

Prostate gland & seminal vesicles
Atypical / intraductal lesions
Low grade PIN
Editorial Board Member: Nicole K. Andeen, M.D.
Editor-in-Chief: Debra L. Zynger, M.D.


Last author update: 18 February 2021
Last staff update: 18 February 2021
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: low grade PIN [TIAB]
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1Cite this page: Brown ML, Tretiakova M. Low grade PIN. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/prostatelowgradePIN.html. Accessed April 26th, 2024.
Definition / general
- Intraepithelial proliferation along pre-existing ducts and acini with mild atypia, at the lower end of the prostatic intraepithelial neoplasia (PIN) spectrum
- Do NOT include in pathology reports - variability in diagnosis exists even among experts (Am J Surg Pathol 1995;19:873, Virchows Arch 2009;454:1)
Essential features
- Not recommended to report
- Often associated with high grade PIN
- PSA may be elevated
Terminology
- Formerly known as grade 1 intraductal dysplasia or PIN 1 (mild dysplasia) (Hum Pathol 1986;17:64)
ICD coding
Epidemiology
- Tends to be present in younger men, first appearing in men in their 30s - 40s (J Urol 1993;150:379)
- No increase in prostate adenocarcinoma in patients with low grade PIN (risk of carcinoma on subsequent biopsy is 18%, as compared with 19% in a man with PSA levels of 4 - 10 ng/mL and an initial benign biopsy) (BJU Int 2011;108:1394)
Sites
- No specific regions of the prostate
