Soft tissue
General
Grading
Author: Farres Obeidin, M.D.
Editorial Board Member: Jose G. Mantilla, M.D.
Deputy Editor-in-Chief: Borislav A. Alexiev, M.D.

Last author update: 14 January 2022
Last staff update: 14 January 2022
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Soft tissue grading pathology [TI]
Table of Contents
Definition / general | Essential features | Terminology | Fédération Nationale des Centres de Lutte Contre le Cancer (FNCLCC) grading | National Cancer Institute (NCI) grading | Pediatric Oncology Group (POG) grading | Treatment | Microscopic (histologic) images | Sample pathology report | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Obeidin F. Grading. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/softtissuegrading.html. Accessed September 16th, 2025.
Definition / general
- Grading in soft tissue tumors is to assign a level of differentiation
- Most important factor in prognosis, metastatic risk and management of soft tissue tumors (Arch Pathol Lab Med 2006;130:1448)
Essential features
- Grading is required in soft tissue sarcomas where possible
- Management often relies on the grade
- FNCLCC (Fédération Nationale des Centres de Lutte Contre le Cancer) is the most common grading system; defined by a combination of tumor differentiation, mitotic count and necrosis
Terminology
- FNCLCC: Fédération Nationale des Centres de Lutte Contre le Cancer
- NCI: National Cancer Institute
- POG: Pediatric Oncology Group
Fédération Nationale des Centres de Lutte Contre le Cancer (FNCLCC) grading
- Based on a combination of tumor differentiation / histology, mitotic count and tumor necrosis
- Tumor differentiation
- Given 1, 2 or 3 points based on how closely it resembles normal tissue
- See table 1 for specific point values by histologic type
- Mitotic count: 10 successive high power fields (HPFs) in the most mitotically active area
- 1 point: 0 - 9 mitoses
- 2 points: 10 - 19 mitoses
- 3 points: 20 or more mitoses
- Tumor necrosis
- 0 points: no necrosis
- 1 point: < 50% necrosis
- 2 points: ≥ 50% necrosis
- Grade: sum total of tumor differentiation, mitotic count and tumor necrosis scores
- Grade 1: 2 - 3 points
- Grade 2: 4 - 5 points
- Grade 3: 6 - 8 points
