
Cytopathology
Cytopathology techniques
Rapid on site evaluation (ROSE)

Copyright: 2021-2025, PathologyOutlines.com, Inc.
PubMed Search: Cytopathology rapid on site evaluation
Cytopathology techniques
Rapid on site evaluation (ROSE)
Author: Austin B. Wiles, M.D.
Editorial Board Members: Bonnie Choy, M.D., Marc Pusztaszeri, M.D.
Last author update: 23 May 2022
Last staff update: 23 May 2022
Copyright: 2021-2025, PathologyOutlines.com, Inc.
PubMed Search: Cytopathology rapid on site evaluation

Table of Contents
Definition / general | Essential features | CPT coding | Sites | Diagrams / tables | Laboratory | Radiology description | Case reports | Molecular / cytogenetics description | Molecular / cytogenetics images | Sample pathology report | Differential diagnosis | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2 | Practice question #3 | Practice answer #3Cite this page: Wiles AB. Rapid on site evaluation (ROSE). PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/cytopathologyrose.html. Accessed September 25th, 2025.
Definition / general
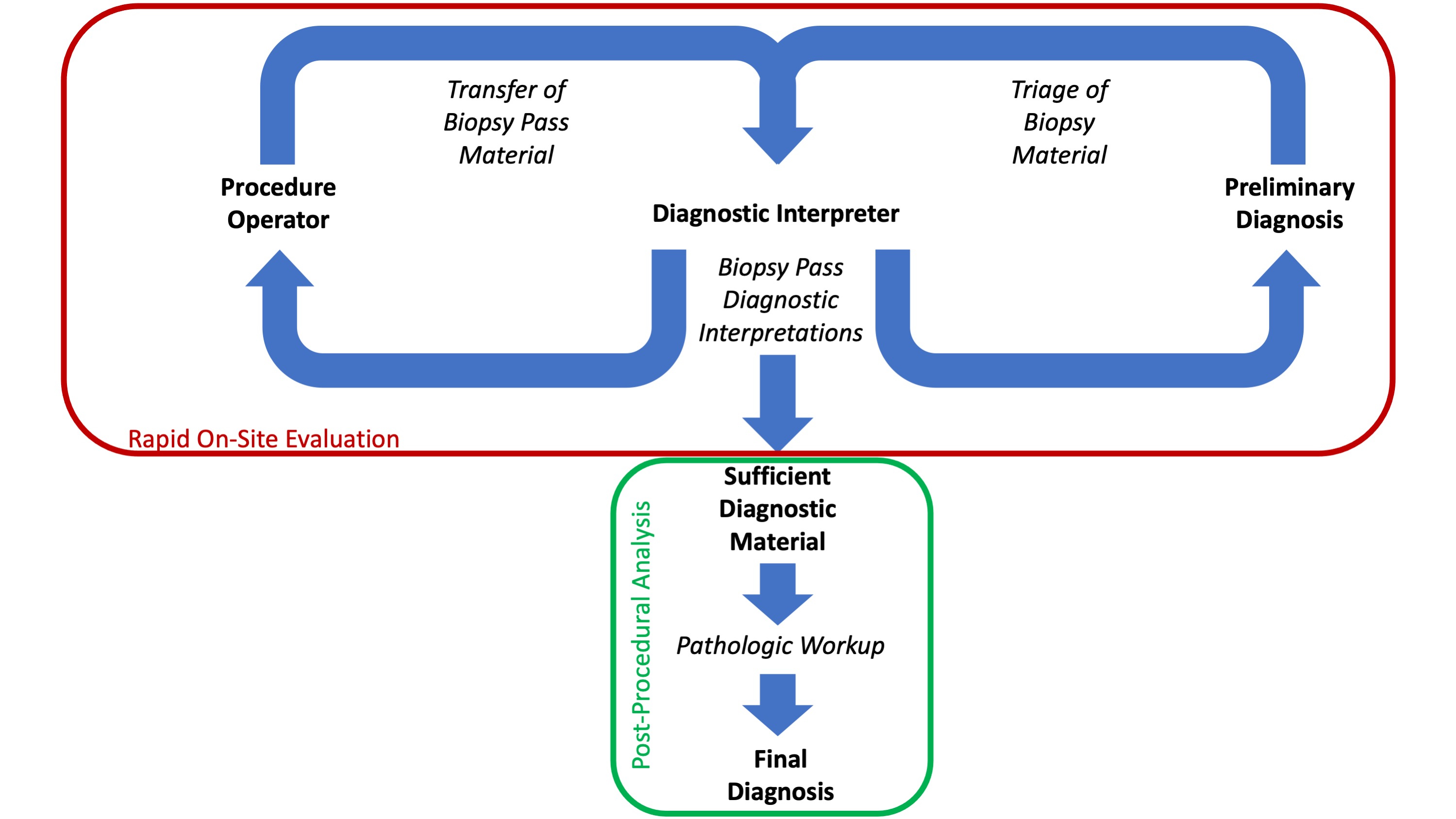
- Rapid on site evaluation (ROSE) is a cytopathologic diagnostic adequacy assessment of individual biopsy passes performed during a biopsy procedure in order to optimize the procedure itself and inform subsequent patient management
Essential features
- ROSE may be performed by a cytopathologist, a pathology trainee, cytotechnologist or clinical physician with sufficient training (Cytopathology 2020;31:303)
- A central goal of ROSE is to optimize the quantity of diagnostic material procured during a biopsy procedure including triage in anticipation of any ancillary studies (e.g., flow cytometry, molecular testing, etc.)
- ROSE specimens consist of aspirate smears from fine needle aspiration (FNA) biopsies or touch preparation slides from needle core (NC) biopsies (see smear making and special techniques for recovering and dividing aspirate material)
- ROSE diagnostic statements are performed for each examined biopsy pass and can be brief and categorical (i.e., adequate or nondiagnostic) or detailed and specific (i.e., favor squamous cell carcinoma), depending on the context
- Utility of ROSE: reduce the number biopsy passes, numbers of procedures and cost to obtain a final diagnosis
CPT coding
- Note 1: ROSE CPT codes for immediate adequacy interpretations may only be billed if the diagnosis is made by an attending pathologist
