
Autopsy & forensics
General
Brain contusions
Authors: Michel Tawil, M.D., Christine E. Fuller, M.D.
Resident / Fellow Advisory Board: Lorenzo Gitto, M.D.
Deputy Editor-in-Chief: Patricia Tsang, M.D., M.B.A.


Last author update: 14 March 2023
Last staff update: 14 March 2023
Copyright: 2021-2025, PathologyOutlines.com, Inc.
PubMed search: Brain contusions

Table of Contents
Definition / general | Essential features | Terminology | Epidemiology | Pathophysiology | Radiology description | Gross images | Microscopic (histologic) images | Autopsy findings | Medicolegal considerations | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Tawil M, Fuller CE. Brain contusions. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/forensicsneuropathologycontusions.html. Accessed August 26th, 2025.
Definition / general
- Focal injuries to the brain occurring at locations where brain tissue directly impacts against the inner skull / bony protuberances
- Bleeding is a result of the damage to the small caliber blood vessels (Handb Clin Neurol 2015;127:45)
Essential features
- Contusions are observed where there is direct impact of brain against bony surfaces of the inner aspect of skull
- Can bleed into the cerebrospinal fluid (CSF), causing subarachnoid hemorrhage
Terminology
- Coup contusion: contusion occurring at site of impact
- Contrecoup contusion: contusion at site separate from impact site
- Generally related to differential movement of brain within the skull, leading to contusion at areas of bony prominences
- Regions with highest frequency of contusions: orbital frontal, frontal and temporal poles, cortex near the Sylvian fissure
Epidemiology
- More prevalent in males with ratios from 1.5:1 to 2.5:1 across the world (J Med Life 2015;8:272)
- Highest rate occurs between the ages of 15 - 24 years (PLoS One 2020;15:e0229489)
- 20 - 30% of the elderly who fall suffer moderate to severe injuries besides contusions and traumatic brain injury (WHO: Falls [Accessed 22 November 2022])
Pathophysiology
Brain contusions due to blows (impacts)
Brain contusions due to falls
Gliding contusions
Fracture contusions (Curr Neuropharmacol 2020;18:538)
Theories that explain the formation of contrecoup contusions
Dating contusions (Open Access Maced J Med Sci 2017;5:813)
- A blow is defined as an impact to a head by a load delivered by a hard object
- Several classes are defined based on kinetic energy and the inertia (or movement) of the involved head:
- Blows producing small amounts of energy that slightly rotate the head
- Examples include lightweight objects such as stones
- Produce abrasions or lacerations of the scalp with or without subgaleal hemorrhage; no fractures or brain injury (J Neurotrauma 2012;29:19)
- Blows that produce more kinetic energy and approach the head at an equal or greater speed (Front Neurol 2015;6:89, StatPearls: Blunt Force Trauma [Accessed 3 March 2023])
- Examples include hollow steel pipes, police night sticks, beer bottles
- Deform the skull, which moves / impacts the brain underneath the impact site
- Single (or multiple) cone shaped lesions beneath the impact site, with the base at the skull and apex within brain parenchyma
