

Placenta
Nonneoplastic placental conditions and abnormalities
Placental findings in specific conditions
Fetus in fetu
Author: Jennifer R. Kaley, M.D.

Last author update: 1 April 2016
Last staff update: 7 September 2022
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: fetus in fetu


Table of Contents
Definition / general | Radiology images | Epidemiology | Treatment | Case reports | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Differential diagnosis | Additional referencesCite this page: Kaley JR. Fetus in fetu. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/syndromesfif.html. Accessed April 26th, 2024.
Definition / general
- To our knowledge, FIF was originally described by Meckel in the 18th century
- Subsequently, Willis described it as rare condition in which a malformed parasitic twin was found inside the body of its partner, usually in the abdominal cavity; Willis defined FIF in 1935 as a "mass containing a vertebral axis often associated with other organs or limbs around this axis" (Willis: The Borderland of Embryology and Pathology, 1962)
- Presence of a vertebral axis in a fetiform mass has since been considered pathognomonic of FIF
- Although several theories as to the pathogenesis of FIF had been proposed, the "twinning" theory has become accepted, as the mass is always found enclosed within a sac resembling the amniotic sac - in fact, the lining of the sac histologically resembles the amniotic membrane
- Of late, Spencer has proposed that one or more of the following criteria needs to be present to label any fetiform mass as FIF: (1) the mass must be enclosed within a distinct sac, (2) it should be partially or completely covered by normal skin, (3) it should have grossly recognizable anatomic parts, (4) it should be attached to its host by only few relatively large blood vessels, (5) it should either be located immediately adjacent to one of the sites of attachments of conjoined twins or be associated with neural tube or the gastrointestinal tract (Clin Anat 2001;14:428)
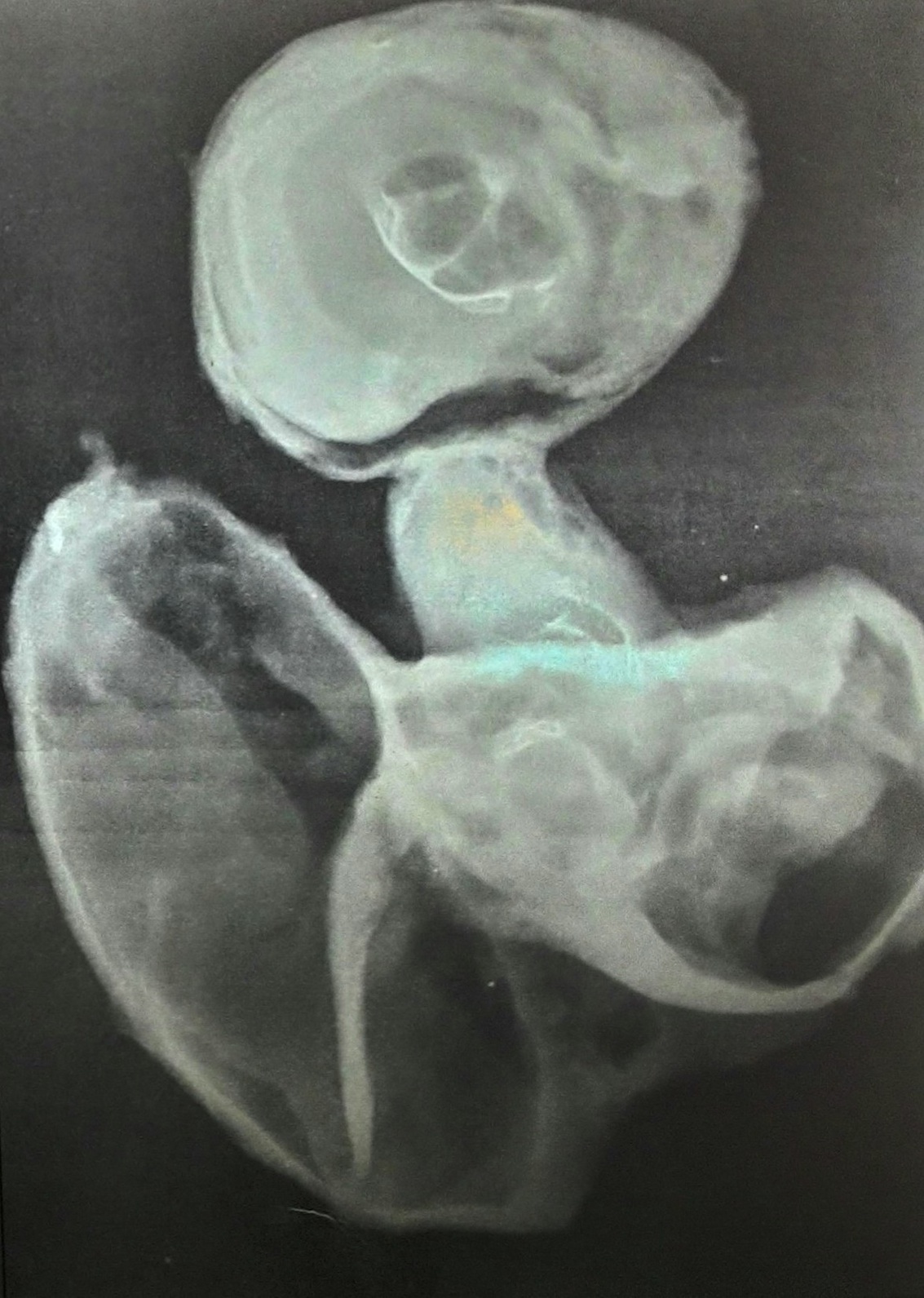
