
Cytopathology
Effusion cytology
IHC panels


Copyright: 2022, PathologyOutlines.com, Inc.
PubMed Search: Immunostaining panels effusion cytology
Effusion cytology
IHC panels
Editorial Board Members: Bonnie Choy, M.D., Marc Pusztaszeri, M.D.
Last author update: 8 August 2022
Last staff update: 8 August 2022
Copyright: 2022, PathologyOutlines.com, Inc.
PubMed Search: Immunostaining panels effusion cytology

Table of Contents
Definition / general | Essential features | CPT coding | Sites | Diagrams / tables | Cytology description | Cytology images | Molecular / cytogenetics description | Molecular / cytogenetics images | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Lin LH, Brandler TC. IHC panels. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/cytopathologyihcpanels.html. Accessed September 16th, 2025.
Definition / general
- Serous cavities can be involved by metastatic neoplasms, inflammatory / infectious conditions or primary malignancies
- Immunostaining panels with correlation with cytomorphology and clinical information can aid in the differential diagnosis of serous fluid effusion
Essential features
- Clinical and radiological correlation with cytomorphology is vital to tailor an appropriate immunostain panel (Arch Pathol Lab Med 2013;137:647)
- Use of immunohistochemical panels is beneficial to avoid pitfalls as no single immunostain has 100% sensitivity or specificity
- Immunostaining can aid in the assessment of effusion cytopathology specimens by:
- Differentiating metastatic disease from mesothelioma (at least 2 markers for mesothelioma / 2 markers for metastasis) (Arch Pathol Lab Med 2013;137:647)
- Determining primary site or lineage of metastatic disease (Cancer Cytopathol 2018;126:590)
- Differentiating neoplastic from reactive mesothelial cells (Arch Pathol Lab Med 2013;137:647)
- Identifying potential therapeutic targets (Cancer Cytopathol 2018;126:590)
CPT coding
Sites
- Pleura, peritoneum, pericardium
Diagrams / tables
Contributed by Lawrence Hsu Lin, M.D., Ph.D. and Tamar C. Brandler, M.D., M.S.
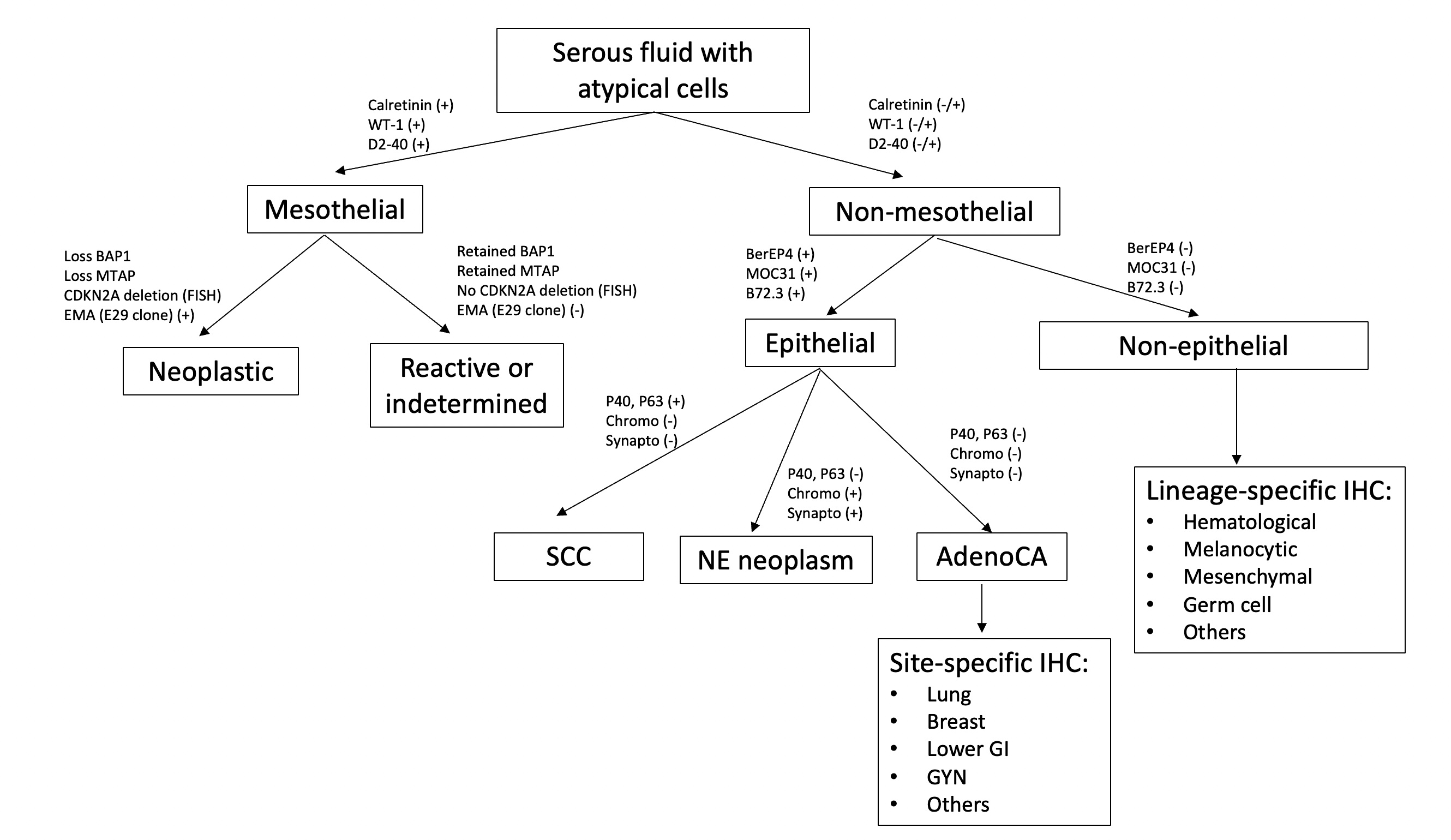
Serous fluid immunostain work up
Cytology description
- Use of immunostaining panel with multiple stains is beneficial since no single stain has 100% sensitivity or specificity