- May present as a superficial lesion confined to the cortex or as a deeper lesion with more extensive hemorrhage
- Blows that happen in the course of falling (StatPearls: Blunt Force Trauma [Accessed 3 March 2023])
- Examples include striking the head on a table edge
- May show scalp abrasion or laceration, subgaleal hematoma and contusions, with or without skull fractures
- Hard to interpret without sufficient background information
- Blows with momentum greater than the inertia of the head (Front Neurol 2015;6:89)
- Examples include weighted pipes, two by fours, metallic baton, heavy duty flashlight, baseball bat
- Forces produced by the impact to the head approximate those of falls
- They deform the skull with or without fractures and may produce coup and contrecoup contusions or contrecoup contusions only
- May be difficult to interpret and should be interpreted within the context of witness accounts and scene inspection
- Blows where the velocity and mass of the object are much greater than the head or the fixed head is struck with an object with a much greater momentum
- Skull is shattered without any significant contusions
- Rare instances where the brain is thrown from the skull while still intact
- Miscellaneous
- Blows at the top of the head
- No surface contusions
- Produce pattern of internal cerebral trauma
- Acceleration type of injury to the centroaxial region of the brain within an enclosed cranium (Handb Clin Neurol 2015;127:45)
- Tangential blows to the head
- Blows at the mandibular condyles
- These lesions involve inner cerebral contusions to the corpus callosum, white matter hemorrhages, avulsions of the choroid plexus and hemorrhages into the tela choroidea
- Blows at the top of the head
- Blows producing small amounts of energy that slightly rotate the head
Brain contusions due to falls
- Tend to produce a contrecoup contusion, as the brain is in motion and then abruptly stops in the course of the fall
- Falls that impact the occiput of the head will have contrecoup contusions at the base of the skull (J Med Case Rep 2018;12:166)
- If impact is on the lateral side of the head, the contusion may be seen on the opposite surface but the impact site will most likely be cushioned by the shoulders so as to decrease its intensity
- Frontal impact contrecoup are uncommon (J Neurotrauma 2016;33:1034)
- Front of the cranium absorbs the energy produced by the impact → no dissipation of energy into the brain parenchyma
- Motor vehicle accident victims that are driven into windshields of their cars will most likely use their hands to protect themselves as a reflex, thus cushioning the impact
- Lateral falls will be cushioned by the shoulders absorbing all the energy
- Falls that impact the inferior portion of head (e.g., mandible), may produce contrecoup contusions at the vertex of the brain (Radiographics 2019;39:1571)
Gliding contusions
- Hemorrhagic lesions within parasagittal white matter in superior cerebral areas; frequently bilateral
- Accompany traumatic axonal injury (Arch Pathol Lab Med 1986;110:485, Front Neurol 2016;7:178)
Fracture contusions (Curr Neuropharmacol 2020;18:538)