Radiology images
Epidemiology
- Fetus-in-fetu (FIF) is an extremely rare pathological condition with an estimated incidence of 1 in 500,000 births
- Less than 200 cases have been reported worldwide
Treatment
- Surgical excision is curative, although the presence of immature elements indicates the need for close clinical, radiological and serological (AFP) followup
Case reports
- 18 month old girl with retroperitoneal mass (Case of the Week #385)
Gross description
Case #385:
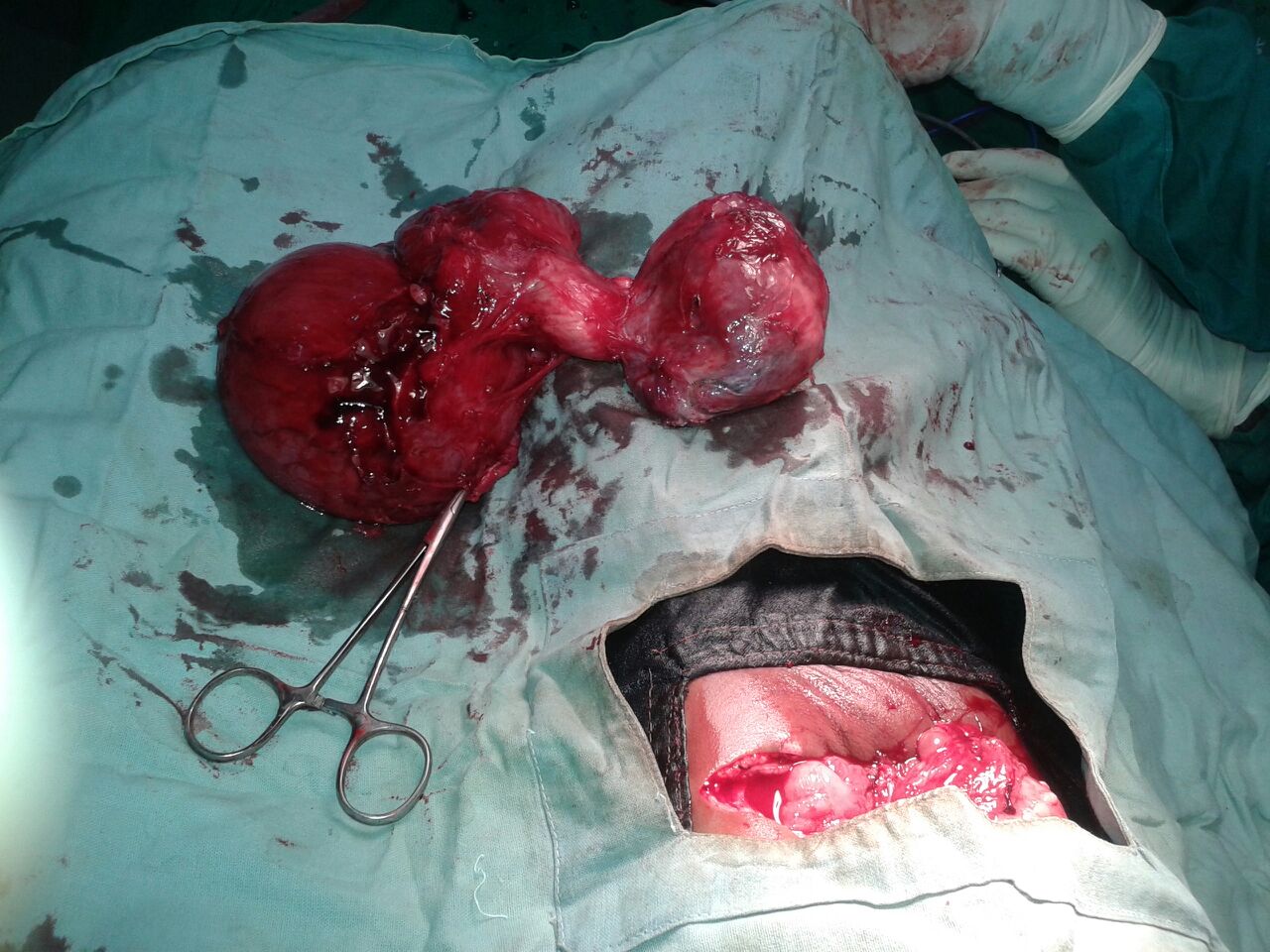
- Mass measured 18 x 10 x 6 cm and weighed 910 g
- External surface was sac-like and smooth, with partial skin covering the upper region
- Vertical cut section showed solid and large cystic areas containing mucoid material
- Upper segment of the mass contained hair, pultaceous (pulpy) material, scalp and brain substance
- Middle segment showed vertebral column, cartilage, intestine and gray-white solid areas
- Lower segment contained a cyst with a flattened wall and limb bud-like structures attached to the external aspect