- Positive stains are more useful than negative stains since a larger percentage of cases in effusion can lose expression as compared with primary tumors
- Cytomorphology and correlation with clinical and radiological information can tailor immunostains panel in order to make the following differential diagnoses:
- Immunostains to differentiate mesothelioma from reactive mesothelial cells (Hum Pathol 2013;44:1, Mod Pathol 2020;33:245, Cancer Cytopathol 2018;126:54, Am J Clin Pathol 2009;131:516, Acta Cytol 2012;56:527):
Mesothelioma Reactive mesothelial cells BAP1 Lost (60% of cases) Retained MTAP Lost Retained EMA (E29 clone) Strong membranous Cytoplasmic / weak membranous Desmin Negative Positive
- Immunostains and special stains to differentiate mesothelioma from metastatic carcinoma (Hum Pathol 2013;44:1, Cancer Cytopathol 2014;122:299, Transl Lung Cancer Res 2020;9:S3):
- Ideally a panel with at least 2 mesothelial and 2 for metastatic carcinoma should be ordered (Arch Pathol Lab Med 2013;137:647)
- Pancytokeratins and CK7 should not be used in this differential diagnosis, as both metastatic carcinoma and mesothelioma can express them (Arch Pathol Lab Med 2013;137:647, Mod Pathol 2000;13:962)