Pathophysiology
- Loss of function of tumor suppressors (SPRY1, SPRY2) without losses of PTEN (Proc Natl Acad Sci U S A 2012;109:20023)
Etiology
- None specific to low grade PIN
Clinical features
- No specific clinical features
- Associated with high grade PIN
Diagnosis
- Seen incidentally on prostate biopsy
Laboratory
- Elevations in PSA
Radiology description
- Normal radiologic findings
Prognostic factors
- ~ 20% of patients with low grade PIN with cancer on rebiopsy (Eur Urol 1997;32:155)
Case reports
- Ectopic prostatic adenoma in retrovesical space (J Urol 1987;137:998)
- Ectopic prostatic tissue in the uterine cervix, four cases (Am J Surg Pathol 2000;24:1224)
Treatment
- No specific treatment recommended, treatment based on higher grade lesions
Gross description
- No specific gross findings
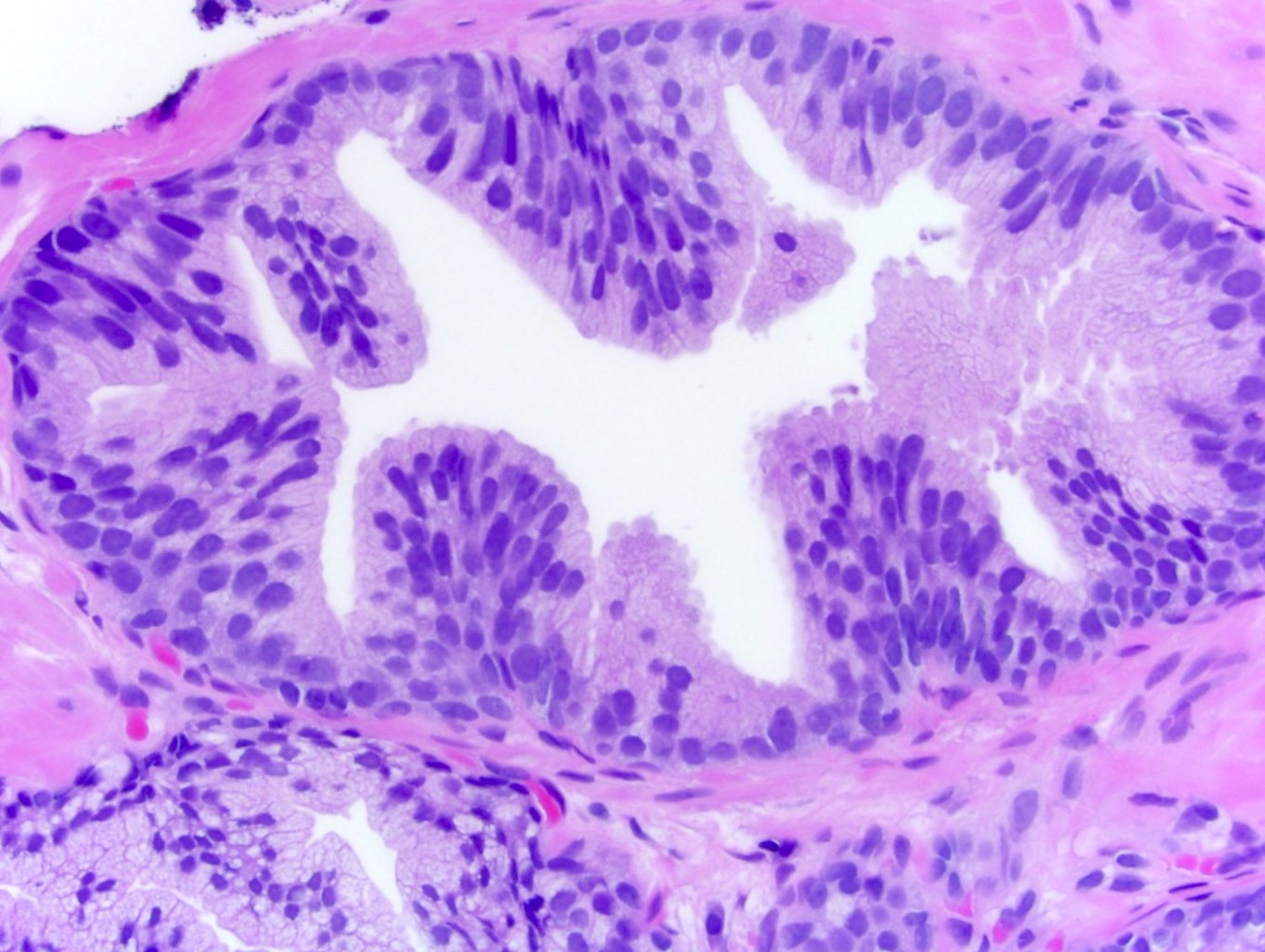
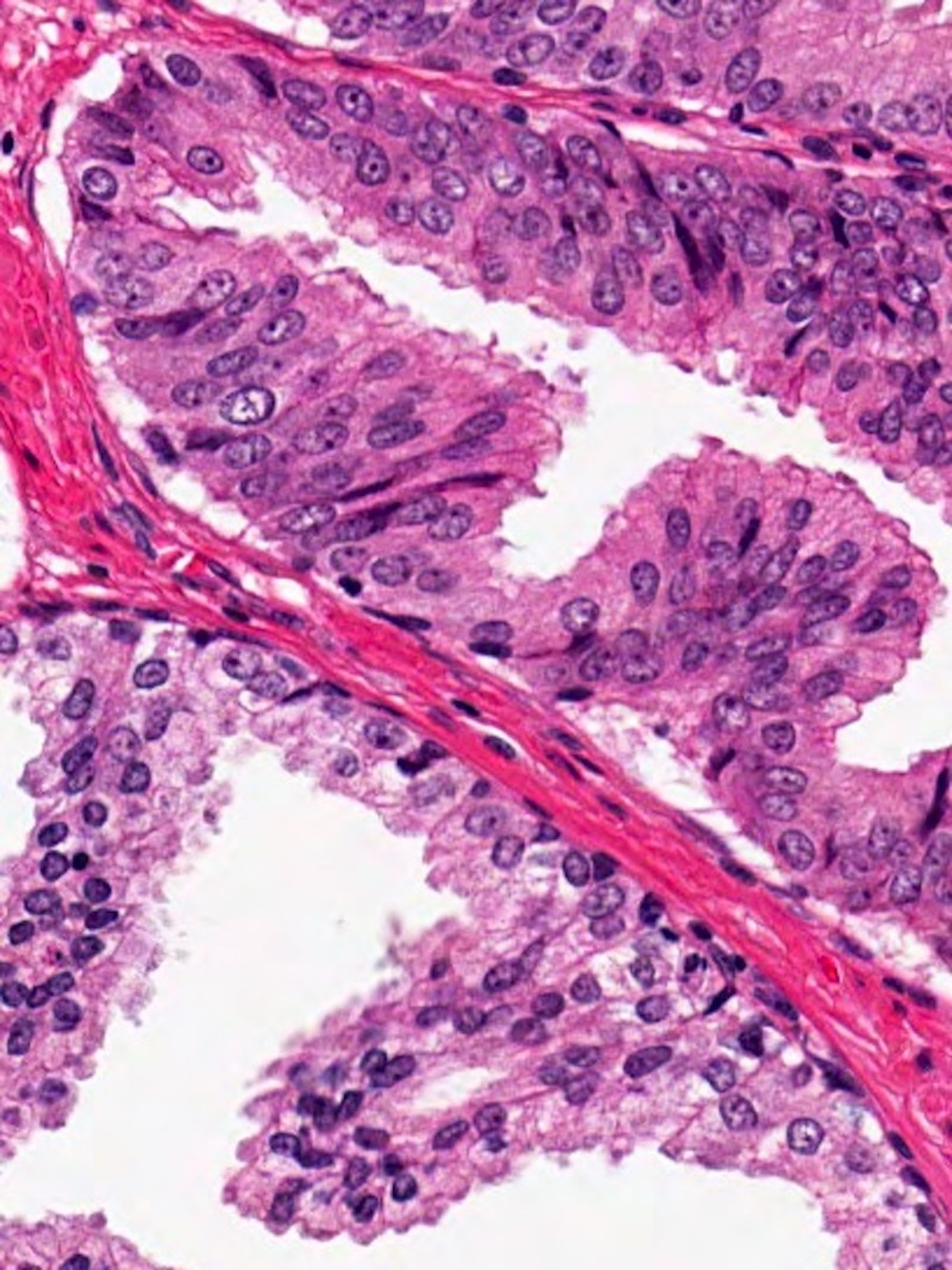
Microscopic (histologic) description
- Architecture:
- At scanning magnification, darker and more complex than normal glands
- Cellular crowding, pseudostratification with irregular spacing
- Intact basal layer
- Cytology:
- Enlarged nuclei with increased variability in nuclear size and nuclear hyperchromasia
- Indistinct and rare nucleoli
- Amphophilic or eosinophilic cytoplasm
- Reference: Virchows Arch 2009;454:1
Microscopic (histologic) images
Contributed by Nicholas P. Reder, M.D., M.P.H.

Acinar cells with crowded nuclei
Atypical acinar cells
Low grade PIN next to high grade PIN
Positive stains
