Skin nonmelanocytic tumor
Benign (nonmelanocytic) epidermal tumors or tumor-like lesions
Epidermolytic acanthoma
Authors: Simon F. Roy, M.D., Jennifer M. McNiff, M.D.
Resident / Fellow Advisory Board: Caroline I. Mullins, M.D.
Editorial Board Member: Kiran Motaparthi, M.D.


Last author update: 18 October 2021
Last staff update: 25 April 2022
Copyright: 2021-2025, PathologyOutlines.com, Inc.
PubMed Search: Epidermolytic acanthoma
Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Videos | Sample pathology report | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Roy SF, McNiff JM. Epidermolytic acanthoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skintumornonmelanocyticepidermolyticacanthoma.html. Accessed October 3rd, 2025.
Definition / general
- Cutaneous acanthotic benign lesion with epidermolytic hyperkeratosis spanning more than 50% of its surface
Essential features
- Solitary or multiple lesions with acanthosis and epidermolytic hyperkeratosis
- Epidermolytic hyperkeratosis spanning > 50% of the lesion surface
ICD coding
Epidemiology
- M = F (J Cutan Pathol 2019;46:305)
- Mean age: 58 years old (J Cutan Pathol 2019;46:305)
Sites
- Extragenital (67% of cases): head and neck, upper limbs, trunk or back, lower limbs (uncommon), oral (uncommon)
- Genital (33% of cases): vulvar, penile, perianal, perineal, scrotal
Pathophysiology
- Somatic hotspot mutations in the Arg156 position of KRT10, also known to cause epidermolytic ichthyosis (germline) (J Cutan Pathol 2020;47:524)
- Not HPV related (J Cutan Pathol 2020;47:524)
Clinical features
- Most frequently a single lesion but may be multiple (5% of instances) (J Cutan Pathol 2019;46:305)
- Erythematous, skin colored or brown papules or nodules with scale
- Multiple epidermolytic acanthomas are more likely to be found on genital sites
- Can be confused with condyloma (J Cutan Pathol 2019;46:305)
- May be pruritic
- Dermoscopy may show pearly white areas, irregular pigmented grooves and peripheral pigmented radial streak-like areas (J Am Acad Dermatol 2017;77:e37)
Diagnosis
- H&E stain with light microscopy
Prognostic factors
- Benign
Case reports
- 40 year old man with multiple epidermolytic acathomas on the fingers, mimicking flat warts (Case Rep Dermatol 2017;9:98)
- 49 year old man with multiple pruritic epidermolytic acanthomas on the scrotum (Actas Dermosifiliogr 2018;109:81)
- 56 year old man with epidermolytic acanthoma on the lower back and related dermoscopy findings (J Am Acad Dermatol 2017;77:e37)
- 57 year old man with solitary penile pidermolytic acanthoma mimicking condyloma (Dermatopathology (Basel) 2019;6:23)
- 58 year old woman with a solitary vulvar epidermolytic acanthoma mimicking condyloma (Int Angiol 1988;7:19)
- 71 year old Caucasian man with an oral solitary epidermolytic acanthoma (Oral Surg Oral Med Oral Pathol Oral Radiol 2019;128:e208)
Treatment
- Surgical excision
- Liquid nitrogen (Case Rep Dermatol 2017;9:98)
- Topical imiquimod (J Dermatol 2007;34:267)
- Topical calcipotriol (J Dermatol 2013;40:144)
Clinical images
Contributed by Simon F. Roy, M.D. and Jennifer M. McNiff, M.D.