Metastatic carcinoma Mesothelioma Calretinin Negative (can be positive in breast cancer, squamous cell carcinoma) Positive (nuclear and cytoplasmic) D2-40 Negative (can be positive in breast, lung and ovarian cancer) Positive (membranous) WT1 Negative (can be positive in gynecologic tumors) Positive (nuclear) CK5/6 Negative (positive in squamous cell carcinoma) Positive (cytoplasmic / membranous) Claudin4 Positive (membranous) Negative MOC31 Positive (membranous) Negative BerEP4 Positive (membranous) Negative B72.3 Positive (cytoplasmic) Negative CEA Positive (cytoplasmic) Negative PASD Positive (cytoplasmic granules) Negative Mucicarmine Positive (cytoplasmic mucin) Negative
- Immunostains to identify primary site or lineage of metastatic neoplasms (Cancer Cytopathol 2018;126:590, Adv Anat Pathol 2020;27:114, Hum Pathol 2013;44:1):
- Lung adenocarcinoma: TTF1 and Napsin A
- Thyroid: TTF1, PAX8, thyroglobulin
- Breast: mammaglobin, GCDFP-15, GATA3, ER
- Urothelial: p40 or p63 and GATA3
- Gynecological tract: PAX8, ER
- Lower gastrointestinal: CDX2, CK20 and SATB2