- Note 2: each different anatomical site for which ROSE is performed during biopsy is billed separately
- 88172 - aspirate smear, first pass
- 88177 - aspirate smear, all subsequent passes
- 88333 - touch preparation, first pass
- 88334 - touch preparation, all subsequent passes
Sites
- ROSE may be performed during cytology biopsy procedures from any anatomic site
- Content of a ROSE statement may be dependent on the institution, anatomic site, presumptive diagnosis, biopsy operator and pathologist
Diagrams / tables


Laboratory
- ROSE can optimize the performance of biopsy procedures benefitting the patient in 3 general capacities:
- Reducing the number of passes made during a biopsy procedure and the overall number of procedures necessary to obtain a treatable diagnosis (Cancer Cytopathol 2013;121:518)
- Informing the efficient disposition of cellular material for subsequent diagnostic and ancillary testing, including obtaining sufficient material necessary for anticipated diagnostic immunohistochemical studies, flow cytometry and theragnostic molecular testing (Cancer Cytopathol 2013;121:544)
- Performance of ROSE can reduce the cost to obtain a diagnosis depending on a number of factors, including the availability of equipment, laboratory staff and procedure frequency (PLoS One 2015;10:e0135466)
- Utility of ROSE may be limited in some circumstances:
- Cysts: only small volumes of cyst fluid may be analyzed generally obviating the utility of ROSE (Cibas: Cytology - Diagnostic Principles and Clinical Correlates, 5th Edition, 2021)
- Solid pancreatic lesions sampled via needle core biopsy (Surg Endosc 2017;31:225)
- Core depletion: depletion of diagnostic material from needle cores due to improper touch preparation technique (J Am Soc Cytopathol 2020;9:322)
- Pathology ancillary studies prompted by ROSE may include:
- Recording formalin fixation time for lesions of suspected breast origin (Am J Clin Pathol 2018;149:275)
- Molecular testing (Curr Oncol 2017;24:103, Acta Cytol 2016;60:372)
- Microbiological cultures (Cancer Cytopathol 2018;126:643, Cancer Cytopathol 2015;123:612)
- Flow cytometry (Acta Cytol 2016;60:302)
- There is no standard staining protocol for performing ROSE but maintenance of the stain line should occur according to laboratory standards
- Diff-Quik Romanowsky stain is commonly used for ROSE slides (CAP Today: Cytopathology and More | FNA Cytology - Rapid On-Site Evaluation - How Practice Varies [Accessed 20 December 2021])