Solitary epidermolytic acanthoma
Images hosted on other servers:

Multiple epidermolytic acanthomas on scrotum
Gross description
Microscopic (histologic) description
- Acanthosis and epidermolytic hyperkeratosis (covering > 50% of the lesion surface) (J Cutan Pathol 2019;46:305)
- Low power architecture generally resembles seborrheic keratosis (J Cutan Pathol 2019;46:305)
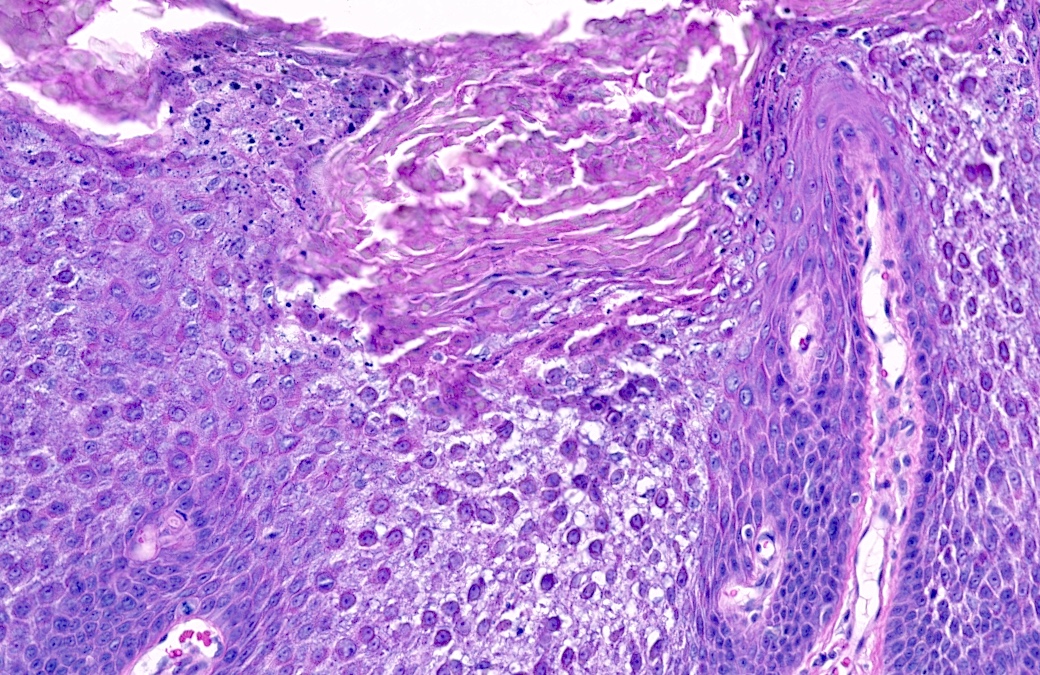
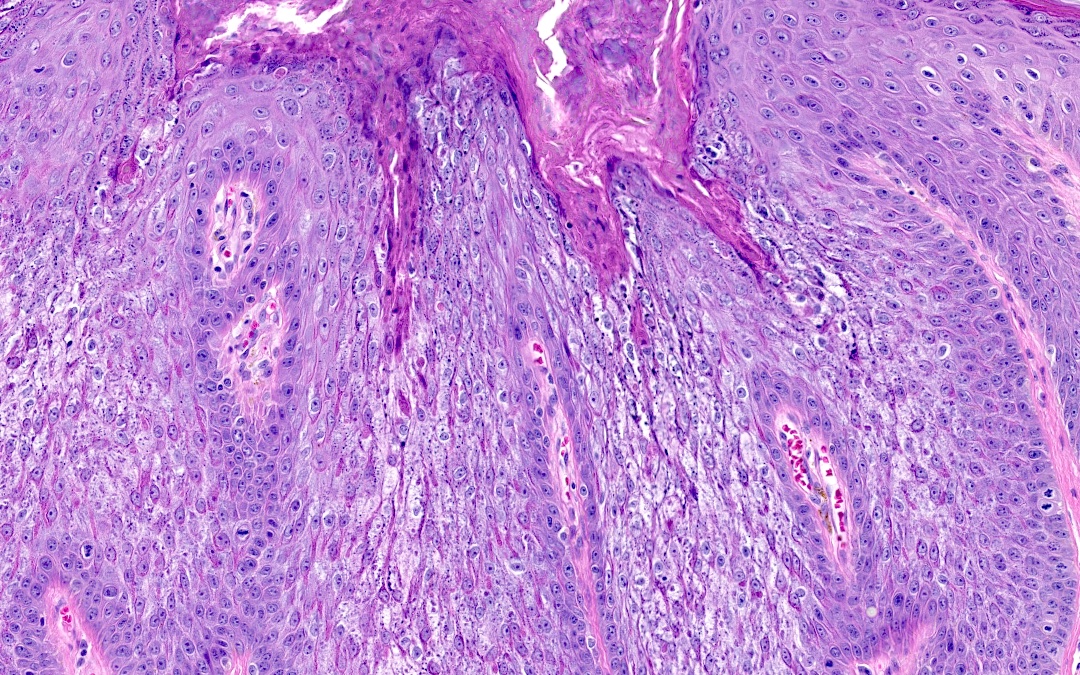
- Epidermolytic hyperkeratosis consists of lace-like degeneration of the midspinous epithelial layer, perinuclear vacuolization, epithelial eosinophilia and finely speckled keratohyaline granules (J Cutan Pathol 2019;46:305)
- 3 architectural patterns of solitary epidermolytic acanthoma have been described: papillomatous, cup shaped and acanthotic (J Eur Acad Dermatol Venereol 2011;25:175)
- Solitary and multiple epidermolytic acanthomas display similar histopathological findings (J Cutan Pathol 2019;46:305)
Microscopic (histologic) images
Contributed by Simon F. Roy, M.D. and Jennifer M. McNiff, M.D.