- Fracture line produced by an impact injury can rub against the underlying brain parenchyma causing a contusion
- Typically associated with basilar skull fracture
Theories that explain the formation of contrecoup contusions
- Vibration theory (J Neurotrauma 2005;22:845)
- Impact to the skull creates vibrations that travel throughout the brain
- These vibratory waves hit the skull on the other side with a large magnitude, fracturing the skull and damaging the brain
- Transmitted force wave theory
- Wave generated by the impact can be strong enough to produce a vacuum at the impact point, leading to disruption of blood vessels, damage to the brain parenchyma and the contrecoup phenomenon (Arch Surg 1965;90:157)
- Brain displacement theory (Neurocrit Care 2004;1:385)
- Brain is mobile within the skull and thus its own momentum can lead to tearing of the brain from its own attachments thus causing damage
- Skull deformation theory (Nihon Hoigaku Zasshi 1993;47:387)
- Combination of brain displacement and skull deformation results in the brain being contused
- Pressure gradient theory
- Movement between the brain and a skull produces intracranial cavitation due to focal, nonuniform pressure gradient (Nihon Hoigaku Zasshi 1993;47:387)
- Rotational shear force theory
- Rapid rotations of the head generate shear forces throughout the brain and therefore have high potential to cause shear force induced brain tissue damage (Clin Sports Med 2011;30:19)
Dating contusions (Open Access Maced J Med Sci 2017;5:813)
- Early reactions
- Edema
- Starts within minutes of injury
- Increases within hours and plateaus over days
- Disappears within 6 days (Vet Pathol 2016;53:962)
- Hemorrhage
- Microscopically starts and expands within hours around perivascular areas
- Maximal accumulation is reached within 24 hours
- Intact red blood cells remain viable for 5 - 6 months postinjury (Forensic Sci Med Pathol 2008;4:187)
- Polymorphonuclear leukocytes
- Starts within hours of the injury
- May be visible for up to a month postinjury, with or without infection
- Degenerating neurons (Toxicol Pathol 2011;39:22)
- Appear within 2 hours
- Characteristic red neurons (= shrinkage, eosinophilic cytoplasm, pyknosis)
- Not very prominent neuronophagia (phagocytosis of dying neurons by microglial cells) may remain in the lesion
- Edema
- Macrophages and scavenger cells
- Start within 24 hours postinjury, plateau at 7 - 14 days and then decrease
- Become distended with fatty granules due to phagocytosis of red cells and degenerate cellular material
- Hemosiderin and siderophages
- Hemosiderin laden macrophages appear as early as 5 days postinjury and may last for years
- Due to iron containing residue of hemoglobin from degenerate red blood cells
- Hematoidin pigment
- Yellow-orange crystallized bilirubin derived from hemoglobin breakdown
- Appears 10 - 12 days postinjury
- Absorbed within a few months due to its high solubility
- May persist for years within hemorrhagic lesions (Blood 2014;124:2158)
- Intermediate and late reactions
- Vascular reactions (J Neuropathol Exp Neurol 1999;58:153)
- Angiogenesis starts 5 - 7 days postinjury and plateaus at 3 weeks