- Tumor differentiation
- Additional notes on specific tumors:
- Sarcomas not graded in the FNCLCC system: embryonal and alveolar rhabdomyosarcoma, angiosarcoma, extraskeletal myxoid chondrosarcoma, alveolar soft part sarcoma, clear cell sarcoma and epithelioid sarcoma
- Malignant peripheral nerve sheath tumor:
- FNCLCC grading has been controversial, recent data suggests an overall correlation with survival (Am J Clin Oncol 2022;45:28)
- Tumor differentiation score may be variable based on closeness to benign peripheral nerve sheath tumors:
- Score 1: resembles benign peripheral nerve sheath tumor with increased cellularity and mitotic activity
- Score 2: overtly malignant with characteristics of nerve sheath differentiation (i.e. marbling and short fascicle formation)
- Score 3: overtly malignant lacking nerve sheath differentiation, having heterologous elements or epithelioid morphology
- In neurofibromatosis type 1 (NF1) associated tumors, the distinction between neurofibroma and low grade malignant peripheral nerve sheath tumor may be difficult and certain criteria have been proposed (Hum Pathol 2017;67:1) (see table 2)
- Myxofibrosarcoma grading by FNCLCC is controversial; currently graded by level of cellularity and percentage of myxoid versus solid areas
- Dedifferentiated liposarcoma:
- By FNCLCC, well differentiated liposarcoma / atypical lipomatous tumor by definition are grade 1 and dedifferentiated liposarcoma may be grade 2 or 3
- There remains controversy over whether nonlipogenic areas with low grade features should be classified as low grade dedifferentiation or cellular well differentiated liposarcoma (Am J Surg Pathol 2007;31:1)
- Well differentiated liposarcoma may represent a spectrum of tumors with variable prognosis (J Surg Oncol 2018;117:1799)
- Solitary fibrous tumors and gastrointestinal stromal tumors are not graded; metastatic risk is given by specific risk stratification nomograms
- Grading on core needle biopsies
- Encouraged where possible but may be limited by amount of tissue
- Separation at least into low (FNCLCC 1) versus high (FNCLCC 2 and 3) grade is recommended as there are implications for neoadjuvant therapy
Table 1: tumor differentiation score by histologic type