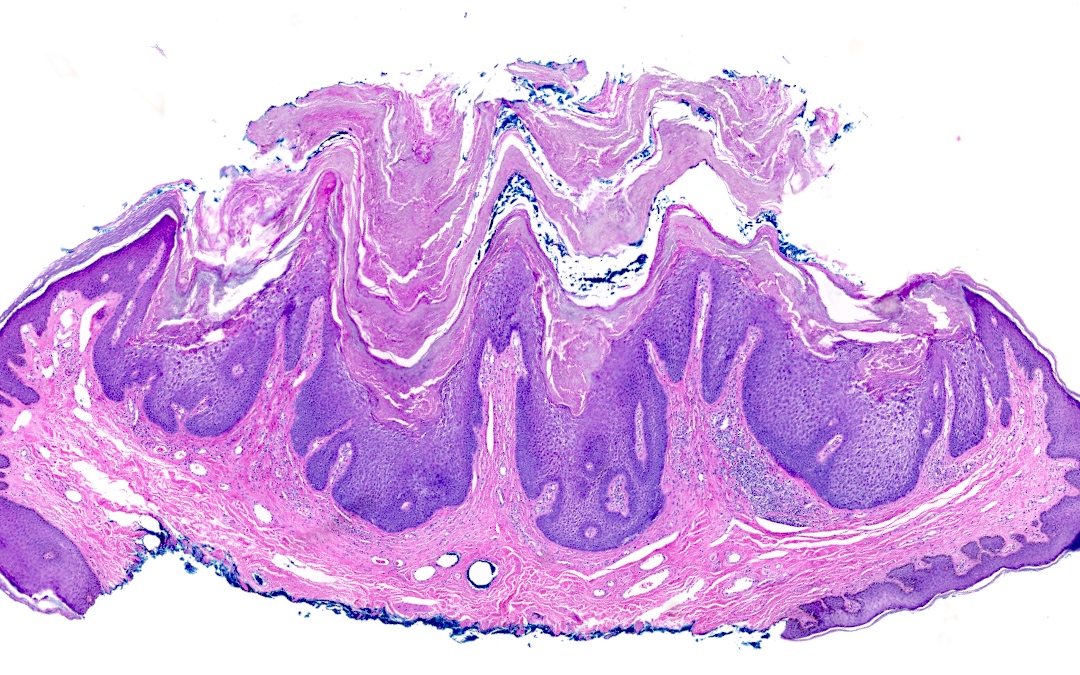
Papillomatous pattern
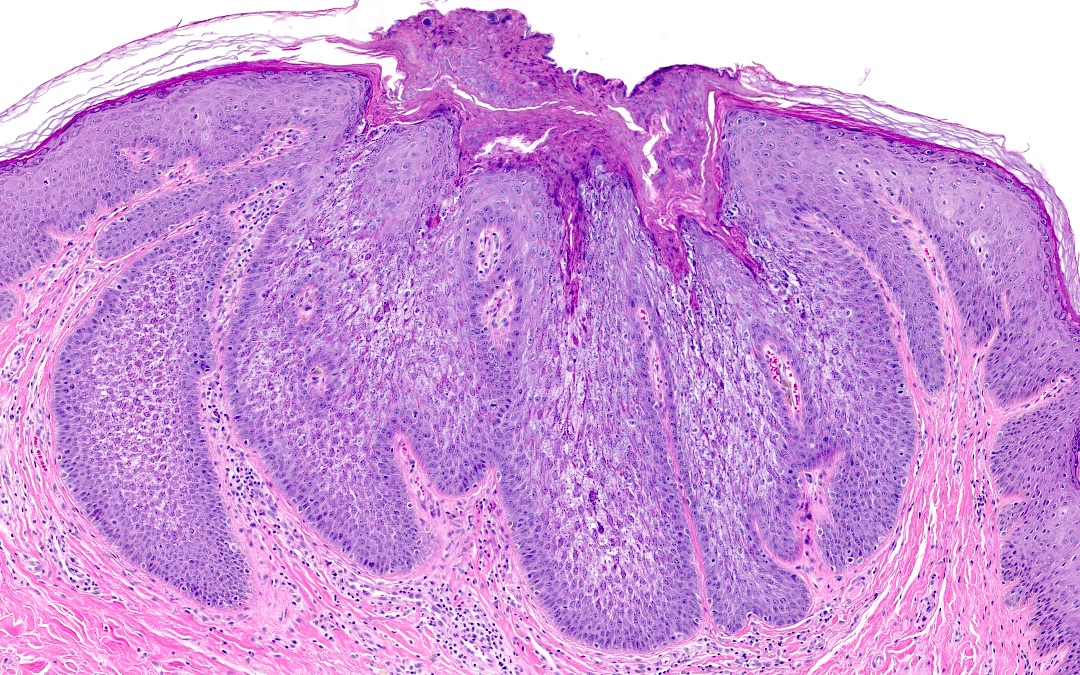
Cup-like / endophytic pattern
Positive stains
- Not usually performed
Videos
Epidermolytic hyperkeratosis
Sample pathology report
- Skin, left forearm, punch biopsy:
- Epidermolytic acanthoma
Differential diagnosis
- Seborrheic keratosis:
- Acanthosis and papillomatosis but no epidermolytic hyperkeratosis
- Focal incidental epidermolytic hyperkeratosis may be present
- Still classified as seborrheic keratosis if covering < 50% of the surface
- Verruca or condyloma:
- Hypergranulosis and finely speckled keratohyaline granules
- No lace-like reticular degeneration
- No dense cytoplasmic eosinophilia
- HPV induced
- Incidental epidermolytic hyperkeratosis in another acanthotic lesion:
- Epidermolytic hyperkeratosis is found spanning < 50% of the lesion surface
- Epidermolytic ichthyosis (formerly bullous congenital icthyosiform erythroderma):
- Generalized desquamating plaques rather than a solitary lesion
- Hereditary ichthyosiform condition due to alterations in keratin genes
- Overlapping histology with solitary epidermolytic acanthoma, clinicopathologic correlation is crucial
- Clear cell acanthoma:
- Pale epithelial cells with acanthosis but no epidermolytic hyperkeratosis
- Solitary keratosis with hypergranulotic dyscornification:
- Dense keratohyaline granules rather than finely speckled
- Both may display eosinophilic cytoplasm but perinuclear vacuolization is more characteristic of epidermolytic acanthoma
- Hypergranulotic dyscornification may be a focal incidental finding in other lesions