- Hepatocellular carcinoma: Arginase1, HepPar1, Glypican 3
- Renal cell carcinoma: PAX8, CAIX, RCC, CD10
- Prostate: NKX 3.1, PSA
- Squamous cell carcinoma: p40 and p63, CK5/6 (also positive in mesothelial cells)
- Neuroendocrine neoplasm: synaptophysin, chromogranin, INSM1, CD56
- Melanoma: SOX10, MelanA, S100, HMB45
- Hematological neoplasm: CD45, B cell marker (CD20, CD79a, PAX5), T cell marker (CD3), plasma cell marker (CD138), HHV8 in primary effusion lymphoma
- Vascular tumors: CD31, CD34, ERG
- Germ cell tumors: PLAP, OCT 3/4, SALL4, HCG
- Sex cord stromal tumors: calretinin (also positive in mesothelial cells), inhibin, SF1 and FOXL2
- Predictive and prognostic markers performed on cell block (Chandra: The International System for Serous Fluid Cytopathology, 1st Edition, 2020, J Am Soc Cytopathol 2017;6:33, Arch Pathol Lab Med 2021;145:46, J Clin Oncol 2018;36:2105, Arch Pathol Lab Med 2018;142:291, Cancer Cytopathol 2015;123:117, Cancer Cytopathol 2018;126:421, Am J Surg Pathol 2017;41:1547, Cancer Cytopathol 2017;125:896):