Gross images


Microscopic (histologic) description
Case #385:
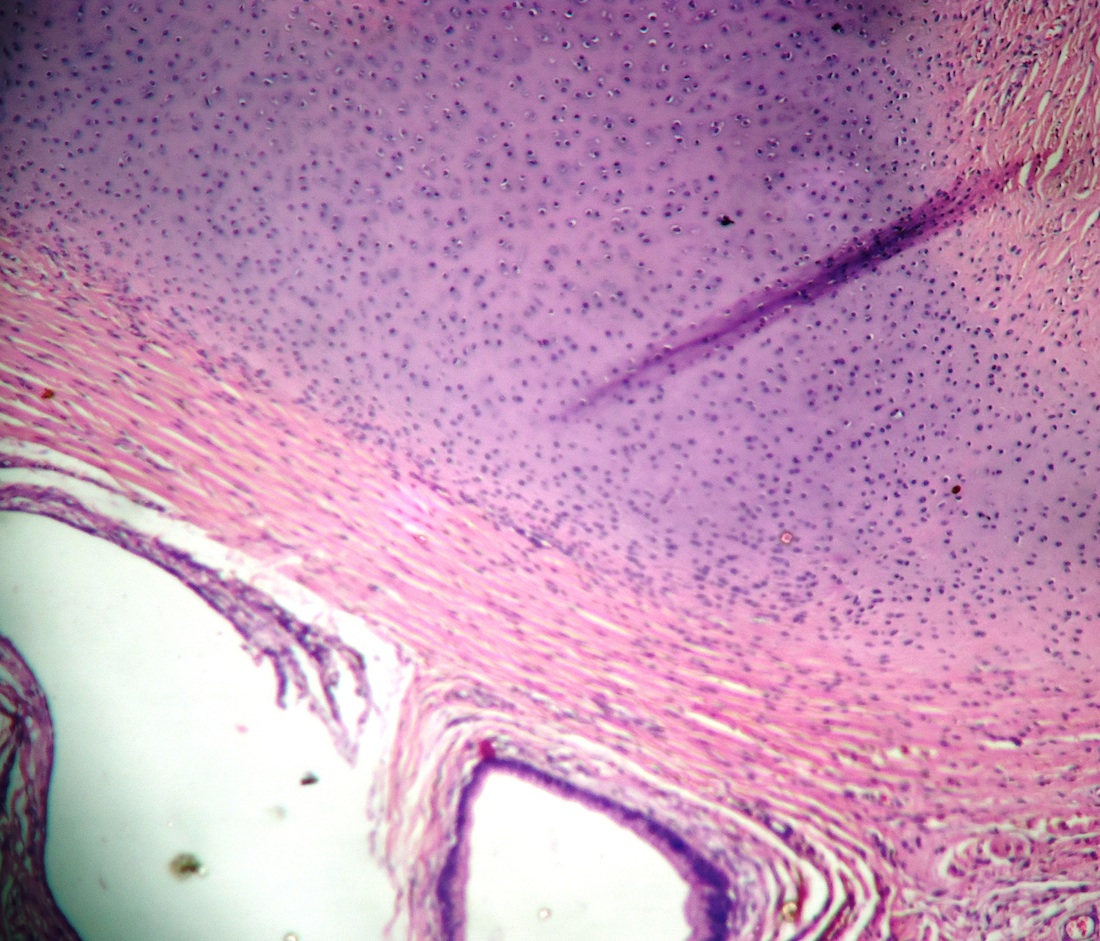
- Upper segment showed primitive brain parenchyma, cartilage and skin with adnexa and hair
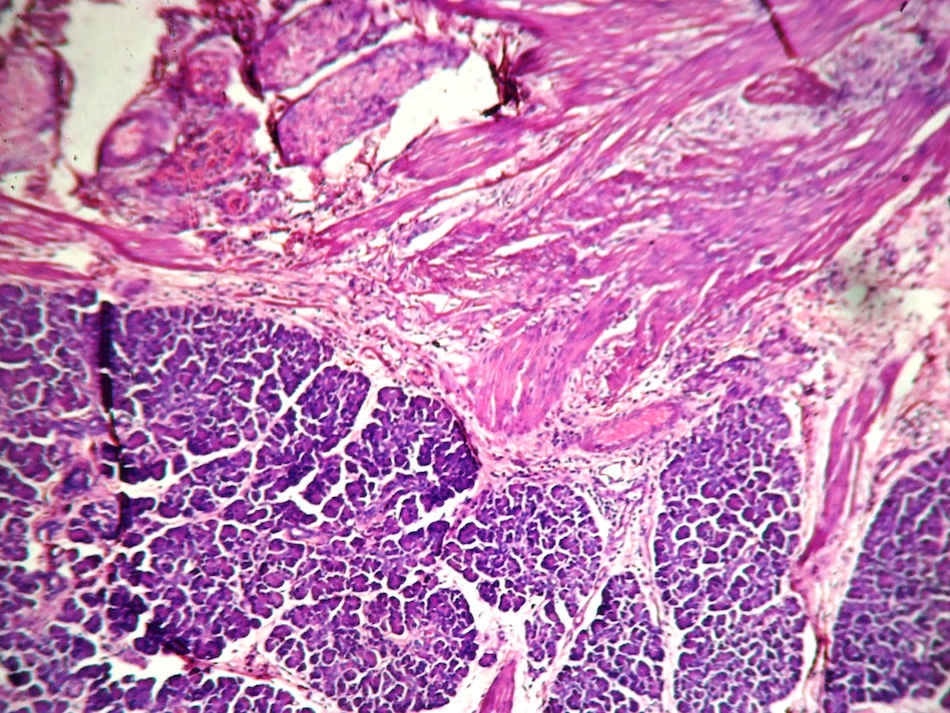
- Middle segment contained stomach, duodenum, small intestine, vertebral column, bone and bone marrow, pancreas, soft tissue, lymph nodes and adipose tissue
- Lower segment contained a cyst wall with flattened lining and no adnexal structures
Microscopic (histologic) images
Differential diagnosis
Other retroperitoneal masses such as:
- Hydronephrosis
- Neuroblastoma
- Teratoma: main diagnostic challenge lies in differentiating FIF from retroperitoneal teratoma, which contains pluripotent cells without organogenesis or vertebral segmentation; this distinction is important as the latter can be associated with risk of malignancy; most important feature that has been used to distinguish between FIF and teratoma is the presence of the vertebral column
- Wilms tumor
