
Liver & intrahepatic bile ducts
Benign / nonneoplastic
Nodular regenerative hyperplasia
Editorial Board Member: Kimberley J. Evason, M.D., Ph.D.
Deputy Editor-in-Chief: Aaron R. Huber, D.O.
Last staff update: 1 February 2024 (update in progress)
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Nodular regenerative hyperplasia

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Diagrams / tables | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Maher P, Hernandez GD. Nodular regenerative hyperplasia. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/livertumornodularregenhyper.html. Accessed May 13th, 2024.
Definition / general
- Nodular regenerative hyperplasia (NRH) is a nonspecific pattern of liver injury that causes formation of liver nodules separated by regions of atrophy in the absence of fibrous septa
- It is a cause of idiopathic noncirrhotic portal hypertension and can mimic cirrhosis both clinically and radiologically
Essential features
- Diffuse transformation of hepatic parenchyma into regenerative, small (1 - 3 mm) nodules with no advanced fibrosis
- Associated with a variety of underlying hematologic, rheumatic and vascular disorders, as well as use of antineoplastic and immunosuppressive drugs
- Nodules are ill defined and separated by regions of atrophy (best seen on reticulin stain)
- Can lead to portal hypertension if underlying cause is not treated
- NRH and hepatoportal sclerosis / obliterative portal venopathy may coexist (Semin Diagn Pathol 2019;36:395)
Terminology
- Nodular regenerative hyperplasia
ICD coding
Epidemiology
- More prevalent in the elderly population but can be seen in children
- Associated with a variety of vascular diseases, rheumatologic diseases, hematological diseases and use of antineoplastic and immunosuppressive drugs
- Oftentimes an incidental finding on autopsies
- A cohort study of 2,500 autopsies in Canada by Dr. Ian Wanless in 1990 showed NRH present in 64 patients (2.6%) (J Investig Med High Impact Case Rep 2021;9:23247096211044617)
Sites
- Liver
Pathophysiology
- Obliteration of small portal vein radicles causes changes in hepatic blood flow
- Obliterative changes lead to decreased blood flow and atrophy and secondary nodular hyperplasia in areas with increased blood flow
- Above changes can lead to noncirrhotic portal hypertension
- Reference: Lamps: Diagnostic Pathology - Hepatobiliary & Pancreas, 1st Edition, 2011