Immunostain Staining pattern Typically performed in Significance Additional testing ER / PR Nuclear Breast cancer Hormonal therapy for ER / PR positive tumors N/A HER2 Membranous Breast, gastric, gastroesophageal, endometrial cancer Anti HER2 therapy for HER2 positive tumors; specimens should be placed in 10% neutral buffered formalin as soon as possible and fixed for 6 - 72 hours FISH is used in equivocal results (2+) Mismatch repair proteins Nuclear Metastatic colorectal, endometrial, cholangiocarcinoma Immunotherapy for tumors with loss of mismatch repair protein PCR or NGS can be used to evaluate microsatellite instability ALK Cytoplasmic Non small cell lung cancer (NSCLC), inflammatory myofibroblastic tumor ALK inhibitors for tumors with ALK fusions or positive ALK immunostain FISH, PCR or NGS can be used as alternative to immunostaining ROS1 Cytoplasmic and membranous NSCLC ROS1 inhibitors for tumors with ROS1 fusions Immunostain is a screening method; FISH, PCR or NGS confirmation is necessary Pan TRK Nuclear, perinuclear, cytoplasmic and membranous Variety Anti NTRK therapy for tumors with NTRK fusions Immunostain is a screening method; molecular confirmation (typically NGS) is necessary PDL1 Membranous NSCLC Immunotherapy for PDL1 positive tumors; type of scoring and cut off points depend on antibody clone and type of tumor N/A