| Atypical lipomatous tumor / well differentiated liposarcoma | 1 |
| Well differentiated leiomyosarcoma | 1 |
| Malignant neurofibroma | 1 |
| Well differentiated fibrosarcoma | 1 |
| Myxoid liposarcoma | 2 |
| Conventional leiomyosarcoma | 2 |
| Conventional fibrosarcoma | 2 |
| Myxofibrosarcoma | 2* (see above) |
| High grade myxoid liposarcoma | 3 |
| Pleomorphic liposarcoma | 3 |
| Dedifferentiated liposarcoma | 3 |
| Pleomorphic rhabdomyosarcoma | 3 |
| Poorly differentiated / pleomorphic leiomyosarcoma | 3 |
| Synovial sarcoma | 3 |
| Mesenchymal chondrosarcoma | 3 |
| Extraskeletal osteosarcoma | 3 |
| Extraskeletal Ewing sarcoma | 3 |
| Malignant rhabdoid tumor | 3 |
| Undifferentiated pleomorphic sarcoma | 3 |
| Undifferentiated sarcoma, NOS | 3 |
Table 2: NF1 associated malignant peripheral nerve sheath tumor (MPNST) grading
| Atypical neurofibromatous neoplasm of uncertain biologic potential (ANNUBP) | Schwann cell neoplasm with ≥ 2 of 4 features: cytologic atypia, loss of neurofibroma architecture, hypercellularity, < 3 mitoses per 10 HPFs |
| MPNST, low grade | Features of ANNUBP but with mitotic count of 3 - 9 mitoses per 10 HPFs and no necrosis |
| MPNST, high grade | MPNST with ≥ 10 mitoses per 10 HPFs or 3 - 9 mitoses per 10 HPFs combined with necrosis |
National Cancer Institute (NCI) grading
- Less commonly used grading system
- Similar performance to the FNCLCC grading system but more difficult to objectively quantify (J Clin Oncol 1997;15:350)
- Uses older terminology and defunct diagnoses
| |
| |
| |
|
Pediatric Oncology Group (POG) grading
- Created as a modification of the NCI system for use in nonrhabdomyosarcomatous sarcomas in the pediatric population
- Similar performance to FNCLCC but may upgrade certain tumors (Cancer 2010;116:2266)
| |
| |
| |
|
Treatment
- Clinical staging for sarcomas of trunk, extremities and retroperitoneum depends on the grade
- Localized grade 1 sarcomas are staged as stage IA or IB
- Grade 2 - 3 sarcomas or metastatic sarcomas are staged as stage II - IV
- Higher grade tumors often require adjuvant therapy to control their higher metastatic risk
Microscopic (histologic) images
Contributed by Farres Obeidin, M.D.