Additional references
Practice question #1
What is the best diagnosis based on the images above, considering this is a solitary lesion?
- Clear cell acanthoma
- Epidermolytic acanthoma
- Epidermolytic ichthyosis
- Seborrheic keratosis
Practice answer #1
B. Epidermolytic acanthoma. Epidermolytic acanthoma is an acanthotic benign lesion that displays epidermolytic hyperkeratosis on more than 50% of its surface. Clear cell acanthoma and seborrheic keratosis do not show epidermolytic hyperkeratosis on their surface. Epidermolytic ichthyosis does not present as a solitary lesion but rather as a hereditary generalized desquamative eruption.
Comment Here
Reference: Epidermolytic acanthoma
Comment Here
Reference: Epidermolytic acanthoma
Practice question #2
What is the histopathological epidermal reaction pattern seen in the image above?
- Acantholysis
- Dyskeratotic acantholysis
- Epidermal necrosis
- Epidermolytic hyperkeratosis
Practice answer #2
D. Epidermolytic hyperkeratosis. Epidermolytic hyperkeratosis is the epidermal reaction pattern displayed here, with reticular (lace-like) clearing of the epidermis, dense eosinophilia of the keratinocytes and coarse keratohyalin granules. Acantholysis is rather a rounding of keratinocytes with detached intercellular attachments (desmosomes). Dyskeratotic acantholysis shows acantholysis in addition to dense eosinophilia of keratinocytes but no reticular degeneration of finely speckled keratohyalin granules.
Comment Here
Reference: Epidermolytic acanthoma
Comment Here
Reference: Epidermolytic acanthoma
