
14 August 2019 - Case of the Month #482
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Sajna V. M. Kutty, MVR Cancer Centre, Calicut, Kerala (India) for contributing this case and Dr. Raul S. Gonzalez, Beth Israel Deaconess Medical Center, Boston, Massachusetts (USA), for writing the discussion.
Case of the Month #482
Clinical history:
A 76 year old woman with rectal carcinoma had a possible enteric duplication cyst in the distal ileum by MRI. A right colon limited resection was performed.
Gross images:



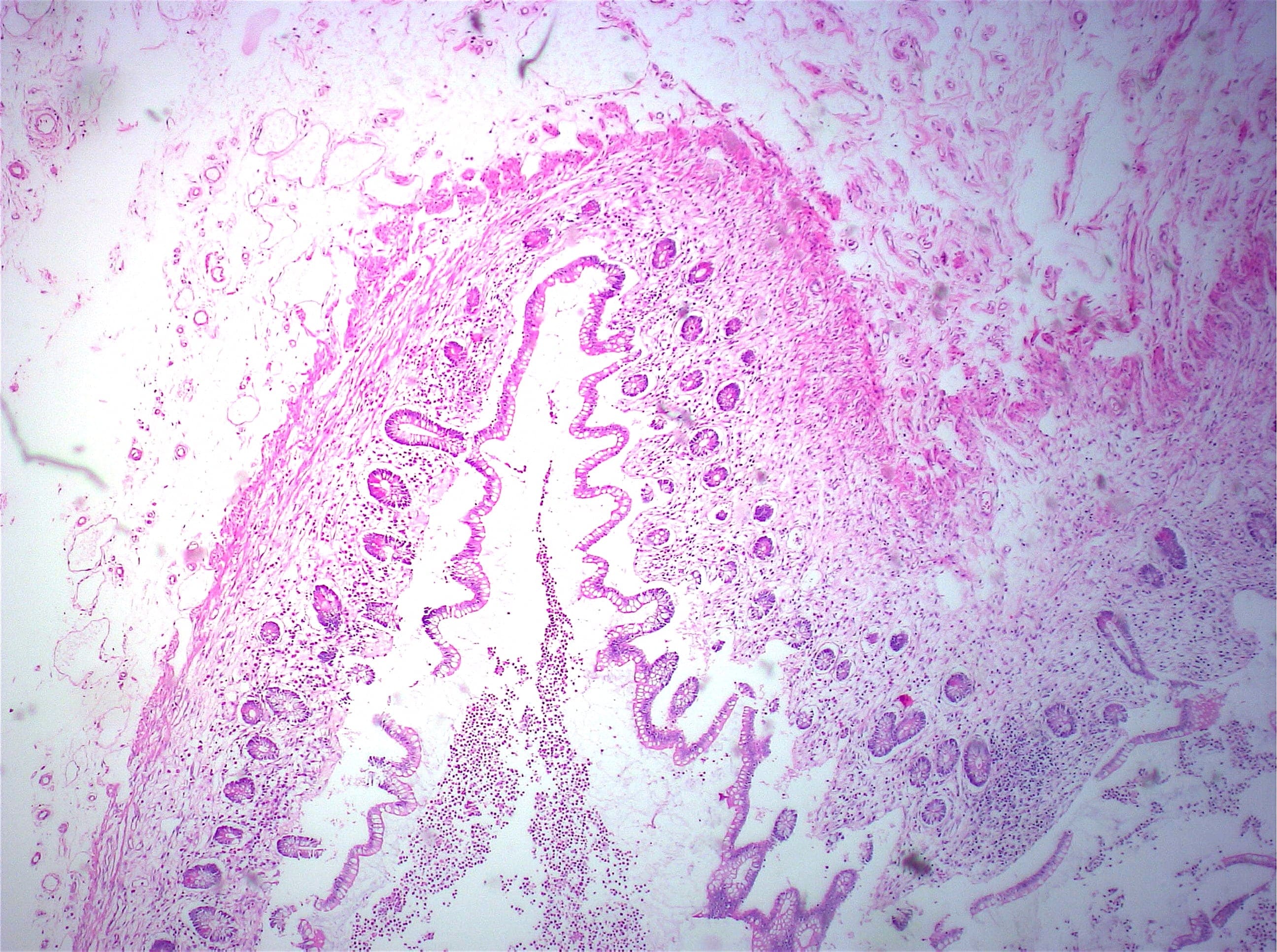
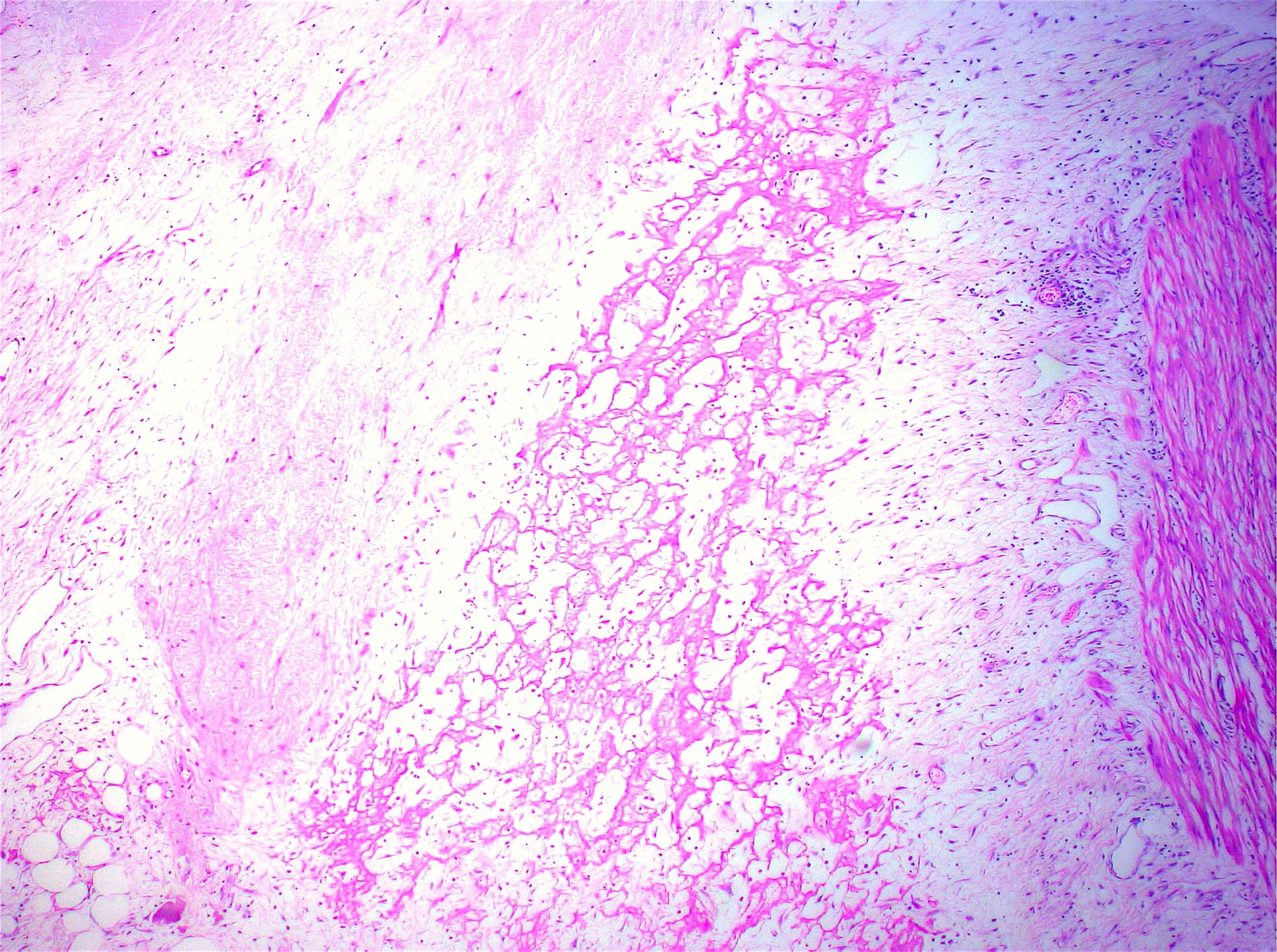
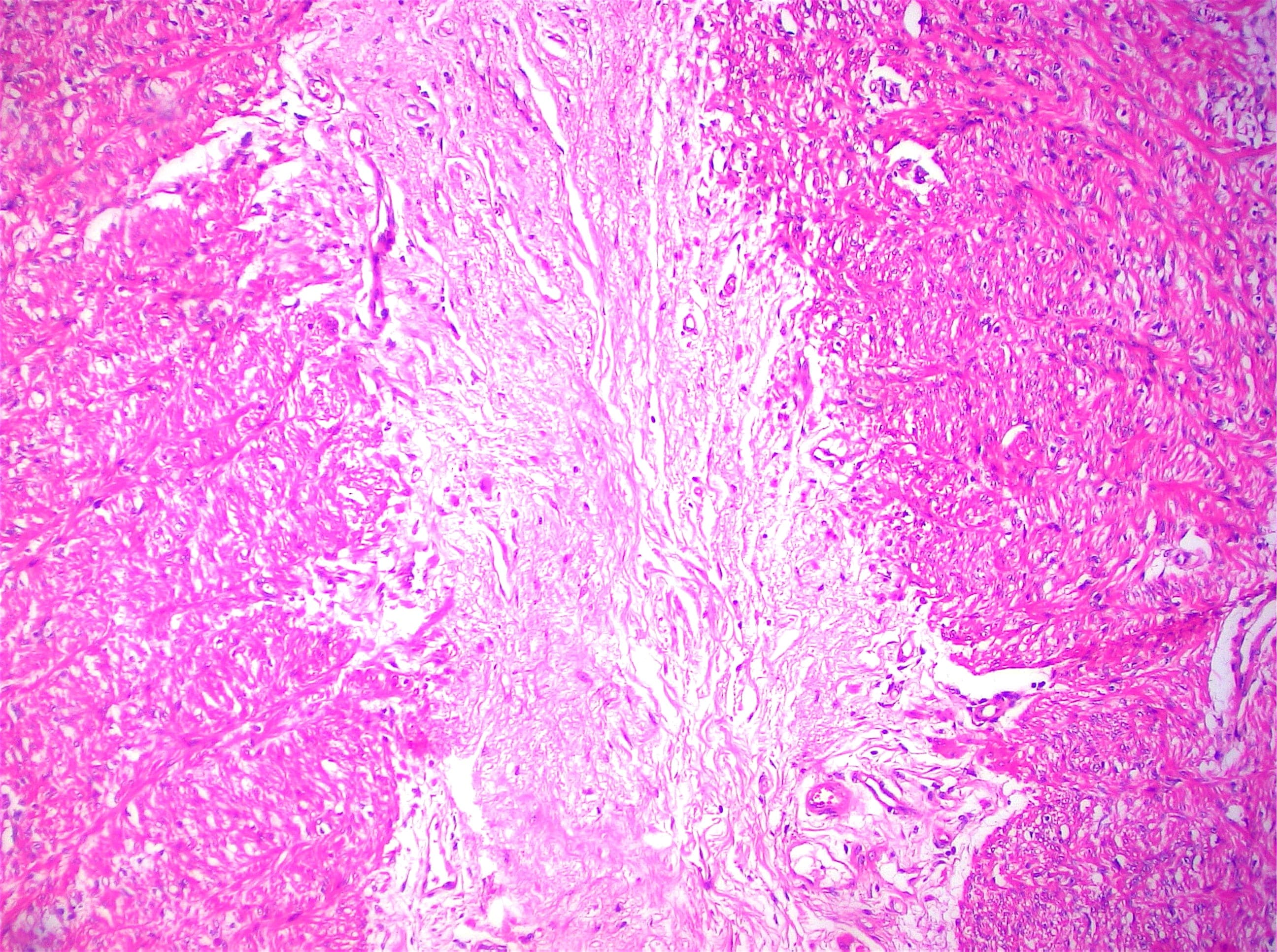
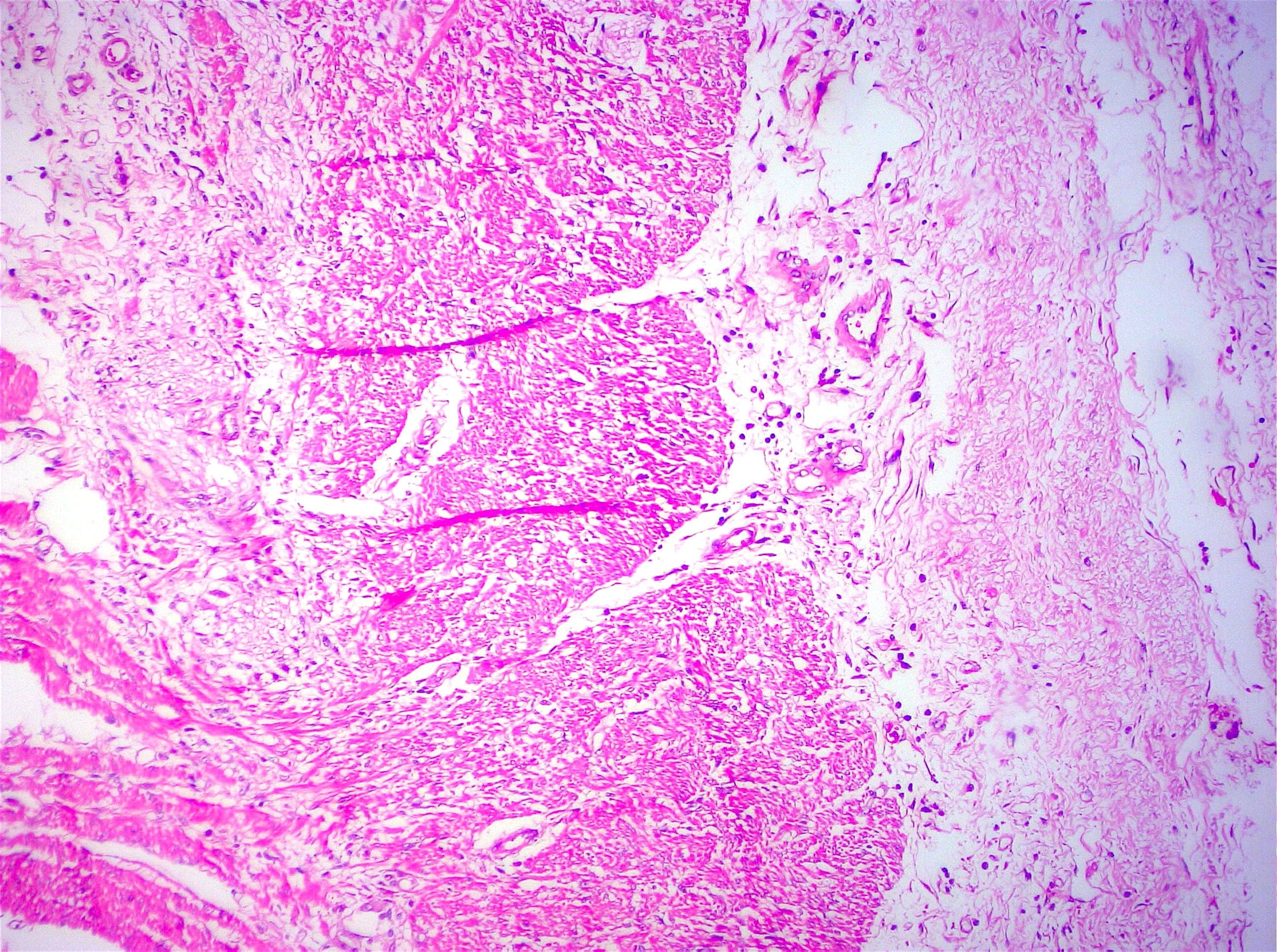
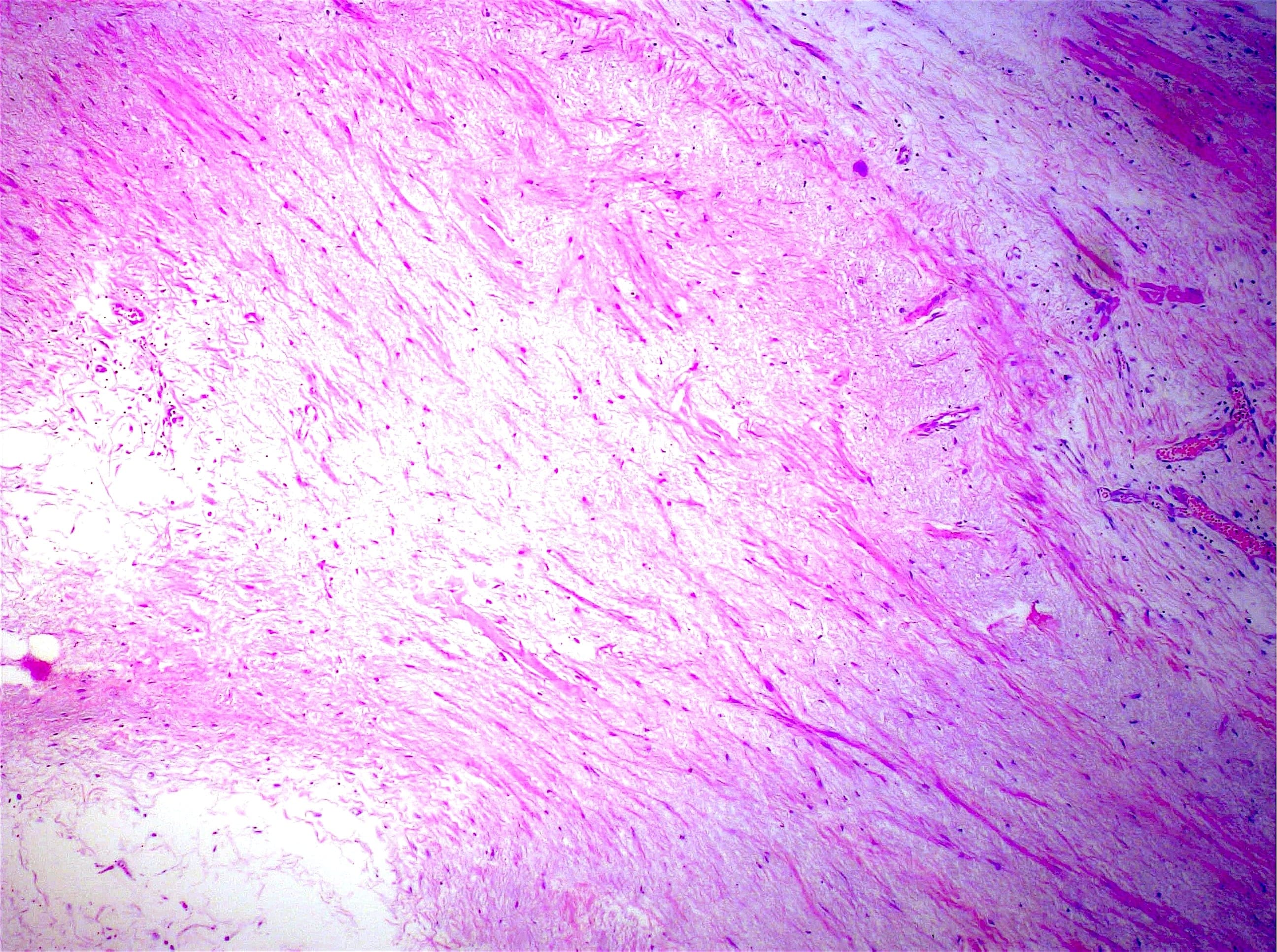
Histopathology images:
What is your diagnosis?
Diagnosis: Sclerosing encapsulated peritonitis (abdominal cocoon)
Test question (answer at the end):
Sclerosing encapsulating peritonitis most often involves what intraperitoneal organ?
A. Colon
B. Ovary
C. Small bowel
D. Stomach
Discussion:
Sclerosing encapsulating peritonitis, more commonly referred to as "abdominal cocoon" is a rare condition characterized by fibrosis and inflammation of the peritoneum, ultimately leading to membranous encasement of the viscera with resultant intestinal obstruction. Among the reported cases, the average age is 39 years, about two-thirds of patients are male and most afflicted patients reside in tropical or subtropical countries (Sultan Qaboos Univ Med J 2016;16:e142). The most common presenting symptom is abdominal pain. Abdominal imaging shows clumped bowel loops and abdominal/peritoneal calcification, potentially with visualization of the membrane (AJR Am J Roentgenol 2004;182:639); surgical findings are confirmatory. While early cases can be managed medically with corticosteroids or total parenteral nutrition, nearly all patients eventually undergo surgery.