- Residual tissue is made up of a mixture of small and sclerotic vessels
- Astrocytic reaction
- Protoplasmic astroglial proliferation starts 4 - 5 days postinjury
- Fibrillary astroglial proliferation starts 7 - 10 days postinjury
- Eventually forms a glial scar (a focus of increased proliferation of glial cells)
- Believed to be a type of reactive gliosis to restore the blood brain barrier
- Vascular reactions (J Neuropathol Exp Neurol 1999;58:153)
- Collagen production and fibrosis (Stem Cell Res Ther 2014;5:122)
- Rarely occurs in the CNS as a reparative mechanism unless the injury occurred at the cortical surface or when many small vessels are involved
- Fibroblasts appear within a week and can persist for months and years
- Microscopically the lesion ultimately resembles an old infarct
Radiology description
- CT imaging (J Stroke 2017;19:11)
- Small foci of petechial hyperdensity involving the gray matter and subcortical white matter
- Large cortical or subcortical bleed
Gross images
Contributed by Michel Tawil, M.D.

Cortical surface
Microscopic (histologic) images
Contributed by Michel Tawil, M.D.
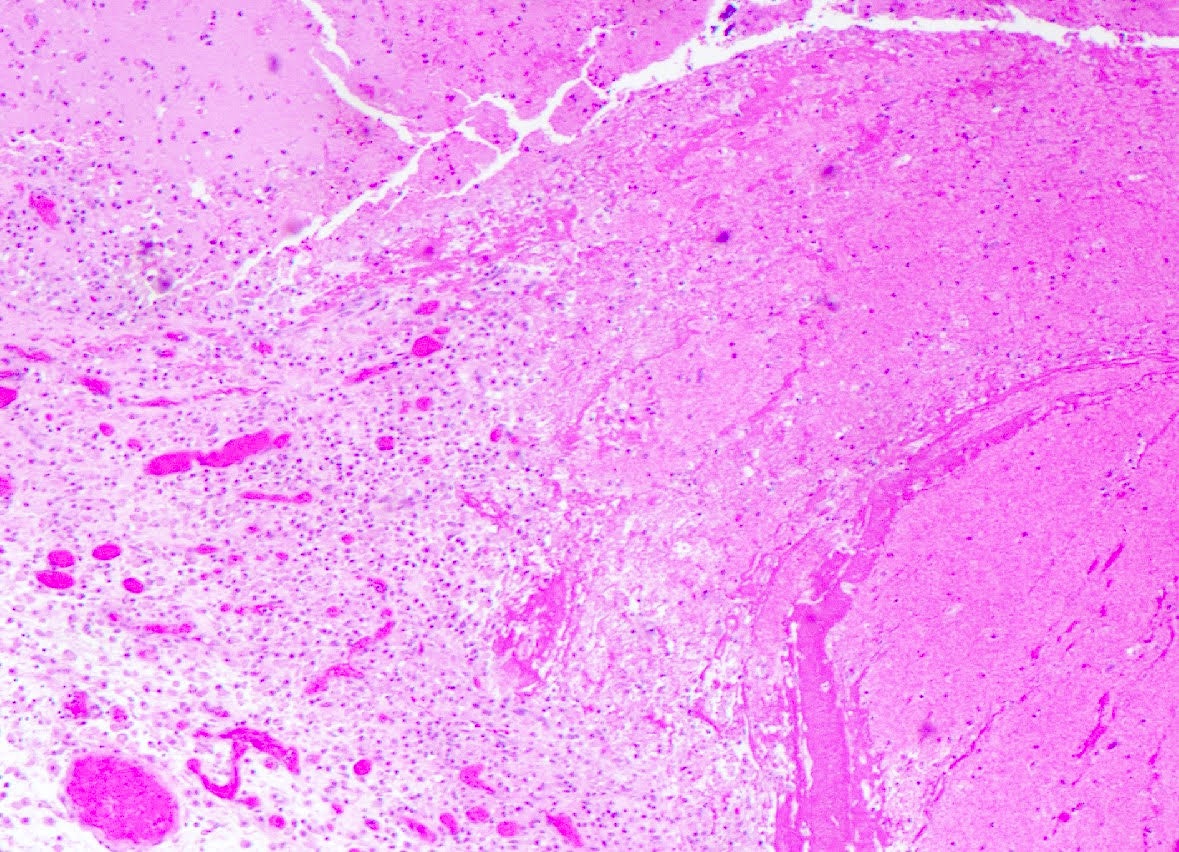
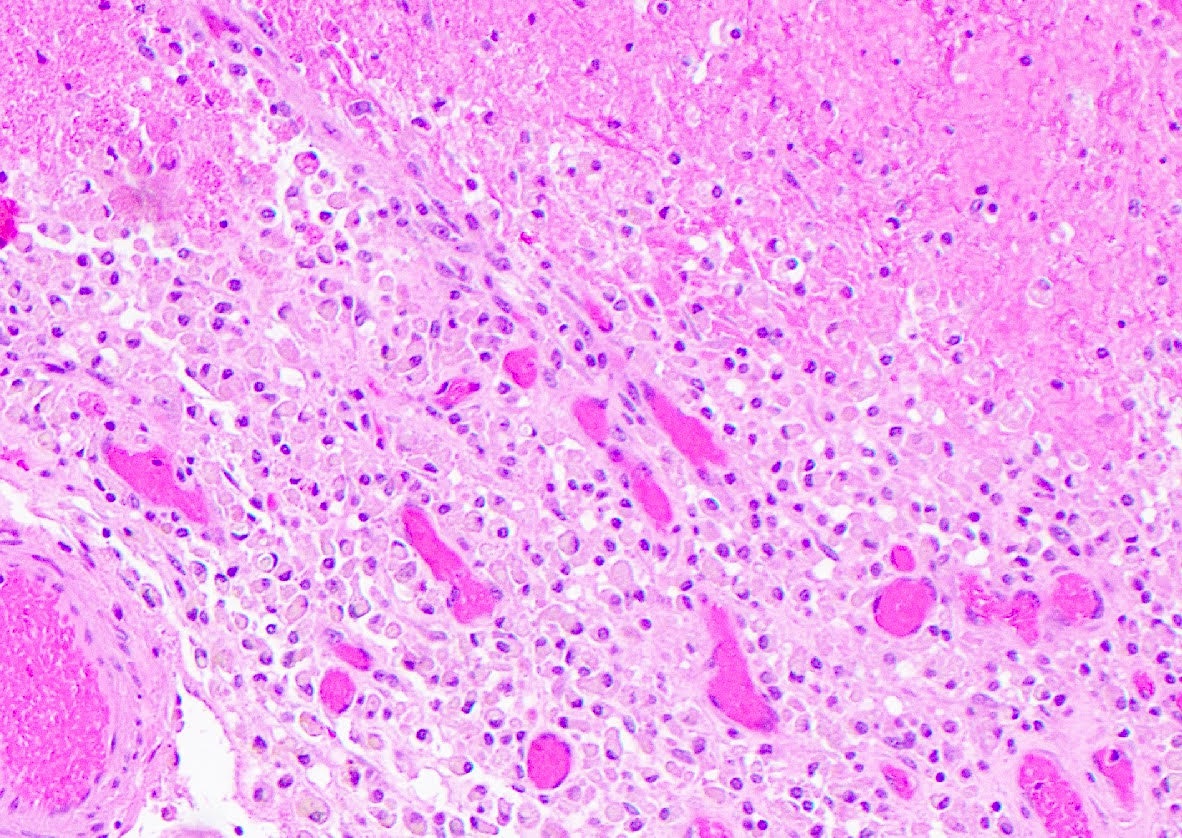
Sections from frontal lobe
Autopsy findings
- Coup contusions (J Emerg Trauma Shock 2018;11:205)
- Classically, are found over the cerebral or cerebellar hemispheric surfaces, especially the gyral crests
- Earliest manifestation is a focal discoloration or bruise on the surface of the cortex, appearing as a cone with its base at the gray matter and fading into the white matter
- With the passage of time contusions undergo reparative changes, sometimes with parenchymal collapse and gliosis
- Contrecoup contusions (Pediatr Radiol 2014;44:S632)
- Occur at surface of gyri and spare the sulci
- Occur at sites distant from initial impact to the head (most frequently in orbitofrontal or temporal tip regions)
- Like coup contusions, they undergo reparative changes and parenchymal collapse / gliosis as time passes
- Older contusions have a sunken tan-brown lesion with a serpentine appearance that follows the crests of the gyri
- Differentiated from infarcts based on the following:
- They do not follow a particular vascular distribution
- Brain will adhere to dura if contusion is extensive or has been surgically manipulated
- Underlying white matter might show demyelination and pallor
- Gliding contusions
- Intraparenchymal hemorrhages within parasagittal cerebral white matter, typically with accompanying traumatic axonal injury (Arch Pathol Lab Med 1986;110:485)
- Fracture contusions
- Appear more like lacerations
- They follow fracture lines
- May involve multiple gyri
- Can be associated with abscess if the fracture passed through a paranasal sinus
- Appear more like lacerations
- Contusional tears (Curr Neuropharmacol 2020;18:538)
- Mostly seen in infants
- Infant's brain is largely made of water and encased within a malleable nonossified cranium
- Does not develop contusions but rather necrosis and hemorrhage in the subcortical matter, that might be mistaken for congenital cysts or artifacts