Etiology
- There is no specific cause of the lesion, however, there are many clinical settings in which NRH can occur, including
- Vascular: portal vein agenesis, cardiac abnormalities, congestive heart failure, portal vein thrombosis, Budd-Chiari syndrome
- Autoimmune: inflammatory bowel disease, myasthenia gravis, celiac disease, primary biliary cirrhosis, scleroderma, sarcoidosis, rheumatoid arthritis, systemic lupus erythematous, polyarteritis nodosa, Beçhet disease
- Malignancy: metastatic breast cancer via portal vein metastasis, carcinoid syndrome, lymphoproliferative and myeloproliferative disorders, Castleman disease
- Other: common variable immunodeficiency, sickle cell anemia, tuberculosis
- Poisoning: arsenic, toxic oil syndrome
- Immunosuppressive agents: azathioprine, mercaptopurine, thioguanine
- Antiretroviral agents: didanosine, stavudine
- Antineoplastic agents: oxaliplatin, isoplatin, busulfan, cytosine arabinoside, chlorambucil, cyclophosphamide, bleomycin, carmustine, doxorubicin, phenytoin, gold and penicillamine
- Other agents: interleukin 2 therapy, thorotrast, methotrexate, oral contraceptives, oxymetholone, trastuzumab
- Reference: Semin Liver Dis 2014;34:240
Diagrams / tables
Images hosted on other servers:

Liver adaptive reactions overview

Proposed diagnostic criteria
Clinical features
- Underlying disease is typically evident before NRH becomes symptomatic
- NRH will typically manifest clinically as portal hypertension and its associated sequelae, including variceal bleeding, ascites, splenomegaly and gastrointestinal bleeding
- Reference: J Investig Med High Impact Case Rep 2021;9:23247096211044617
Diagnosis
- Definitive diagnosis is made on liver biopsy but there must be a high index of suspicion and cirrhosis must be ruled out before diagnosis of NRH is made
- Interobserver agreement is low even with diagnostic criteria set forth by Jharap et al. (PLoS One 2015;10:e0120299)
- Imaging modalities like magnetic resonance imaging (MRI), computed tomography (CT) and ultrasound are often employed but their sensitivities and specificities are typically low (World J Gastroenterol 2011;17:1400)
Laboratory
- Liver transaminases and serum bilirubin are usually normal, however, alkaline phosphatase can be elevated in 25% of cases (Lamps: Diagnostic Pathology - Hepatobiliary & Pancreas, 1st Edition, 2011)
