic adenoma?
- BCL2
- KIT
- RB
- TP53
Practice answer #1
D. TP53. Alteration of TP53 allows cells to survive DNA damage and other cellular changes. It is found in ~25% of adenomas.
Comment Here
Reference: Adenoma overview
Comment Here
Reference: Adenoma overview
Practice question #2
According to 2021 NCCN guidelines for colorectal cancer screening, which of the following is a feature of low risk colonic adenomatous polyp(s)?
- 2 adenomas
- High grade dysplasia
- Tubulovillous histology
- Villous histology
Practice answer #2
A. The number of adenomatous polyps considered to be a low risk feature is < 3.
Comment Here
Reference: Adenoma overview
Comment Here
Reference: Adenoma overview