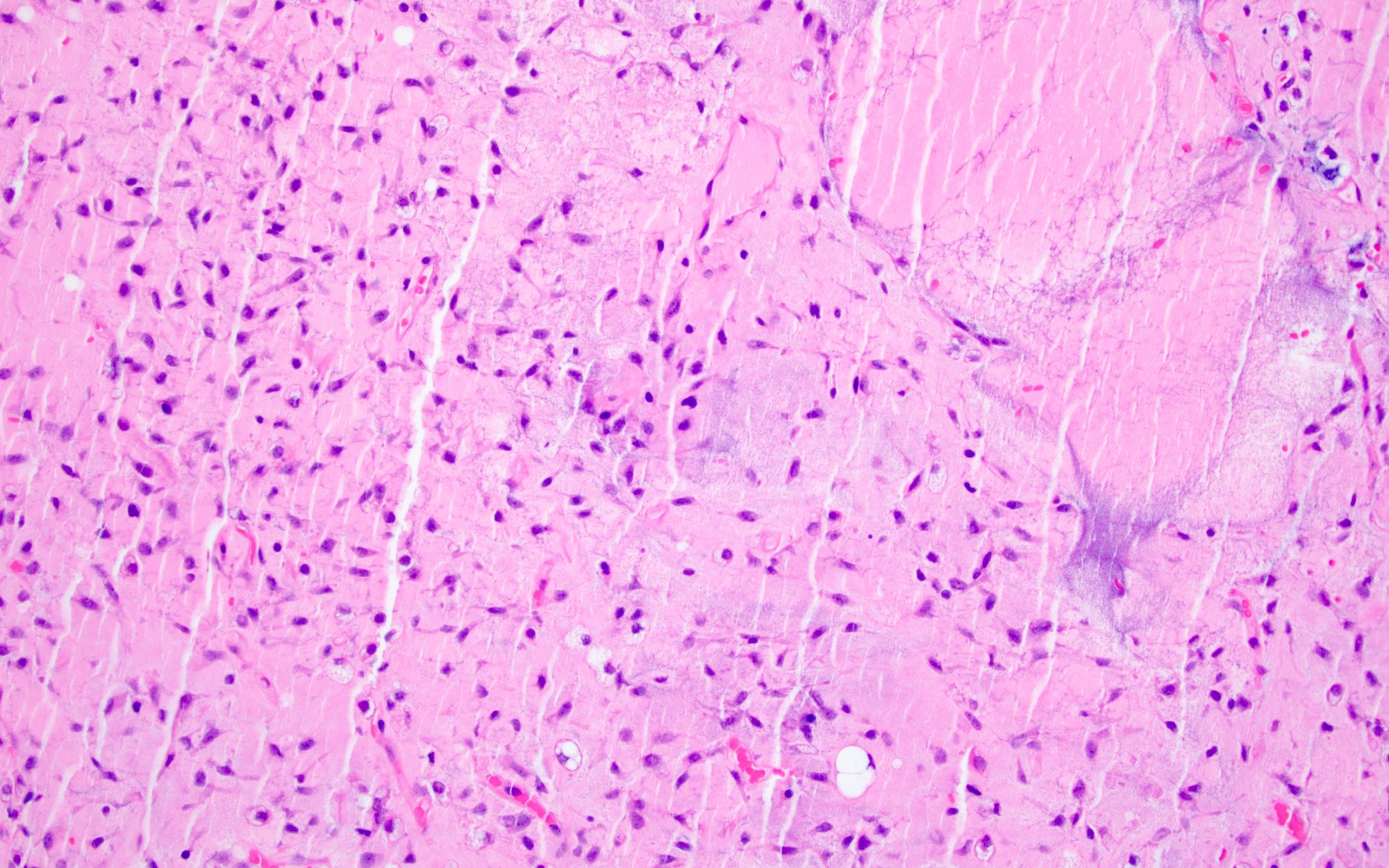
FNCLCC grade 1
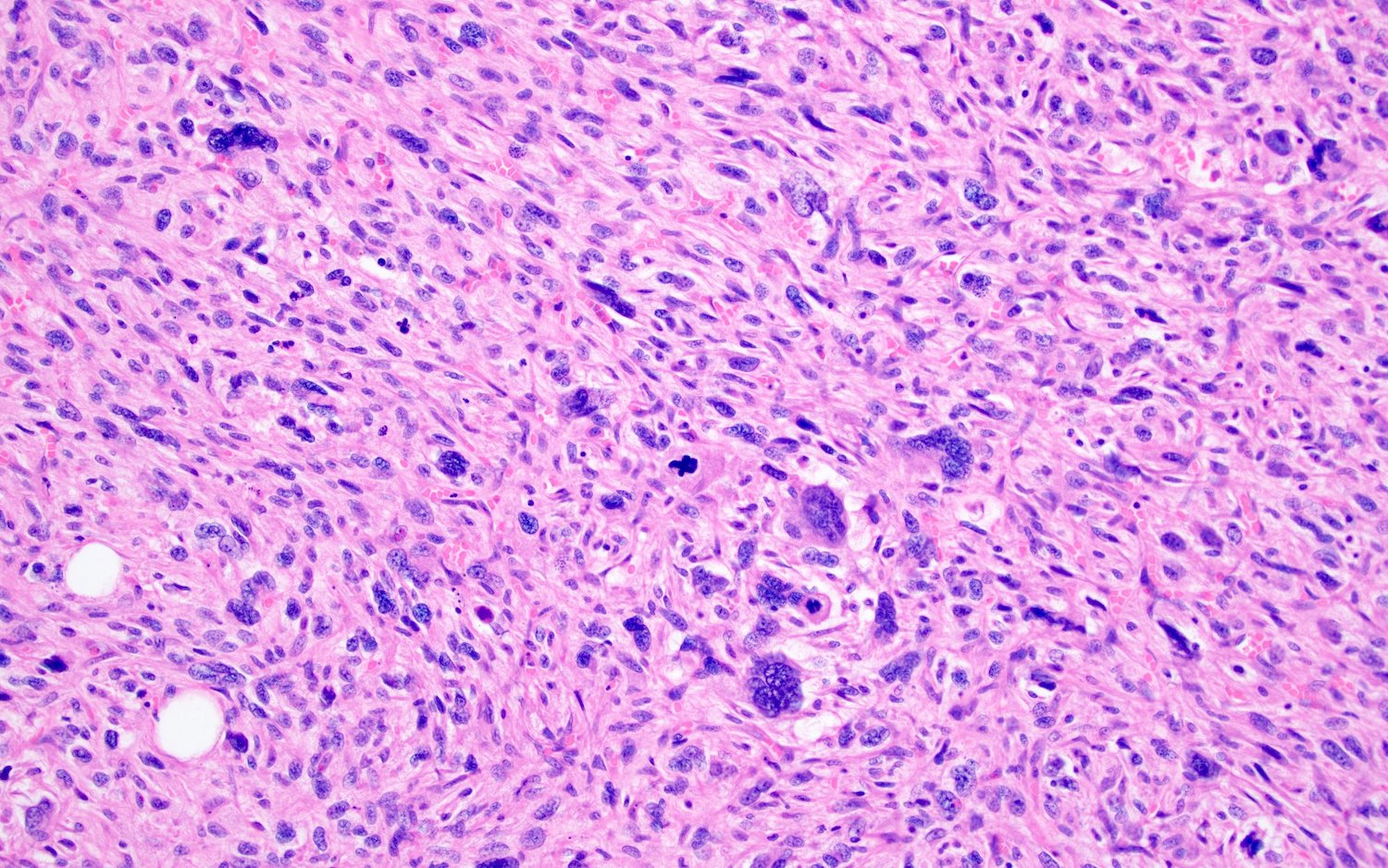
FNCLCC grade 3
Sample pathology report
- Right leg, mass, radical resection:
- Undifferentiated pleomorphic sarcoma, FNCLCC grade 3 (see comment)
- Comment: Histologic sections demonstrate a pleomorphic malignancy without evidence of definitive line of differentiation, consistent with an undifferentiated pleomorphic sarcoma (score 3). The mitotic count is up to 25 mitoses per 10 HPFs (score 3) and there is necrosis encompassing approximately 20% of the tumor volume (score 1).
Additional references
- WHO Classification of Tumours Editorial Board: Soft Tissue and Bone Tumours, 5th Edition, 2020, College of American Pathologists: Protocol for the Examination of Resection Specimens from Patients with Soft Tissue Tumors [Accessed 6 August 2021], National Comprehensive Cancer Network: Soft Tissue Sarcoma (Version 2.2021) [Accessed 6 August 2021]
Practice question #1
A 65 year old man presents with a 10 cm leg mass. A core needle biopsy is performed which demonstrates a leiomyosarcoma. Which of the following most accurately describes the factors involved in FNCLCC grading of this lesion?
- Mitotic activity, size, necrosis
- Pleomorphism, architecture, vascular invasion
- Size, age, location
- Tumor differentiation, mitotic activity, necrosis
Practice answer #1
D. FNCLCC grading is based on a combined score of tumor differentiation, mitotic activity and necrosis
Comment Here
Reference: Soft tissue grading
Comment Here
Reference: Soft tissue grading
Practice question #2
A 30 year old woman presents with a 5 cm arm mass. After histologic examination and ancillary studies, a diagnosis of synovial sarcoma is made. The tumor has up to 12 mitoses per 10 HPFs and no necrosis is seen. What is the appropriate FNCLCC grade for this tumor?
- FNCLCC grade 1
- FNCLCC grade 2
- FNCLCC grade 3
- Not graded by FNCLCC
Practice answer #2
B. FNCLCC grade 2. The combination of tumor differentiation (score 3), mitotic activity (score 2) and necrosis (score 0) sum to 5, which falls under grade 2 in the FNCLCC grading system.
Comment Here
Reference: Soft tissue grading
Comment Here
Reference: Soft tissue grading