- Rapid or ultrafast Papanicolaou, toluidine blue, rapid hematoxylin and eosin stains or brilliant cresyl blue may be used (J Cytol 2012;29:241, J Int Med Res 2019;47:626, Diagn Cytopathol 2019;47:469)
- ROSE can be performed via telepathology following validation (Diagn Cytopathol 2019;47:206, Cytopathology 2020;31:402)
- Equipment necessary for a ROSE procedure:
- Adequate workspace
- Disposable workpad (i.e., Chux pad)
- Microscope
- Power source for microscope
- Stain line
- Coplin jar
- Pencil and pencil sharpener
- Blank slides
- Slide box
- RPMI tubes and holders
- Formalin jars
- Needles for manipulating tissue
- Steel needle holder
- Needle disposal box
- Biohazard trash receptacle
- Cleaning supplies
- Secure storage
- Note 1:
- Equipment may be brought by the pathologist or stored in the procedure room
- All equipment must be maintained according to accreditation protocols regardless of its storage site
- Note 2: see Diagrams / tables for a depiction of a portable cart containing all the above items
- Personnel:
- ROSE may be provided by a single pathologist
- An assistant may be very useful, as they can work on preparing slides while the pathologist renders interpretations
Radiology description
- ROSE can be performed in conjunction with any radiological modality incorporated into the biopsy procedure
Case reports
- 19 year old man with early cytologic diagnosis of cysticercosis using ROSE (IDCases 2018;15:e00477)
- 65 year old woman diagnosed with sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman-Destombes disease) using ROSE (Eur J Med Res 2021;26:34)
- 65 year old man with respiratory failure and metastasis of renal cell carcinoma diagnoses using endobronchial ultrasound guided transbronchial needle aspiration using ROSE (Respir Med Case Rep 2020;29:101028)
Molecular / cytogenetics description
- Molecular testing, including next generation sequencing (NGS) and microRNA classifier assessments, may be performed on uncoverslipped, stained aspirate smears with adequate cellularity of diagnostic material (Diagn Cytopathol 2019;47:469, Arch Pathol Lab Med 2018;142:291)
Molecular / cytogenetics images
Images hosted on other servers:

NGS analysis on smears
Sample pathology report
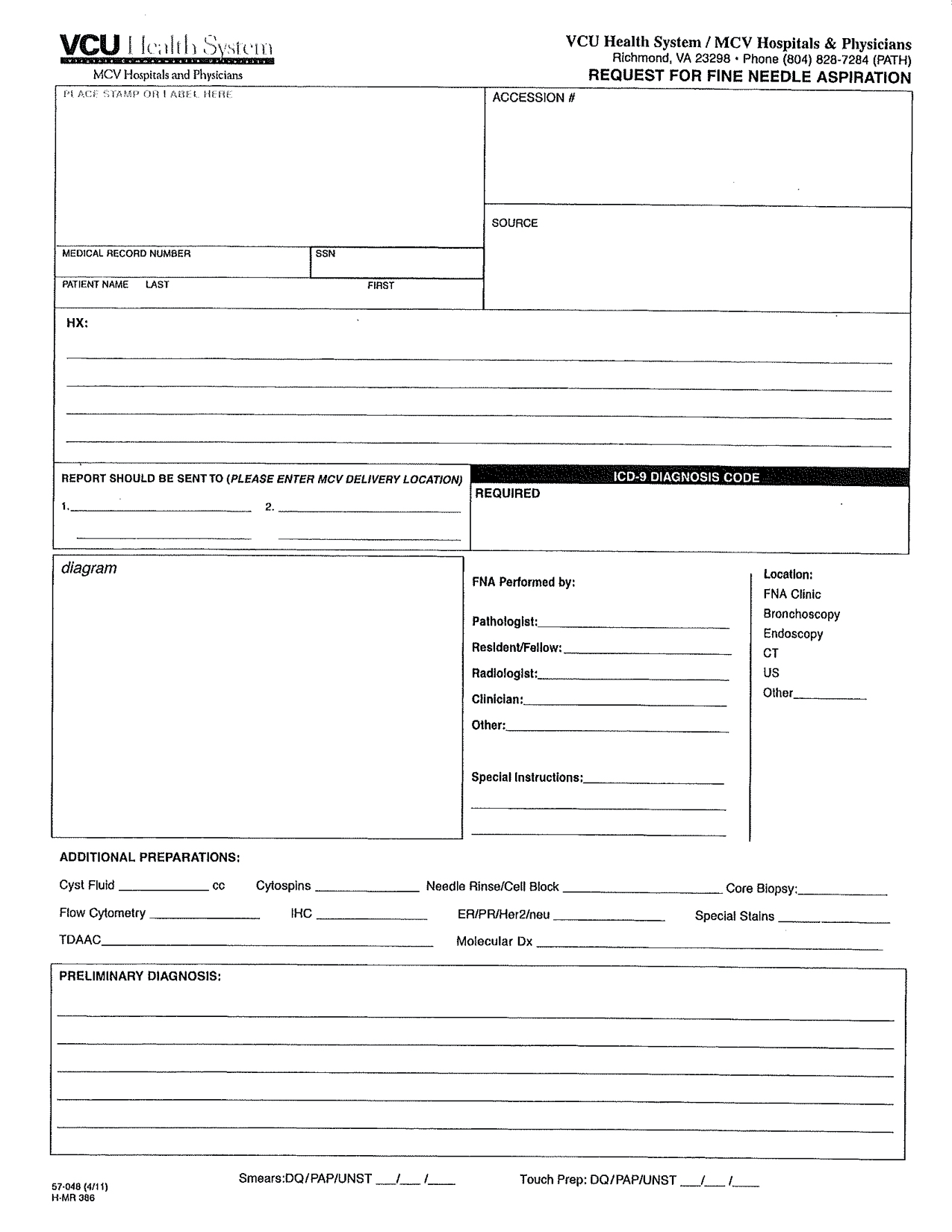
- See Diagrams / tables for a sample blank report form containing all necessary elements for an ROSE procedure