Radiology description
- CT: hypodense nodules on unenhanced CT typically measuring ~1 mm (Clin Radiol 2009;64:1190)
- Ultrasound: small, round isoechoic lesions with a thin hyperechoic rim resembling a ring shaped coral reef configuration referred to as an atoll (Br J Radiol 2011;84:e129)
Radiology images
Images hosted on other servers:

Atoll lesion on ultrasound

CT scan demonstrating NRH
Prognostic factors
- Long term prognosis is uncertain, however, it is usually dependent on the level of the underlying disease causing NRH and the age of patient at diagnosis (Eur J Gastroenterol Hepatol 2010;22:1001)
Case reports
- 46 year old woman with recurrent variceal bleeding (Cureus 2022;14:e28740)
- 56 year old woman with polyarteritis nodosa (J Investig Med High Impact Case Rep 2021;9:23247096211044617)
- 58 year old man with Raynaud phenomenon (J Investig Med High Impact Case Rep 2021;9:23247096211044617)
Treatment
- Mainstay of treatment is treating the underlying etiology causing NRH
- If portal hypertension is present, then portosystemic shunts can be used
- Liver transplantation is rarely necessary and only used in cases of hepatic failure
- Reference: World J Gastroenterol 2011;17:1400
Gross description
- Vaguely nodular cut surface with the nodules having a pale appearance and the borders being darker in color (Semin Diagn Pathol 2019;36:395)
Gross images
Images hosted on other servers:

Postmortem liver
Microscopic (histologic) description
- Vague, ill defined, diffuse parenchymal nodules without fibrous septa between the nodules
- Sinusoidal dilation in areas of hepatocellular atrophy
- Inflammation is absent
- 2 morphologically distinct populations: hypertrophied hepatocytes centrally with atrophic hepatocytes on the periphery
- Atrophic hepatocytes can show feathery degeneration of the cytoplasm
- Hypertrophic cells can compress terminal hepatic venules that can appear shrunken or even be undetectable
- Hypertrophic cells can show regenerative changes (variation in nuclear size, mitotic figures and frequent binucleation)
- Within the center of nodules, there can be portal tracts known as reversed lobulation
- References: World J Gastroenterol 2011;17:1400, Semin Diagn Pathol 2019;36:395
Microscopic (histologic) images
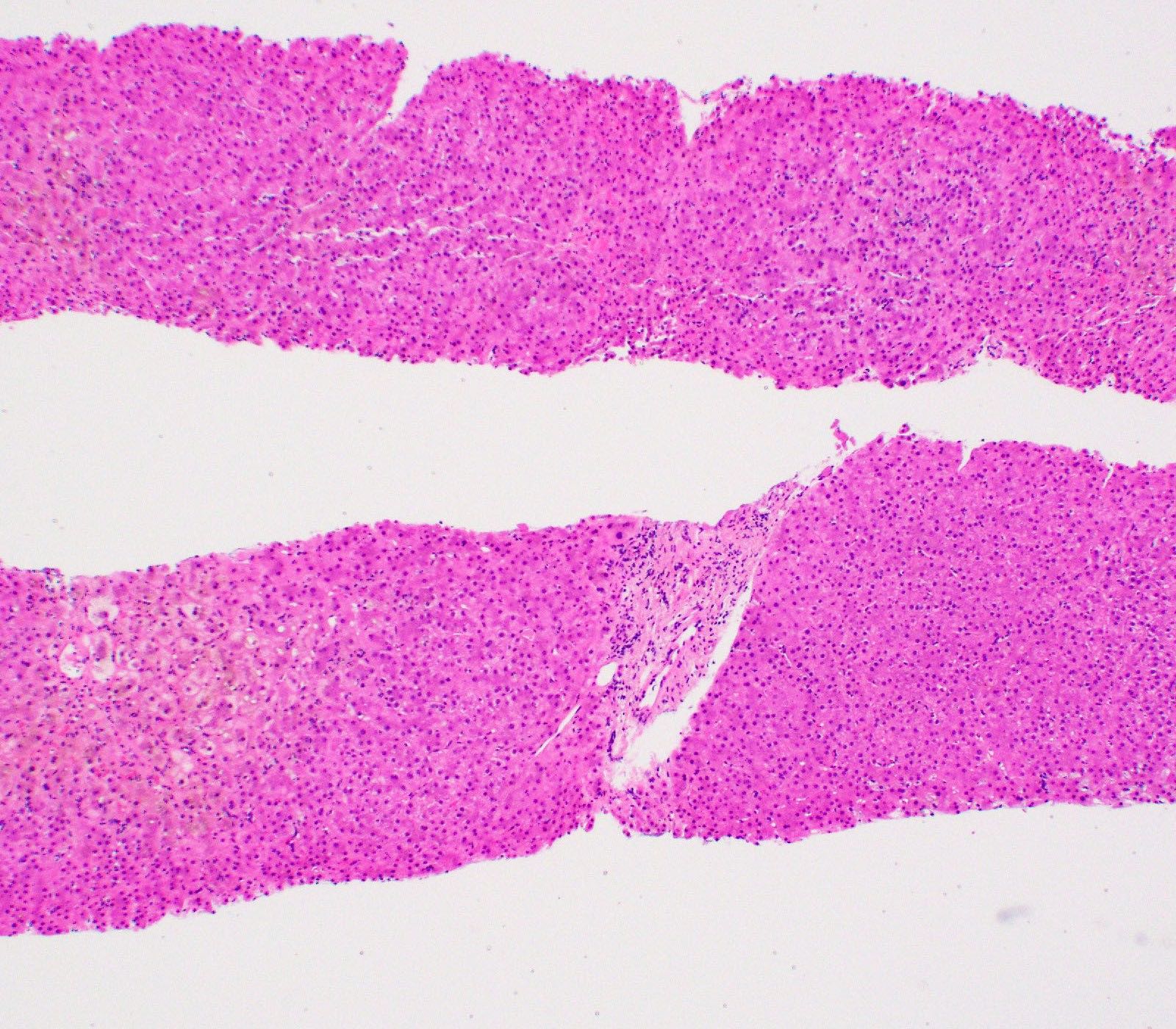
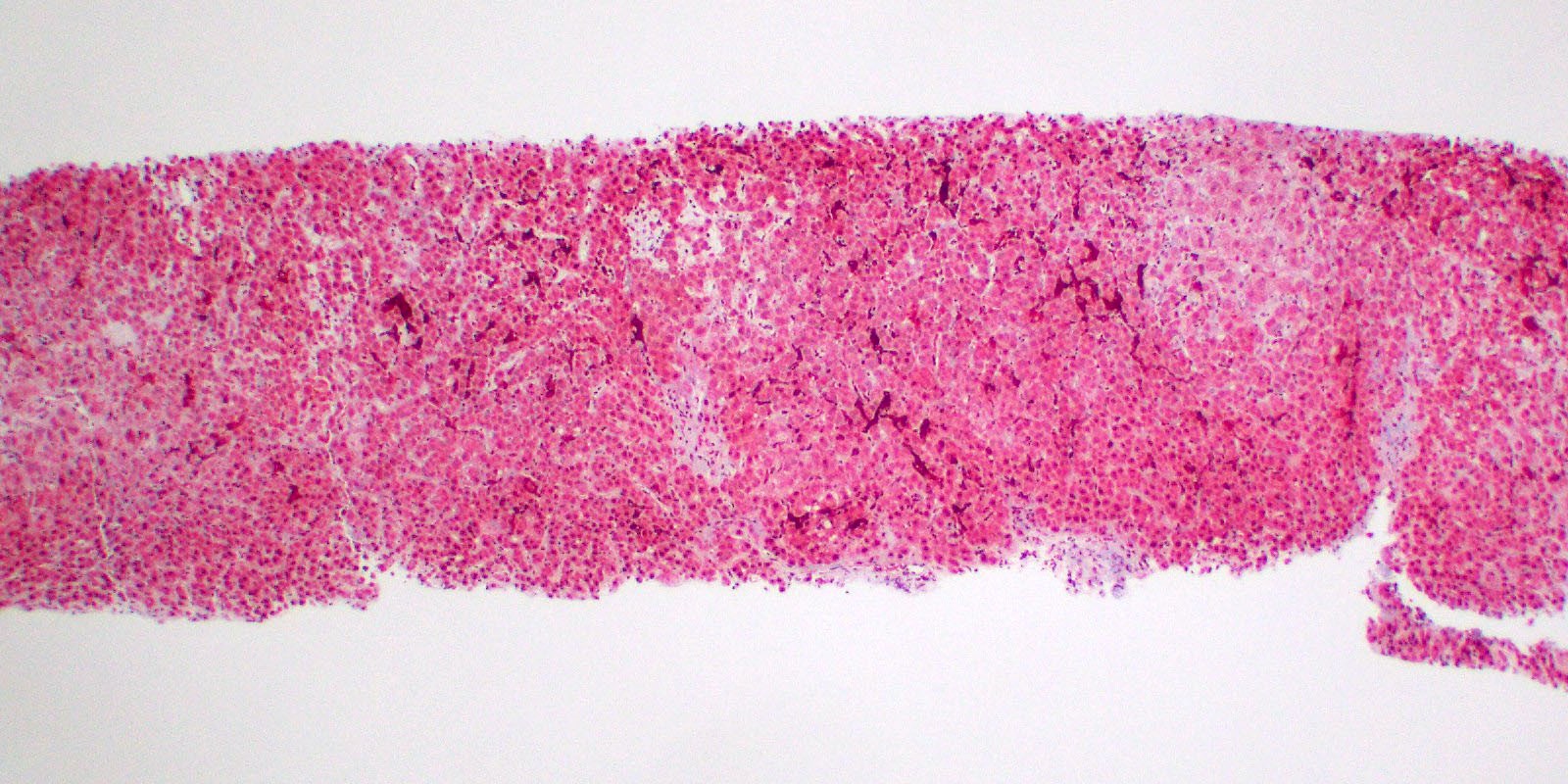
Contributed by David Hernandez Gonzalo, M.D.