- No need for IHC, although high molecular weight keratin (34βE12) and p63 will highlight a circumferential basal cell layer (BJU Int 2011;108:1394)
- Can be AMACR positive (Mod Pathol 2004;17:1180)
Molecular / cytogenetics description
- Usually diploid, in contrast with high grade PIN, which can be aneuploid
Sample pathology report
- It is not recommended to report low grade PIN
Differential diagnosis
- Benign central zone glands:
- Can have complex architecture with papillary infoldings and pseudostratified epithelium but lacking nuclear atypia
- Clear cell cribriform hyperplasia:
- Clear cells forming crowded cribriform glands without atypia and with a very prominent basal cell layer
- High grade PIN:
- Prominent nucleoli (1 - 3 microns in diameter), robust cellular crowding and multilayering
- Low grade PIN-like low grade prostatic adenocarcinoma:
- Lack of basal cells (Pathology 2014;46:88)
Additional references
Board review style question #1
The above finding may be regarded as low grade prostatic intraepithelial neoplasia. How should this be described in the pathology report?
- Benign central zone glands
- Clear cell cribriform hyperplasia
- Do not report, consider as no significant pathologic change
- High grade prostatic intraepithelial neoplasia
- Low grade prostatic intraepithelial neoplasia
Board review style answer #1
C. Do not report, consider as no significant pathologic change
Comment Here
Reference: Low grade PIN
Comment Here
Reference: Low grade PIN