- ROSE pathology reports should be designated as provisional or preliminary in the patient record
- Nodule, inferior right lobe, thyroid, ultrasound guided fine needle aspiration biopsy:
- Pass 1 (aspirate smear): adequate follicular cells and colloid
- Mass, liver, CT guided fine needle aspiration and needle core biopsy:
- Pass 1 (aspirate smear): hepatocytes and blood
- Pass 2 (aspirate smear): malignant cells present
- Pass 3 (touch preparation): malignant cells present
- Passes 3, 4 and 5 were placed directly in formalin for anticipated ancillary diagnostic studies
- Lymph node, station 7, endobronchial ultrasound guided fine needle aspiration biopsy:
- Pass 1 (aspirate): blood and bronchial cells
- Pass 2 (aspirate): lymphoid elements, rare epithelioid histiocytes
- Pass 3 (aspirate): noncaseating granulomas
- Pass 4 (aspirate) was sent for culture by the clinician
- Passes 5 and 6 were placed directly in RPMI for anticipated ancillary diagnostic studies
- Mass, pancreas, endoscopic ultrasound guided fine needle aspiration biopsy:
- Pass 1 (aspirate): nondiagnostic, predominately GI contaminant
- Pass 2 (aspirate): atypical cells present
- Pass 3 (aspirate): atypical cells present
- Pass 4 (aspirate): diagnostic material present
Differential diagnosis
- ROSE preliminary diagnoses can be generally categorized:
- Nondiagnostic or inadequate:
- Material present on slides is not consistent with a definitive final diagnosis
- Diagnostic or adequate:
- Material present on the slides is diagnostic of some process
- This may or may not include malignant diagnoses
- Atypical:
- Cytologic features are present that may or not be associated with a pathologic process
- Both reactive and neoplastic entities may be suggested by this category
- Suspicious:
- Cytologic features suspicious but not definitive for malignancy, are present
- Malignant:
- Cytologic features present on the slides is consistent with a malignant process
- Nondiagnostic or inadequate:
- ROSE diagnostic classifications are generally very reliable when compared to the final diagnosis; concordance with the final diagnosis is not guaranteed, with false negatives being the more common error (J Am Soc Cytopathol 2014;3:67, Diagn Cytopathol 2019;47:367)
Practice question #1