- Produces a slit-like lesion underneath the vertex of brain
- Mostly seen in infants
Medicolegal considerations
- Blow contusions that indent the skull might deform the underlying brain cortex, deep into the sulci instead of superficially on the gyri
- These blows are uncommon and mostly seen when a hammer is used to strike the head or in crush scenarios
- Contrecoup contusions produced by falls are almost always accompanied by coexisting injuries due to shearing and torsional forces (e.g., inner cerebral trauma, traumatic axonal injury) and subdural or epidural hemorrhages (Neurocrit Care 2004;1:385)
- Contusional tears can be a potential marker of nonaccidental trauma / child abuse or when an adult crushes a child during a fall (AJNR Am J Neuroradiol 2016;37:163)
Additional references
Practice question #1

The image shown above is that of a traumatic brain injury. Which of the following statements is true in reference to the lesions present?
- They always result in loss of consciousness
- They are most likely the direct result of a skull fracture
- They are the result of the differential movement of the brain inside of the skull in acceleration / deceleration head injury
- They are the result of uncal herniation
- They could never have resulted from closed head injury alone
Practice answer #1
C. They are the result of the differential movement of the brain inside of the skull in acceleration / deceleration head injury. This image shows coup and contrecoup contusive injury due to an acceleration / deceleration head injury, in which there was a resultant differential movement of the brain inside of the skull. Closed head injury alone could cause this pattern of injury and it is not the result of uncal herniation. One could have a contusion beneath a skull fracture but you would need multiple (bilateral) skull fractures to cause the amount of injury shown here. This patient may or may not have lost consciousness; it would depend upon whether they had diffuse axonal injury in addition to these contusions.
Comment Here
Reference: Brain contusions
Comment Here
Reference: Brain contusions
Practice question #2
A large contrecoup contusion is most likely to be encountered in which of the following scenarios?
- 18 year old man who was struck in the head with a baseball bat
- 30 year old man with a history of trisomy 21
- 44 year old woman who struck her head on a tree while skiing and was lucid for 30 minutes before collapsing
- 55 year old man who fell off a ladder, striking the occipital skull
- 80 year old woman with progressive memory decline over the past 10 years who recently fell out of bed at a nursing home
Practice answer #2
D. 55 year old man who fell off a ladder, striking the occipital skull. Trauma with a contrecoup cerebral contusion that is larger than the coup contusion is associated with a stationary object and a moving head, especially a fall from a height (choice D). Choice A would likely result in a larger coup injury, choice C would likely result in an epidural hemorrhage and choice E would likely result in a subdural hematoma.
Comment Here
Reference: Brain contusions
Comment Here
Reference: Brain contusions