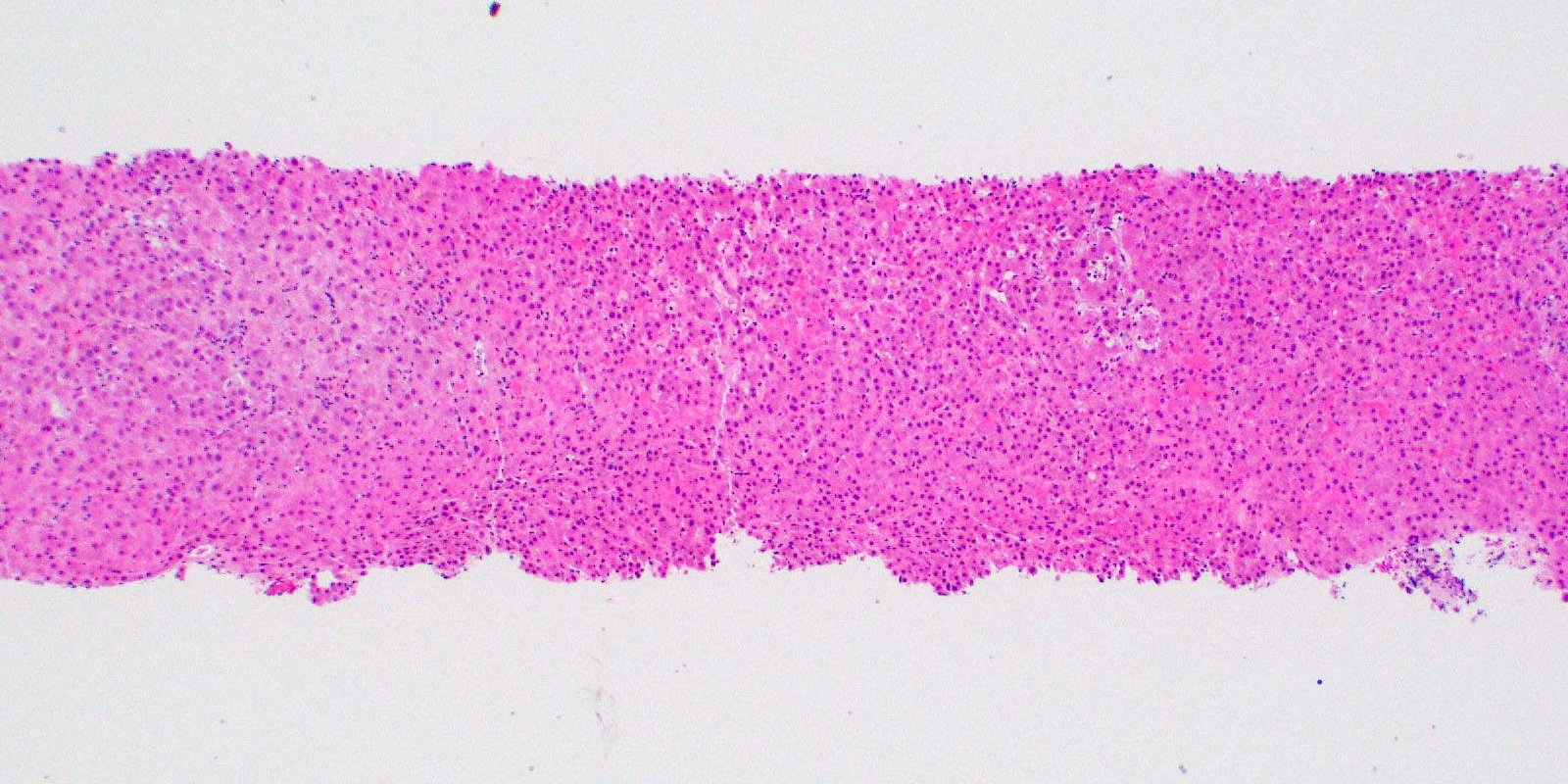
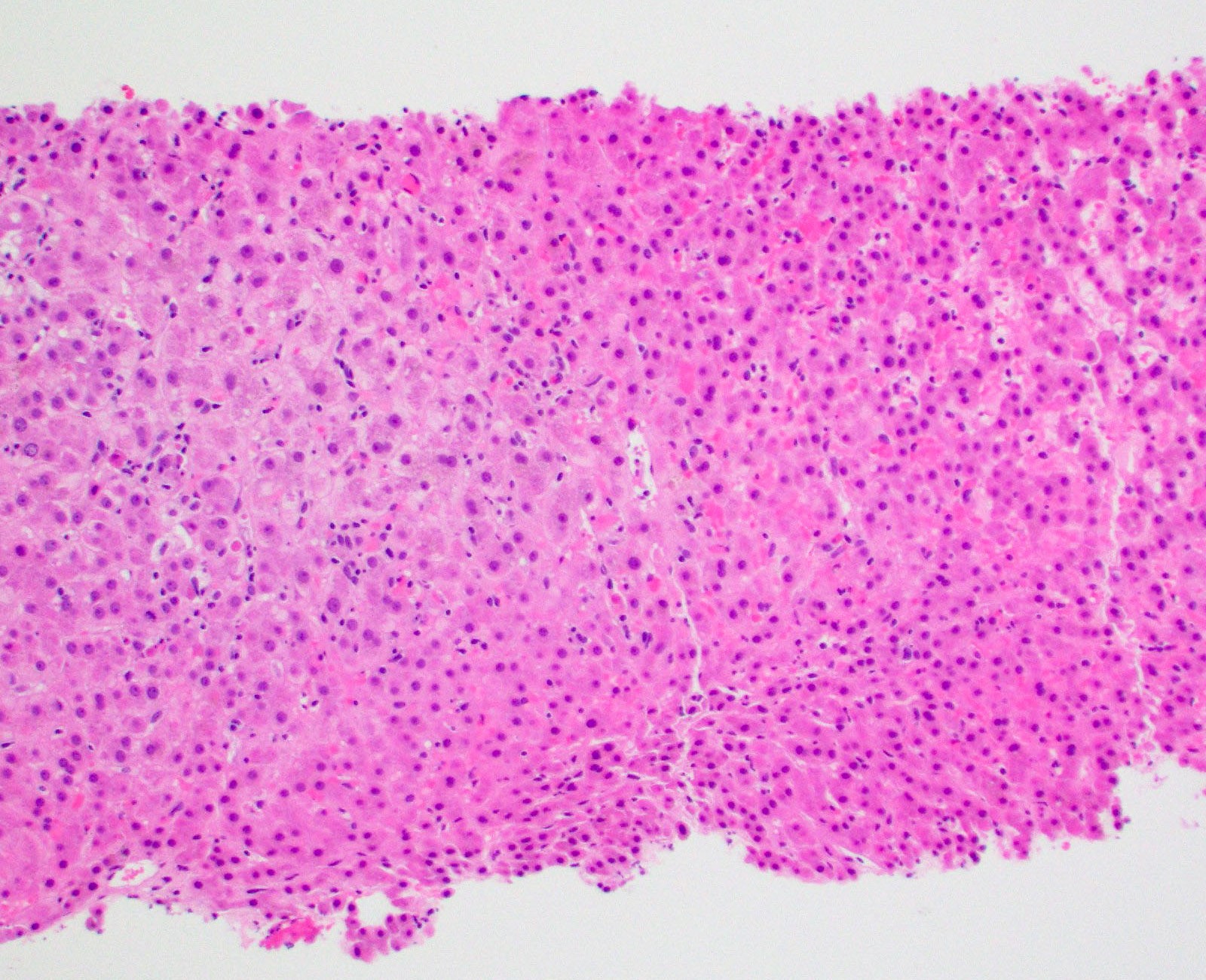
Nodules without fibrous septa
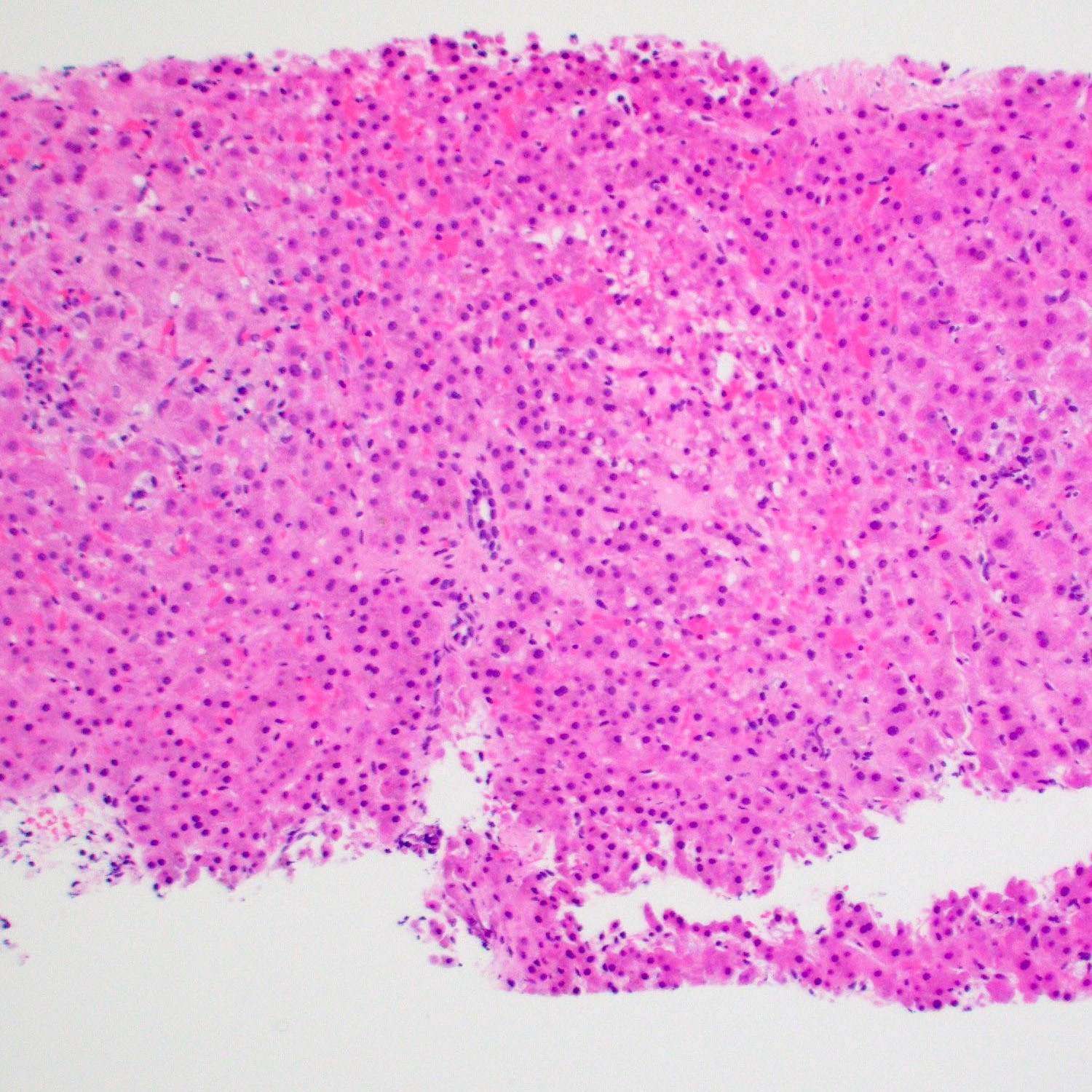
Reversed lobulation
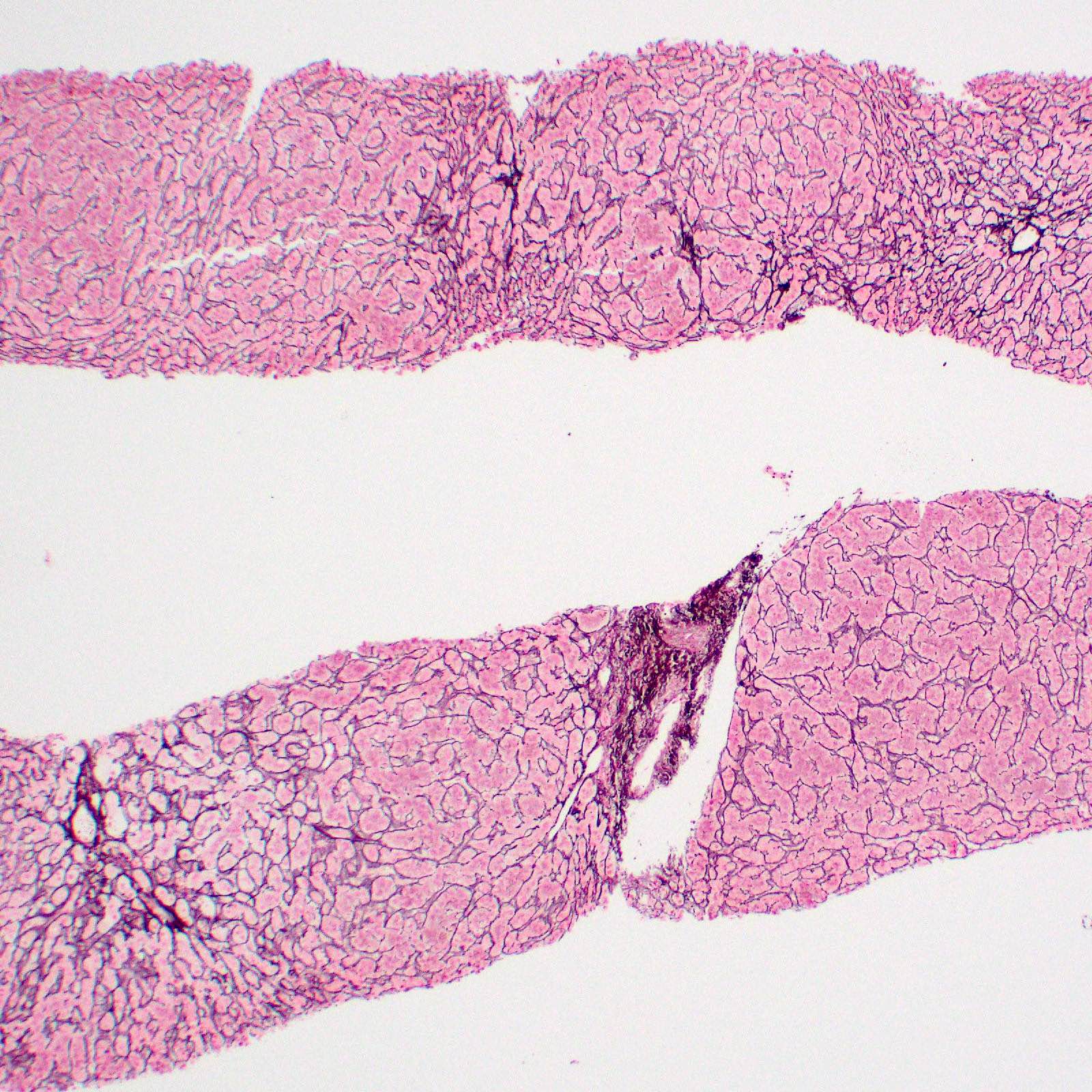
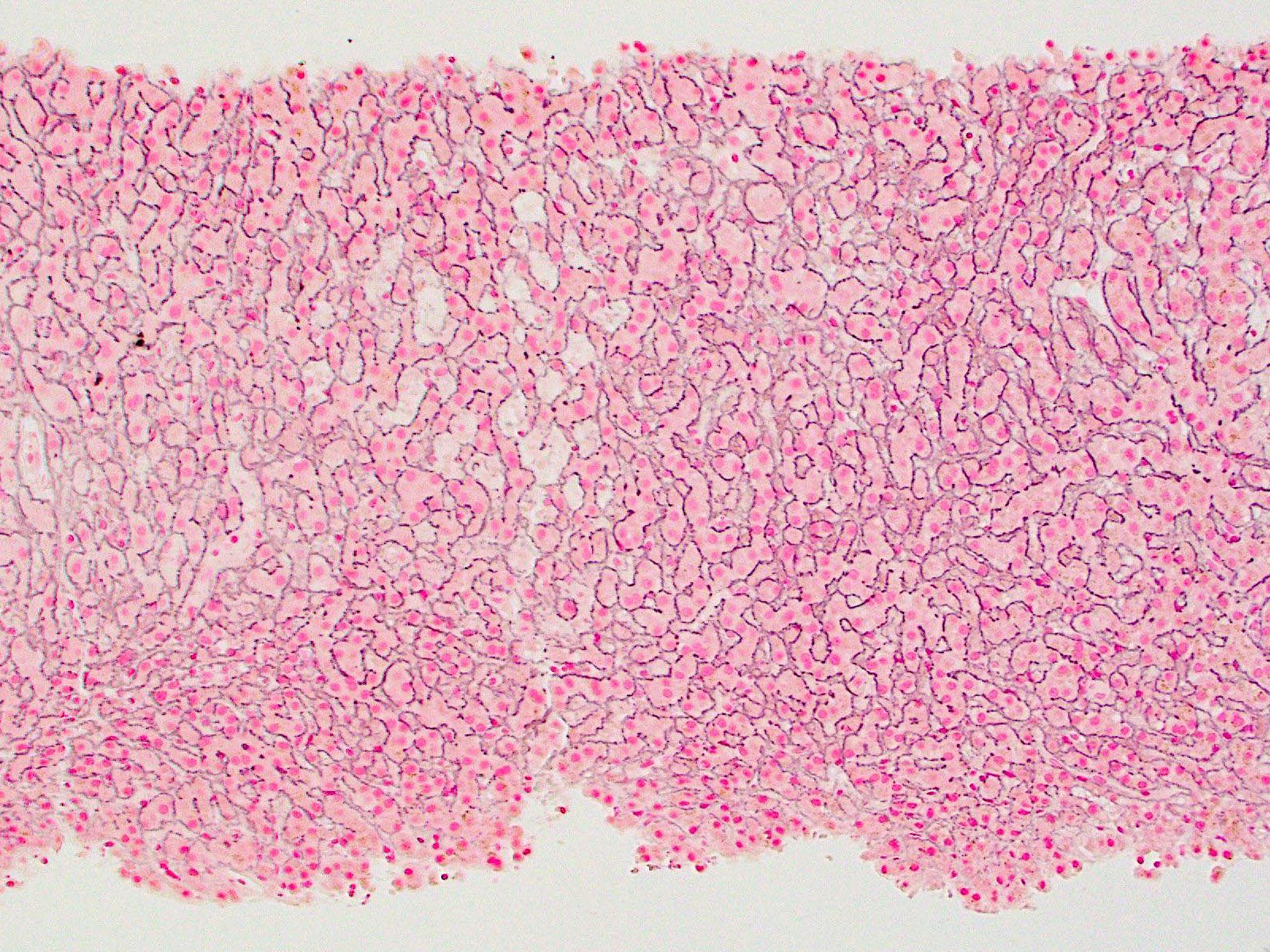
Reticulin stain
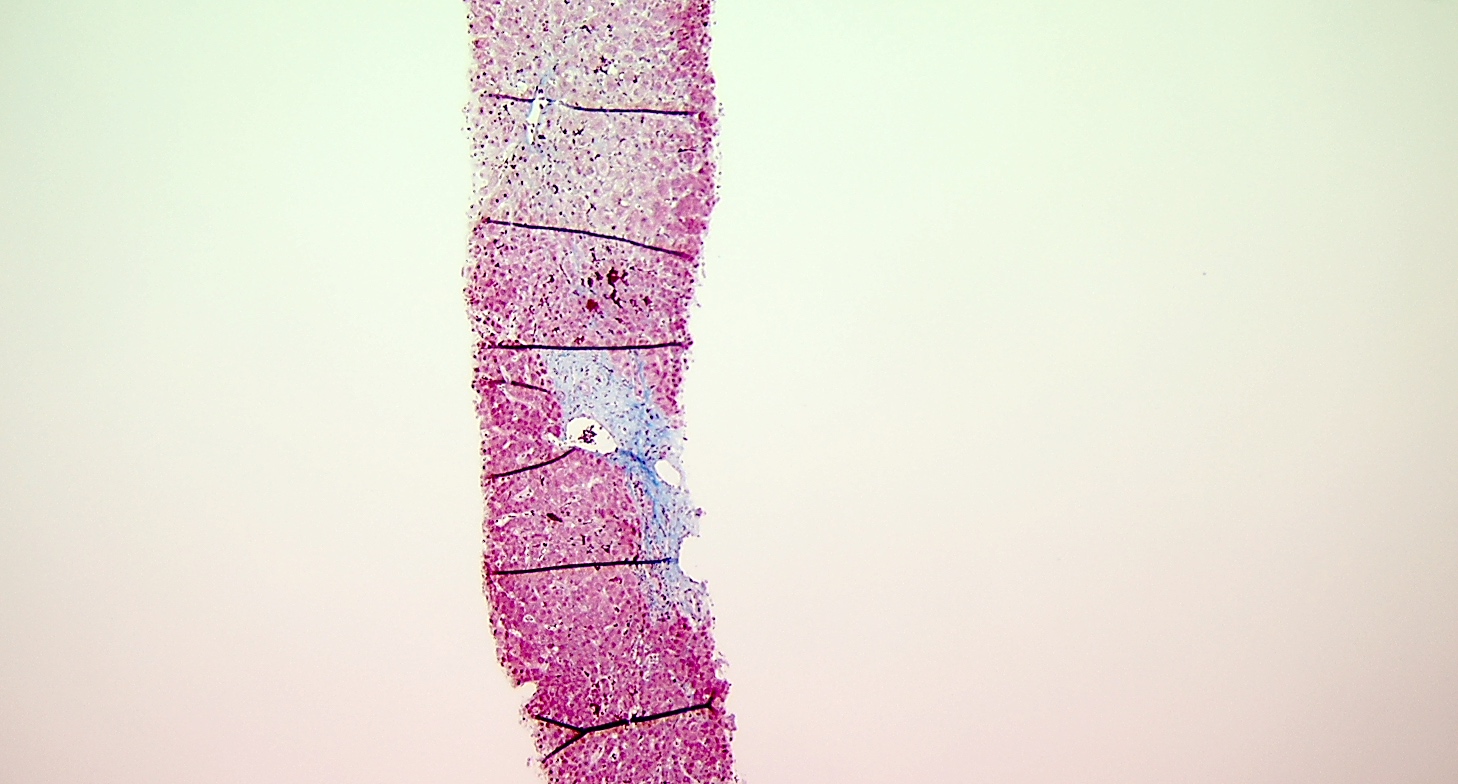
Absence of fibrosis
Positive stains
- Reticulin stain will highlight the nodules and the reticulin network will be compressed in between the nodules
Negative stains
- Trichrome stain will show no advanced fibrosis; patchy sinusoidal fibrosis may be seen
Molecular / cytogenetics description
- Methylated RASSF1A, a proapoptotic gene, has been shown to be methylated in hyperplastic hepatocytes in genetic studies (World J Gastroenterol 2011;17:1400)
Sample pathology report
- Liver, core biopsy:
- Nodular regenerative hyperplasia (NRH) (see comment)