A radiologist performs an ultrasound guided fine needle aspiration biopsy of a liver mass obtaining 4 passes from a single anatomic site. Aspirate smears from each pass were evaluated by an attending pathologist during rapid on site evaluation (ROSE). A preliminary interpretation was given to the radiologist for each pass and was subsequently recorded in the patient record in a preliminary report. What CPT codes are appropriate for the ROSE portion of this procedure?
- 88172x1 and 88177x3
- 88172x4
- 88307x1
- 88333x1 and 88334x3
- 88333x4
Practice answer #1
Practice question #2
A radiologist performs a CT guided needle core biopsy of a soft tissue mass present in the quadriceps muscle of a patient obtaining 3 passes. Each needle core is transferred to an attending pathologist during rapid on site evaluation (ROSE). The pathologist gently manipulates each needle core on a glass slide to produce touch preparations and then transfers them to a formalin container for posterior processing in the cytology laboratory. Following staining an examination of the touch preparation slides, a preliminary interpretation of "scant spindle cells and blood" is provided to the radiologist following each pass. These results were recorded in the patient record in a preliminary report. Examination of the formalin fixed, paraffin embedded needle core tissue with H&E demonstrates a schwannoma which correlates well with the clinical and radiological impression. No immunohistochemical studies were necessary to produce the final diagnosis. What CPT codes should be applied to this pathology case?
- 88172x1, 88177x2, 88305x1
- 88172x3, 88305x1
- 88307x1
- 88333x1, 88334x2, 88307x1
- 88333x3, 88307x1
Practice answer #2
D. 88333x1, 88334x2, 88307x1 (see CPT coding)
Comment Here
Reference: Rapid on site evaluation (ROSE)
Comment Here
Reference: Rapid on site evaluation (ROSE)
Practice question #3
The practices and terminologies used to perform rapid on site evaluation (ROSE) are
- Delineated by CLIA '88 and the College of American Pathologists
- Regulated and informed by standards established by the American Society of Cytopathology
- Universal and standardized
- Vary widely between institutions
Practice answer #3
D. Vary widely between institutions. The practice, terminologies and equipment to perform ROSE vary widely between institutions and may even vary within institutions depending on the specific needs of clinical practices. Variation is influenced by organ site, clinical capabilities, local convention and individual judgement of the ROSE provider.
Comment Here
Reference: Rapid on site evaluation (ROSE)
Comment Here
Reference: Rapid on site evaluation (ROSE)