- Immunostains to differentiate mesothelioma from reactive mesothelial cells (Hum Pathol 2013;44:1, Mod Pathol 2020;33:245, Cancer Cytopathol 2018;126:54, Am J Clin Pathol 2009;131:516, Acta Cytol 2012;56:527):
Cytology images
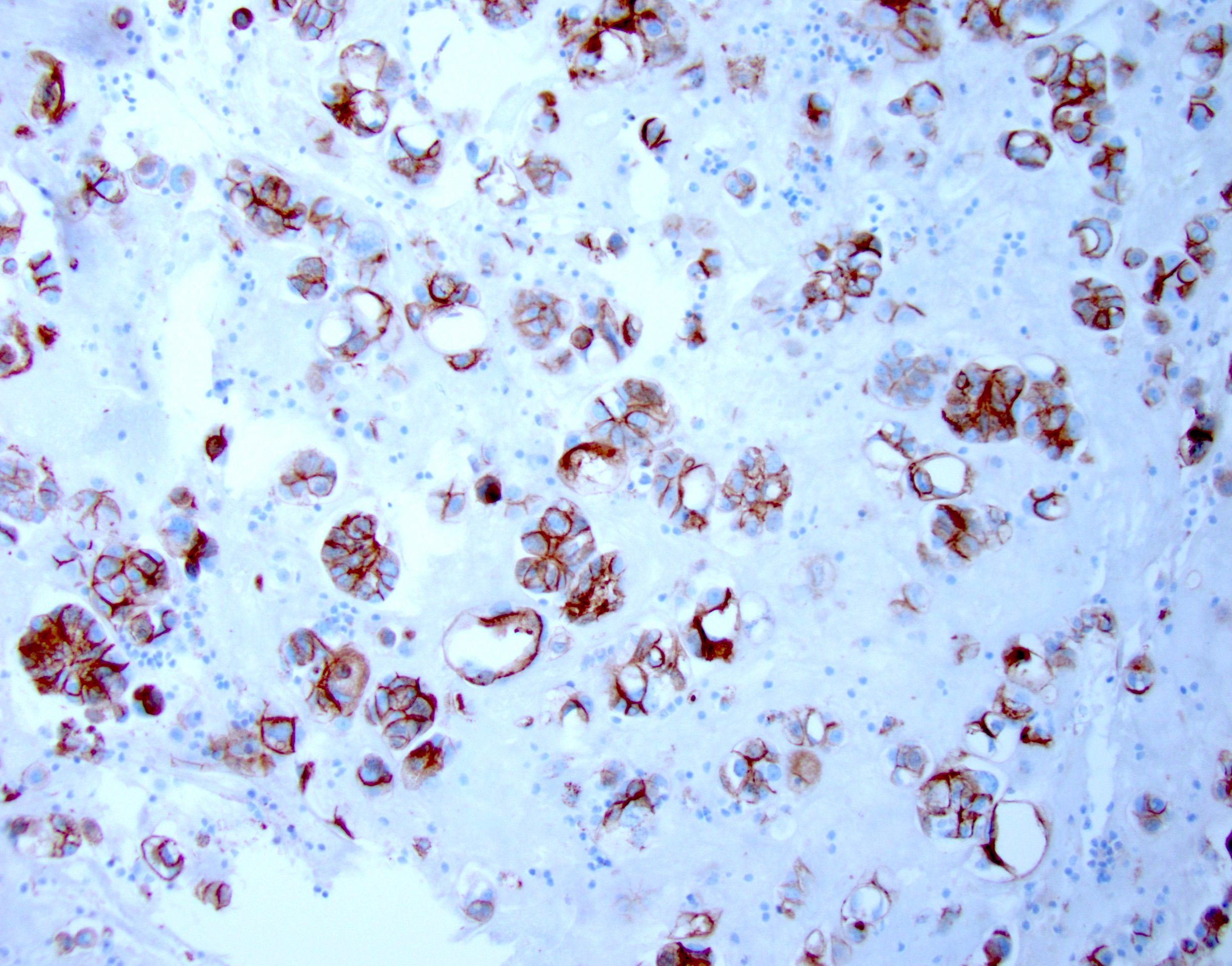
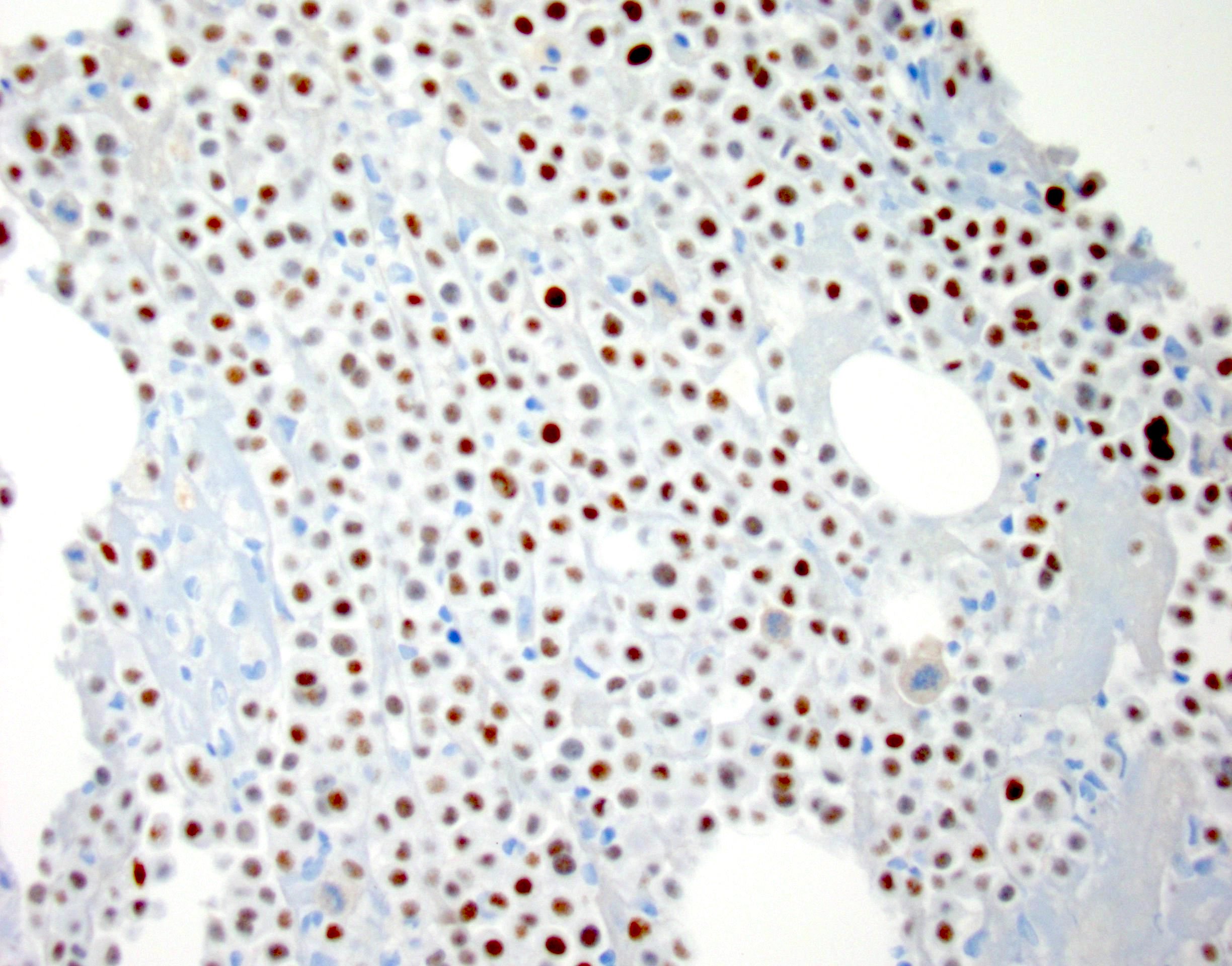
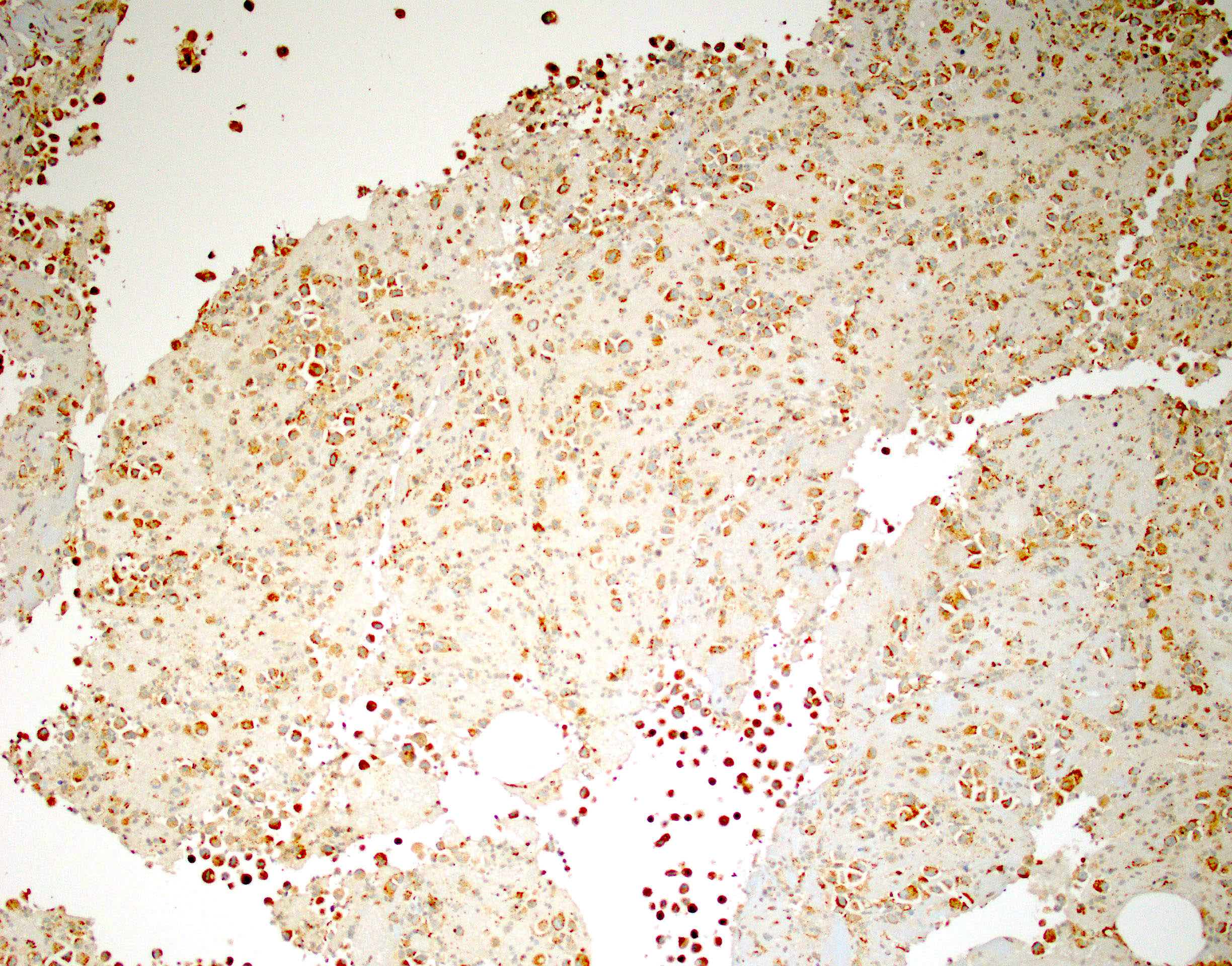
Contributed by Lawrence Hsu Lin, M.D., Ph.D. and Tamar C. Brandler, M.D., M.S.

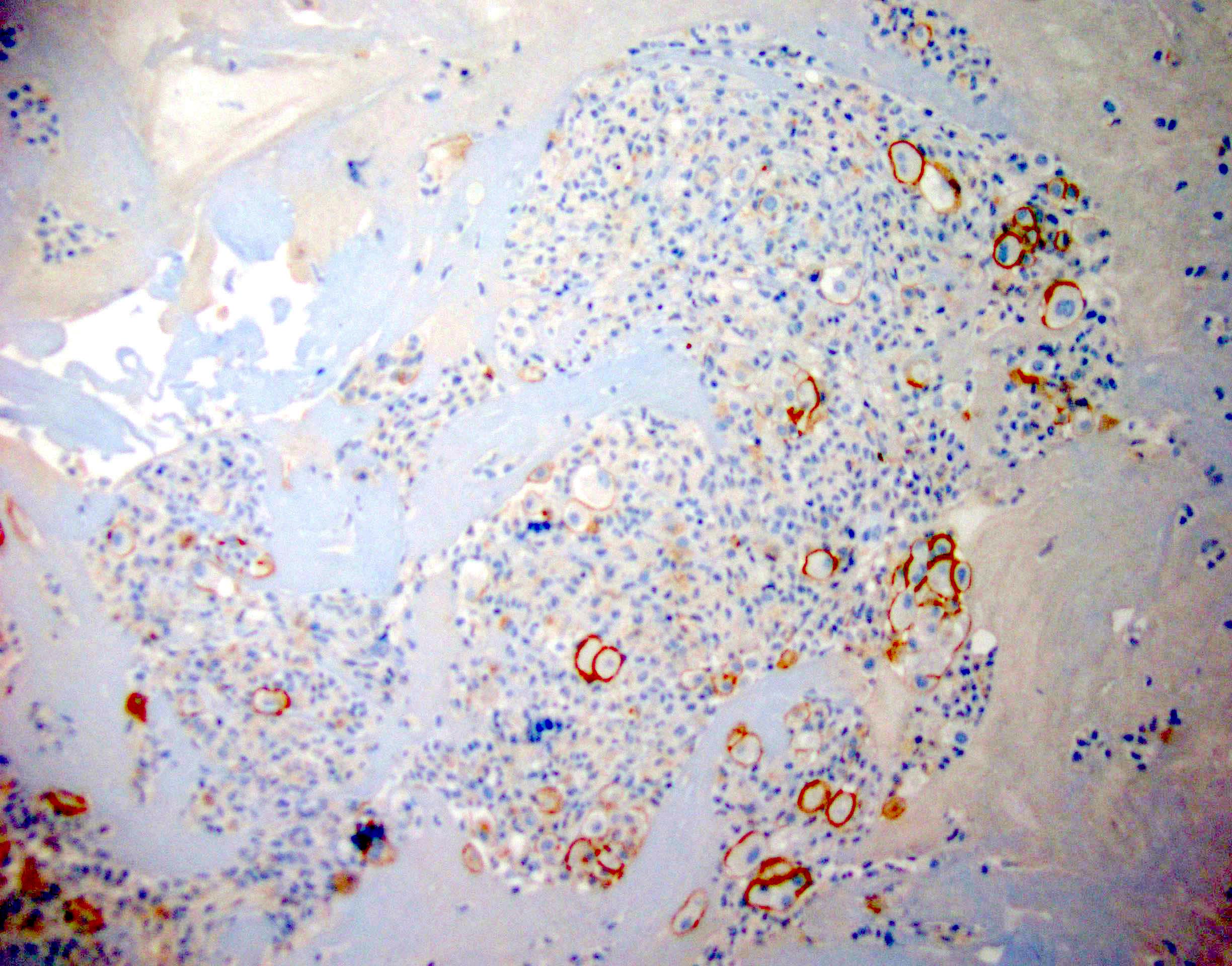
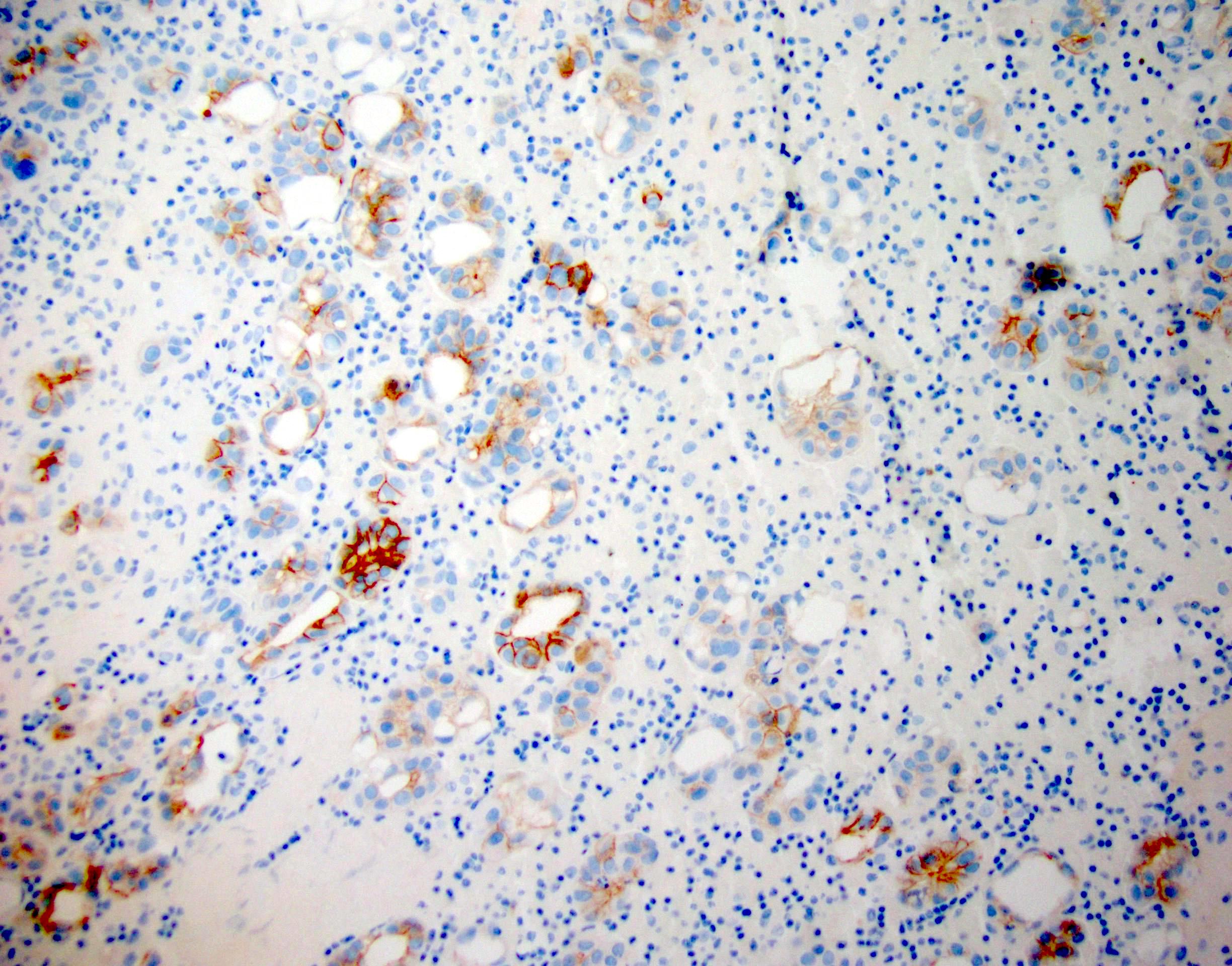
BerEP4 in pleural fluid
MOC31 in pleural fluid
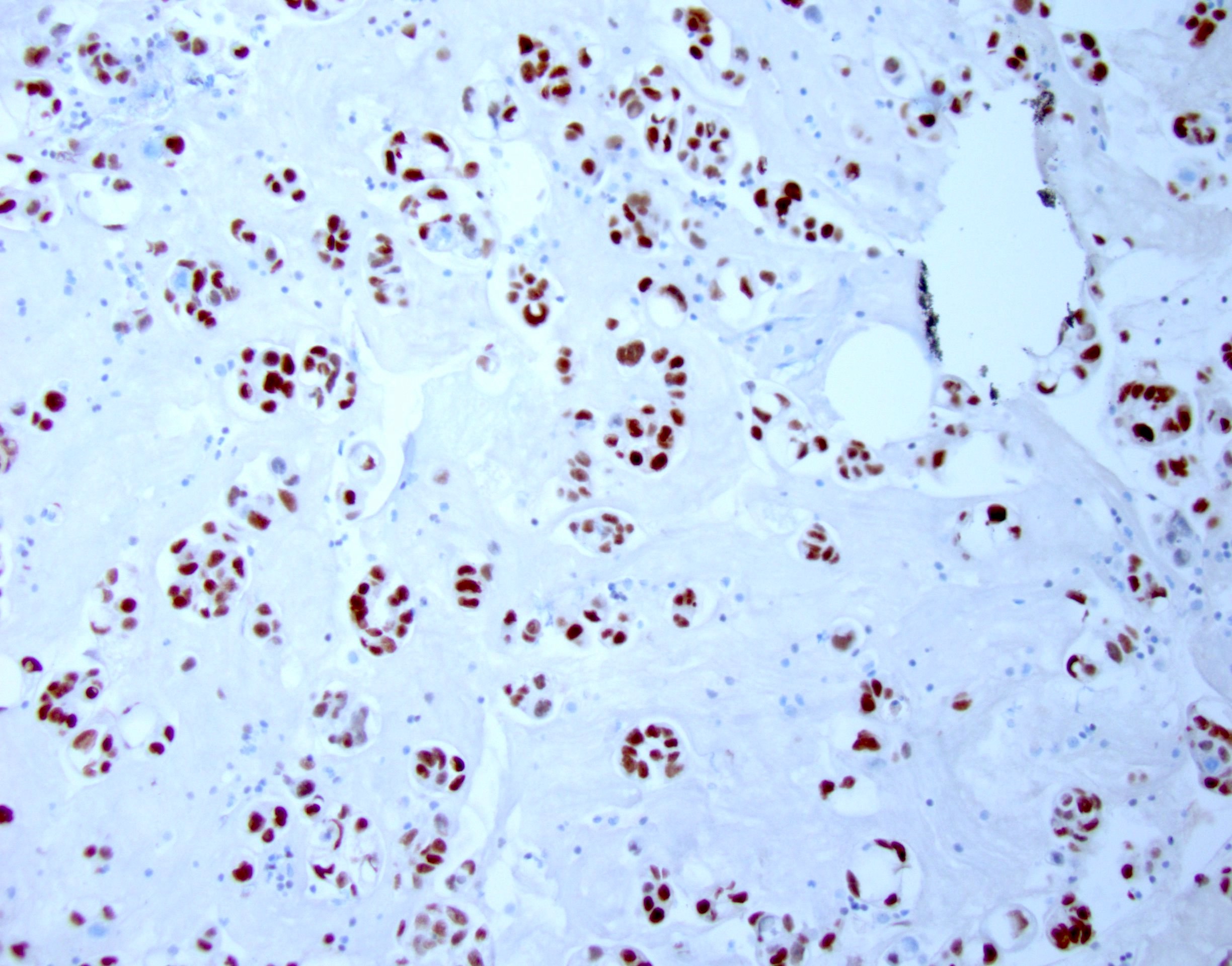
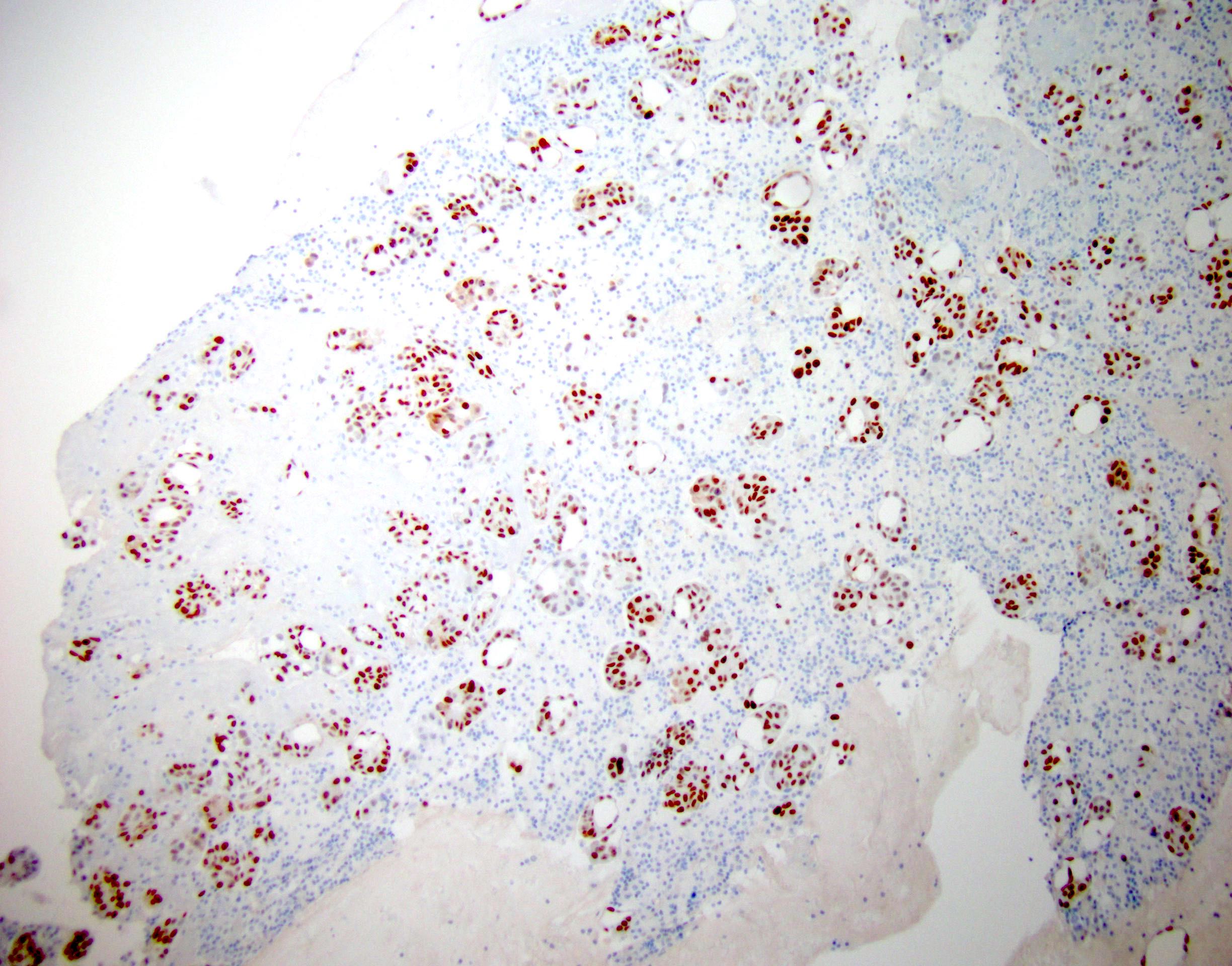
GATA3 in pleural fluid
PAX8 in pleural fluid
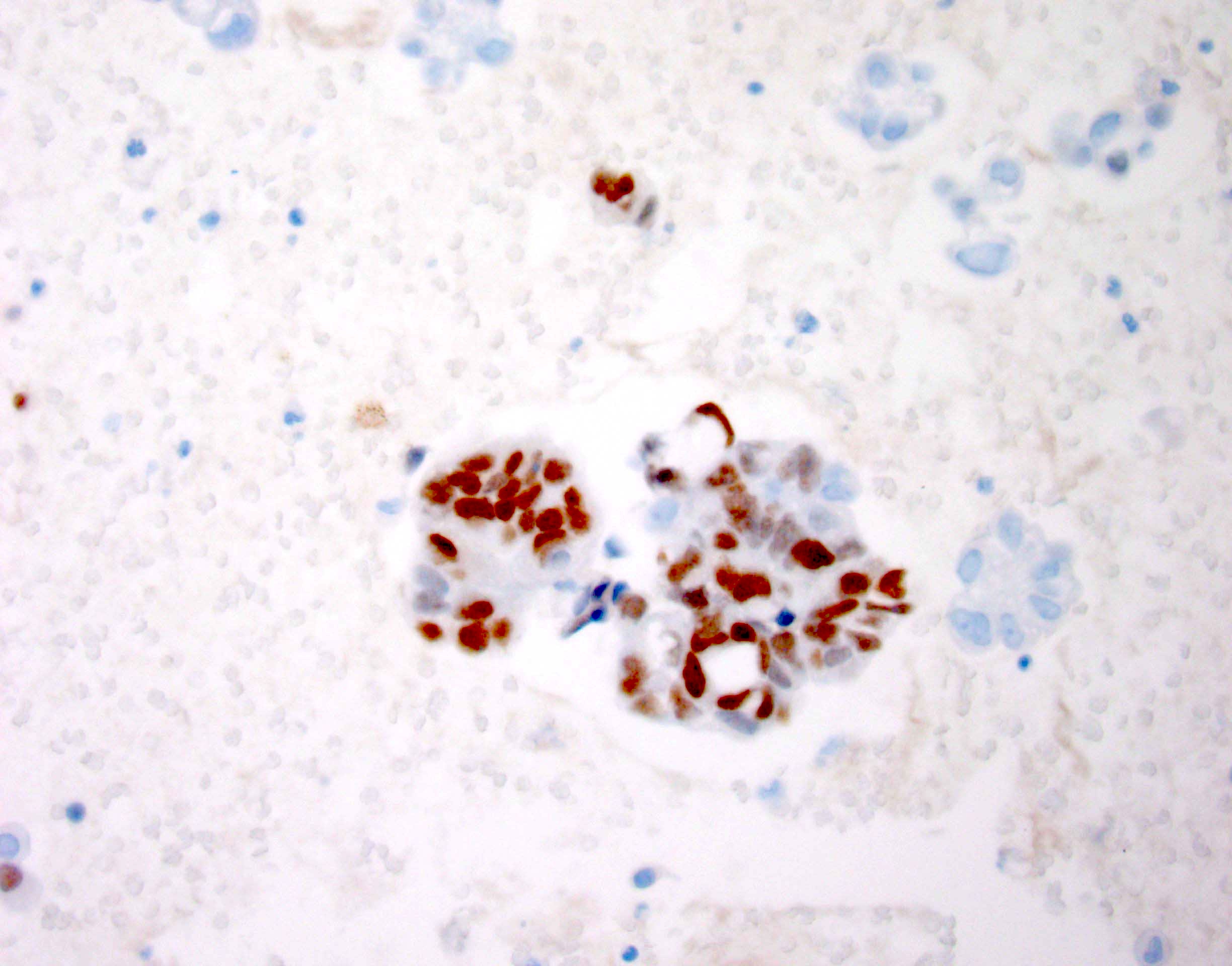
NKX3.1 in ascites
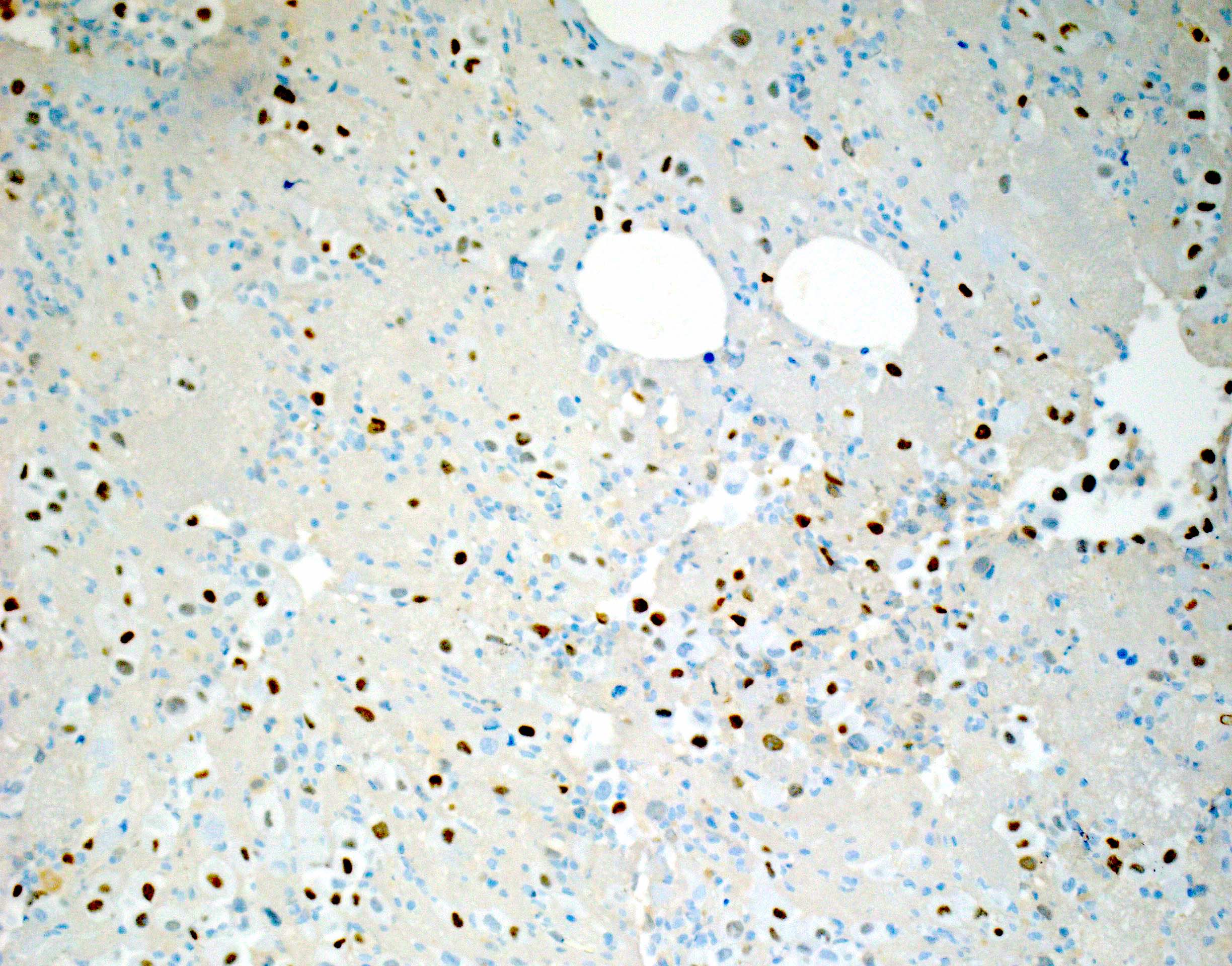
TTF1 in pleural fluid
Napsin A in pleural fluid

p40 in ascites

CDX2 in ascites
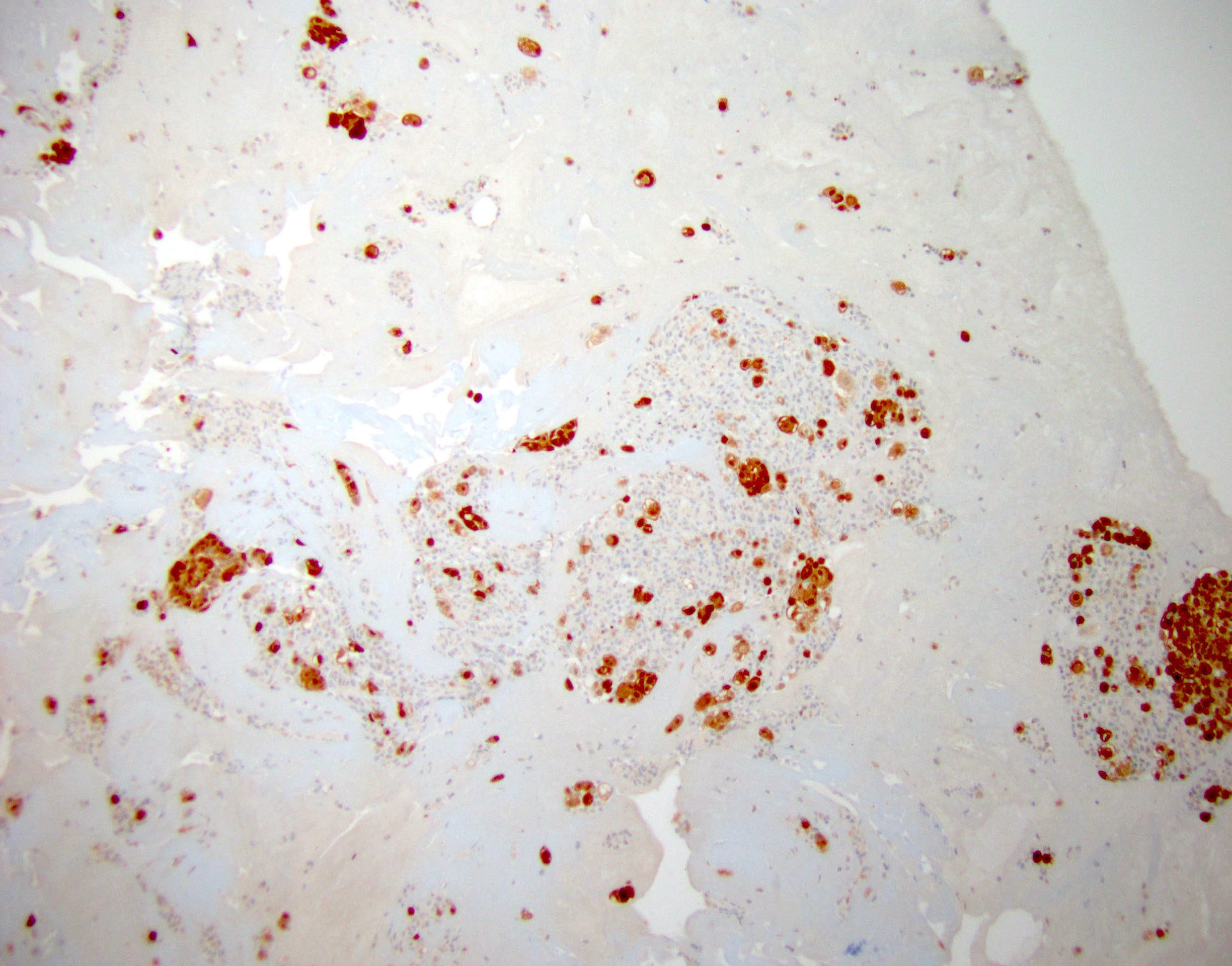
Calretinin in ascites
D2-40 in ascites

WT1 in ascites
ER in pleural fluid
HER2 in pleural fluid
