Stains & CD markers
Immunohistochemistry (IHC) procedure

Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: immunohistochemistry procedure
Immunohistochemistry (IHC) procedure
Author: Nat Pernick, M.D.
Last author update: 1 July 2015
Last staff update: 21 June 2021
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: immunohistochemistry procedure
Table of Contents
Definition / general | Common errors | IHC procedure - general | Diagrams / tables | Uses by pathologists | Microscopic (histologic) images | VideosCite this page: Pernick N. IHC procedure. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/stainsihcprocedure.html. Accessed September 17th, 2025.
Definition / general
- Immunohistochemistry (IHC) is a tool for surgical pathology and research
- Diagnosis should be based on H&E morphology, with confirmation by immunohistochemistry or molecular testing; it is dangerous to use immunohistochemistry alone to make the diagnosis
- A stain / result is not just positive or negative; focus on the types of cells that are immunoreactive and determine if they are tumor cells, inflammatory cells, normal cells or stromal cells; comparing the results to an H&E stained section or a negative control of the same block may be helpful (Am J Surg Pathol 2007;31:1627, J Clin Pathol 2011;64:466)
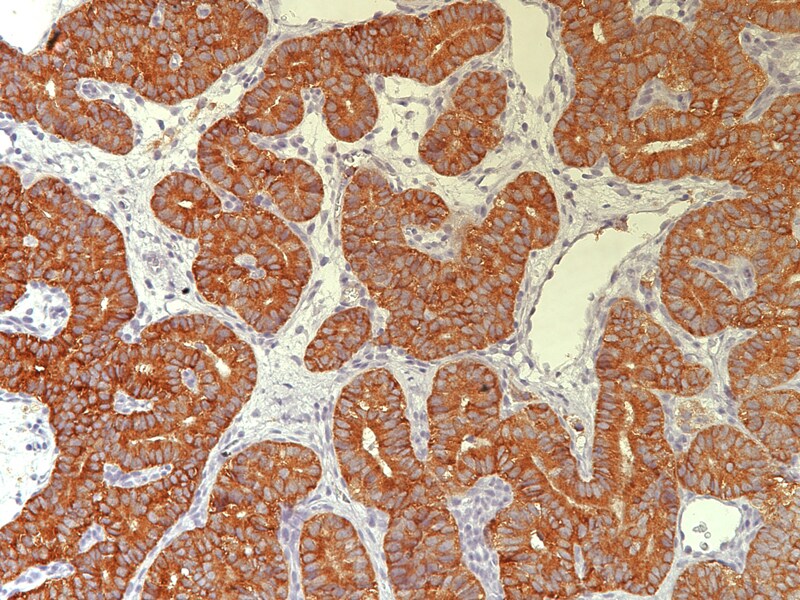
- After you identify the type of cell staining, it is helpful to note the percentage of these cells staining, the intensity of staining (weak, 1+, 2+, 3+, 4+) and the pattern of staining (membranous, cytoplasmic, nuclear, dot-like)
- The pattern of immunoreactivity should follow the anatomic distribution of the antigen before it is called positive / immunoreactive
- Reference: CAP Laboratory Improvement Programs: Principles of Analytic Validation of Immunohistochemical Assays
- Antibodies are often useful beyond their recommended expiration dates
- Combining results from different studies may be hazardous, as studies may use different antibodies and different standards of interpretation
- Recommended to interpret immunohistochemical stains in small needle core biopsy specimens based on the area with the greatest immunoreactivity (Am J Clin Pathol 2007;127:273)
Common errors
- Not using a positive or negative control; they are helpful in interpreting the staining pattern, particularly if it is heavy or weak
- Other sources of error are ectopic antigen expression (may be due to abundant endogenous biotin, Hum Pathol 2011;42:369), cross reactions (Mod Pathol 2012;25:231), less specificity than thought (Int J Clin Exp Pathol 2012;5:137), use of the wrong secondary antibody or rarely the wrong primary antibody
IHC procedure - general
- Most important steps in immunohistochemistry are selection of appropriate antibodies, correct interpretation, technical quality and integration of results into final diagnosis (Am J Surg Pathol 2002;26:873)
- Pretreatment, often with microwaving of tissue in citrate buffer to unmask antigens hidden by formalin cross-links or other fixative
- Other agents for pretreatment (antigen retrieval) are pepsin, proteases and trypsin
- Apply primary antibody (monoclonal antibodies usually are more specific); antibody binds to antigens of interest
- Wash off excess primary antibody
- Add biotinylated anti-IgG antibody (secondary antibody), which binds to the primary antibody present
- Add avidin-biotin-peroxidase complex, which binds to secondary antibody
- Add 3, 3’ diaminobenzidine (DAB) as a chromagen (color changing reagent), with hematoxylin counterstaining
- Other enzyme complexes besides avidin-biotin are horseradish peroxidase, alkaline phosphatase with naphthol phosphate and glucose oxidase with nitroblue tetrazolium
- Other chromagens besides DAB are AEC (water soluble, sensitive to light)
- Alternative fixation methods are possible, but must validate IHC for each target (Virchows Arch 2012;461:259)
- References: Wikipedia, IHC World-protocols, NordiQC
Diagrams / tables
Images hosted on other servers:

Direct method (uses only one antibody)

Indirect method (uses primary and secondary antibodies)
Uses by pathologists
- Assist with diagnosis, by identifying staining patterns characteristic of specific tumors or disease processes
- Assist with identification of normal tissue
- Identify protein overexpression (HER2, EGFR), which is associated with response to treatment, and so is useful to clinicians
- For research, to assist in understanding disease processes
Microscopic (histologic) images
Case of the Week #200
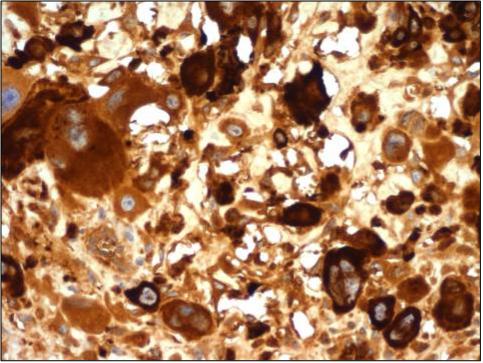
Cytoplasmic staining pattern (beta hCG):
stain is diffuse within cytoplasm
Images hosted on other servers:

Golgi staining pattern: prolactin
Cytoplasmic staining pattern (inhibin):
stain is diffuse within cytoplasm

Nuclear staining pattern: p63 in myoepithelial carcinoma

Dot-like staining pattern
Videos