- Comment: No significant fibrosis (trichrome stain). The patient's history of elevated alkaline phosphatase is noted. Imaging findings demonstrate diffuse nodularity. The biopsy is adequate for evaluation containing 12 portal tracts. The most striking feature corresponds to the alternating areas of hepatocyte atrophy and hyperplasia (best highlighted in reticulin stain). The portal tracts appear unremarkable with no portal inflammation or bile duct damage. There is no interface activity and the lobules demonstrate regenerative changes within the hyperplastic areas. There is no significant fibrosis on the trichrome stain. PASD stain is negative for diagnostic cytoplasmic inclusions. The overall findings, along with the patient's history of portal hypertension, are in keeping with nodular regenerative hyperplasia.
Differential diagnosis
- Cirrhosis:
- Fibrous septa around nodules are present in cirrhosis but not NRH
- Focal nodular hyperplasia:
- Solitary lesion with central scar and fibrous septa
- Aberrant arterioles and ductular reaction present
- Adenomatosis:
- Lesions are generally larger than in NRH
- Lesions generally do not involve the liver uniformly or diffusely
- Partial nodular transformation:
- Single nodule or multiple nodules at or near the hepatic hilum
- Nodules are generally larger than in NRH
- Venous outflow tract obstruction:
- Hepatocyte atrophy and necrosis can be seen but usually accompanied by sinusoidal dilatation in zone 3 of the hepatic parenchyma
- Red blood cell extravasation in space of Disse can be seen as can elongation and crowding of bile ducts with dilatation of distal bile duct radicles
- Reference: Lamps: Diagnostic Pathology - Hepatobiliary & Pancreas, 1st Edition, 2011
Board review style question #1