Images hosted on other servers:

BAP1 in mesothelioma
Molecular / cytogenetics description
- p16 / CDKN2A deletion by fluorescent in situ hybridization (FISH) is found in up to 80% of malignant mesothelioma and can help differentiate it from reactive mesothelial cells (Cancer Sci 2015;106:1635)
Molecular / cytogenetics images
Images hosted on other servers:

p16 / CDKN2A deletion (FISH) in malignant mesothelioma

Absence of p16 / CDKN2A deletion by FISH
Additional references
Practice question #1

Which immunostaining panel is most helpful in the differential diagnosis of a 60 year old male patient with unilateral pleural effusion with the above findings from the pleural fluid cytology smear stained with Papanicolaou stain?
- AE1 / AE3, CAM5.2, CK7, CK20
- BerEP4, MOC31, calretinin, D2-40, TTF1
- BerEP4, MOC31, CK7, CK20, TTF1
- Calretinin, D2-40, WT1, AE1 / AE3, CAM5.2
- TTF1, synaptophysin, chromogranin, Ki67
Practice answer #1
Practice question #2
Which of the following immunostains can aid in the differentiation between a reactive mesothelial cells and mesothelioma?
- BAP1
- BerEP4
- Calretinin
- D2-40
- MOC31
Practice answer #2