Sclerosing encapsulating peritonitis can be classified into three types. Type I involves part of the small bowel, type II involves the entire small bowel, and type III extends into other adjacent organs, including the large bowel and the ovaries. A minority of cases are primary (idiopathic), with the remaining cases secondary to medication induced injury, procedure related injury, autoimmune conditions and infections such as tuberculosis (Clujul Med 2017;90:179).
Microscopically, sclerosing encapsulating peritonitis is characterized by thickened fibrocollagenous tissue extending along the serosal surface of the bowel with loss of the normal mesothelial lining. An inflammatory infiltrate may be present and lymphatics may be dilated (World J Gastroenterol 2012;18:1999).
The clinical and imaging features of sclerosing encapsulating peritonitis are quite striking and pathologists are unlikely to face a taxing differential diagnosis. The only other cause of diffuse peritoneal fibrosis is peritoneal encapsulation, a developmental anomaly that creates a thin, uninflamed accessory mesothelial membrane that rarely causes symptoms (World J Gastrointest Surg 2015;7:174). Focal fibrous appearing masses that can arise in the abdomen include desmoid type fibromatosis (which would show nuclear positivity for beta catenin), inflammatory myofibroblastic tumor (which often shows positivity for ALK1) and sclerosing mesenteritis but these should not manifest as membranes lining the small bowel serosa.
Test question answer:
C. Small bowel
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Sajna V. M. Kutty, MVR Cancer Centre, Calicut, Kerala (India) for contributing this case and Dr. Raul S. Gonzalez, Beth Israel Deaconess Medical Center, Boston, Massachusetts (USA), for writing the discussion.

Advertisement
Case of the Month #482
Clinical history:
A 76 year old woman with rectal carcinoma had a possible enteric duplication cyst in the distal ileum by MRI. A right colon limited resection was performed.
Gross images:
Histopathology images:
What is your diagnosis?
Click here for diagnosis, test question and discussion:
Diagnosis: Sclerosing encapsulated peritonitis (abdominal cocoon)
Test question (answer at the end):
Sclerosing encapsulating peritonitis most often involves what intraperitoneal organ?
A. Colon
B. Ovary
C. Small bowel
D. Stomach
Discussion:
Sclerosing encapsulating peritonitis, more commonly referred to as "abdominal cocoon" is a rare condition characterized by fibrosis and inflammation of the peritoneum, ultimately leading to membranous encasement of the viscera with resultant intestinal obstruction. Among the reported cases, the average age is 39 years, about two-thirds of patients are male and most afflicted patients reside in tropical or subtropical countries (Sultan Qaboos Univ Med J 2016;16:e142). The most common presenting symptom is abdominal pain. Abdominal imaging shows clumped bowel loops and abdominal/peritoneal calcification, potentially with visualization of the membrane (AJR Am J Roentgenol 2004;182:639); surgical findings are confirmatory. While early cases can be managed medically with corticosteroids or total parenteral nutrition, nearly all patients eventually undergo surgery.
Sclerosing encapsulating peritonitis can be classified into three types. Type I involves part of the small bowel, type II involves the entire small bowel, and type III extends into other adjacent organs, including the large bowel and the ovaries. A minority of cases are primary (idiopathic), with the remaining cases secondary to medication induced injury, procedure related injury, autoimmune conditions and infections such as tuberculosis (Clujul Med 2017;90:179).
Microscopically, sclerosing encapsulating peritonitis is characterized by thickened fibrocollagenous tissue extending along the serosal surface of the bowel with loss of the normal mesothelial lining. An inflammatory infiltrate may be present and lymphatics may be dilated (World J Gastroenterol 2012;18:1999).
The clinical and imaging features of sclerosing encapsulating peritonitis are quite striking and pathologists are unlikely to face a taxing differential diagnosis. The only other cause of diffuse peritoneal fibrosis is peritoneal encapsulation, a developmental anomaly that creates a thin, uninflamed accessory mesothelial membrane that rarely causes symptoms (World J Gastrointest Surg 2015;7:174). Focal fibrous appearing masses that can arise in the abdomen include desmoid type fibromatosis (which would show nuclear positivity for beta catenin), inflammatory myofibroblastic tumor (which often shows positivity for ALK1) and sclerosing mesenteritis but these should not manifest as membranes lining the small bowel serosa.
Test question answer:
C. Small bowel