This liver biopsy was taken from an ill defined 2 mm nodule. What is the entity shown in this biopsy?
- Focal nodular hyperplasia
- Hepatocellular carcinoma
- Liver cirrhosis
- Nodular regenerative hyperplasia
Board review style answer #1
D. Nodular regenerative hyperplasia. The ill defined nodules have hypertrophic hepatocytes with atrophic hepatocytes. The small nodules are further highlighted on the reticulin stain and the trichrome stain shows the lack of fibrosis. Answer C is incorrect because no fibrosis is seen on trichrome stain. Answer B is incorrect because no distinct clonal population, nuclear atypia or architectural features typical of hepatocellular carcinoma are present. Answer A is incorrect because the nodules in focal nodular hyperplasia are separated by a fibrous septum. No fibrous septae are seen in the trichrome stain.
Comment Here
Reference: Nodular regenerative hyperplasia
Comment Here
Reference: Nodular regenerative hyperplasia
Board review style question #2
Nodular regenerative hyperplasia is associated with the development of which of the following?
- Cholangiocarcinoma
- Hepatocellular adenoma
- Hepatocellular carcinoma
- Hepatoportal sclerosis / obliterative portal venopathy
Board review style answer #2
D. Hepatoportal sclerosis / obliterative portal venopathy. Hepatoportal sclerosis / obliterative portal venopathy is a possible sequelae of nodular regenerative hyperplasia. Answer B is incorrect because hepatocellular adenoma has not been shown to develop from NRH. Answer A is incorrect because cholangiocarcinoma has not been shown to develop from NRH. Answer C is incorrect because hepatocellular carcinoma has not been shown to develop from NRH.
Comment Here
Reference: Nodular regenerative hyperplasia
Comment Here
Reference: Nodular regenerative hyperplasia
