

Skin nontumor
Alopecia
Lichen planopilaris
Deputy Editor-in-Chief: Jonathan D. Ho, M.B.B.S., D.Sc.


Last author update: 16 January 2024
Last staff update: 16 January 2024
Copyright: 2020-2024, PathologyOutlines.com, Inc.
PubMed Search: Lichen planopilaris
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Immunofluorescence description | Positive stains | Negative stains | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Zare P, Ramezani M. Lichen planopilaris. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skinnontumorlichenplanopilaris.html. Accessed April 26th, 2024.
Definition / general
- Lichenoid inflammation around the hair follicle
Essential features
- Most common scarring alopecia in White populations; discoid lupus erythematosus (DLE) and central centrifugal cicatricial alopecia (CCCA) predominate in richly pigmented populations (Am J Dermatopathol 2023;45:532)
- Involvement of the infundibuloisthmic area of the hair structure with lymphocytic infiltration
- Perifollicular mucinous fibroplasia
- 3 variants
- Classic lichen planopilaris (LPP)
- Frontal fibrosing alopecia (FFA)
- Graham-Little-Piccardi-Lassueur syndrome (GLPLS)
Terminology
- Follicular lichen planus
- Frontal fibrosing alopecia (FFA)
- Graham-Little-Piccardi-Lassueur syndrome (GLPLS)
ICD coding
- ICD-10: L66.1 - lichen planopilaris
Epidemiology
- F > M
- Middle age > others
- Most commonly occurs in White patients, followed by Black patients and then patients of other races (Int J Womens Dermatol 2018;4:180)
Sites
- LPP: scalp (more common in the vertex and parietal scalp)
- FFA: frontotemporal with or without eyebrows, sideburns in males, limbs in both
- GLPLS: scalp (scarring alopecia), axilla and groin (nonscarring alopecia), trunk and extremities (hyperkeratotic follicular papules)
- References: An Bras Dermatol 2022;97:348, Front Med (Lausanne) 2021;8:737813
Pathophysiology
- Not completely understood
- Loss of immune privilege in hair follicle stem cells
- Autoimmune follicular damage by CD8+ T cell dominant lymphocytic infiltration
- Disruption of peroxisome proliferator activated receptor gamma (PPARγ) and its lipid mediator stimulants
- Epidermal - mesenchymal transition
- FOXP3 overexpression
- Mitochondrial malfunction
- Increase in M2 macrophages: LPP > FFA
- References: J Clin Med 2023;12:3259, JID Innov 2022;2:100113
Etiology
- Not completely understood
- Some reported genetic factors
- Usage of skin care products
- Local trauma
- Androgen levels: can be deficient in FFA and excess in LPP
- References: J Clin Med 2023;12:3259, JID Innov 2022;2:100113
Clinical features
- LPP (JID Innov 2022;2:100113, J Clin Med 2023;12:3259, Int J Trichology 2013;5:204)
- Asymmetric, single or multifocal patches of scarring alopecia
- Perifollicular erythema
- Follicular scar
- Follicular spine (plugging)
- Symptoms: pruritus, burning or pain
- Trichoscopy: diminished follicular ostia, perifollicular white scales and erythema, white dots, blue-gray dots with target pattern around follicles
- Lichen planopilaris activity index (LPPAI) is used for quantification of symptoms and signs (J Am Acad Dermatol 2010;62:387)
- FFA (JID Innov 2022;2:100113, J Clin Med 2023;12:3259)
- Facial and extrafacial keratotic papules
- Involvement of androgenetic dependent areas
- Postmenopausal hair loss along the frontotemporal hairline and the eyebrows
- Symmetric
- Symptoms: pruritus, burning or pain
- Trichoscopy: diminished follicular ostia, perifollicular white scales and erythema
- Frontal fibrosing alopecia severity index (FFASI) is validated for assessing FFA (Br J Dermatol 2016;175:203)
- Frontal fibrosing alopecia severity score (FFASS) is also validated for assessing FFA (J Am Acad Dermatol 2018;78:522)
- GLPLS (An Bras Dermatol 2022;97:348)
- Triad
- Scarring alopecia of the scalp
- Nonscarring alopecia of axilla and groin
- Follicular papules on trunk and extremities
- Triad
Diagnosis
- History taking
- Physical examination and trichoscopy
- Skin biopsy
- Reference: J Clin Med 2023;12:3259
Prognostic factors
- Generally can be resistant to treatment
- Some cases improve spontaneously or with treatment
- Others last for years
- Reference: Am Fam Physician 2011;84:53
Case reports
- 9 year old girl with scarring alopecia (Cureus 2021;13:e16730)
- 26 year old man with scarring alopecia of the scalp, nonscarring alopecia of the axillary and groin region and several follicular papules on his body (Clin Case Rep 2021;9:e04761)
- 36 year old White woman with basal cell carcinoma arising in association with an old LPP lesion (JAAD Case Rep 2022;29:92)
- 53 year old Black man with reticulated hyperpigmentation on his scalp (Skin Appendage Disord 2021;7:397)
- 87 year old woman with squamous cell carcinoma arising within LPP (J Dermatol Case Rep 2013;7:84)
Treatment
- Goal: to improve symptoms and stop progression of the alopecia
- No written guidelines
- Recommended therapies
- LPP (Clin Cosmet Investig Dermatol 2018;11:91, An Bras Dermatol 2022;97:348)
- Limited: topical / intralesional steroids
- Extensive
- Systemic treatment: hydroxychloroquine, methotrexate, cyclosporine, mycophenolate mofetil, pioglitazone and tofacitinib
- Topical / intralesional steroids: if limited active lesions are present
- Systemic steroids: only in severe cases to improve symptoms and stop rapid progression
- FFA (An Bras Dermatol 2022;97:348)
- Topical / intralesional steroids
- Systemic treatment: 5 alpha reductase inhibitors, hydroxychloroquine, retinoids, etc.
- LPP (Clin Cosmet Investig Dermatol 2018;11:91, An Bras Dermatol 2022;97:348)
Clinical images
Images hosted on other servers:

Frontotemporal and
eyebrow alopecia
/ multifocal scalp
alopecia

Trichoscopic view
Microscopic (histologic) description
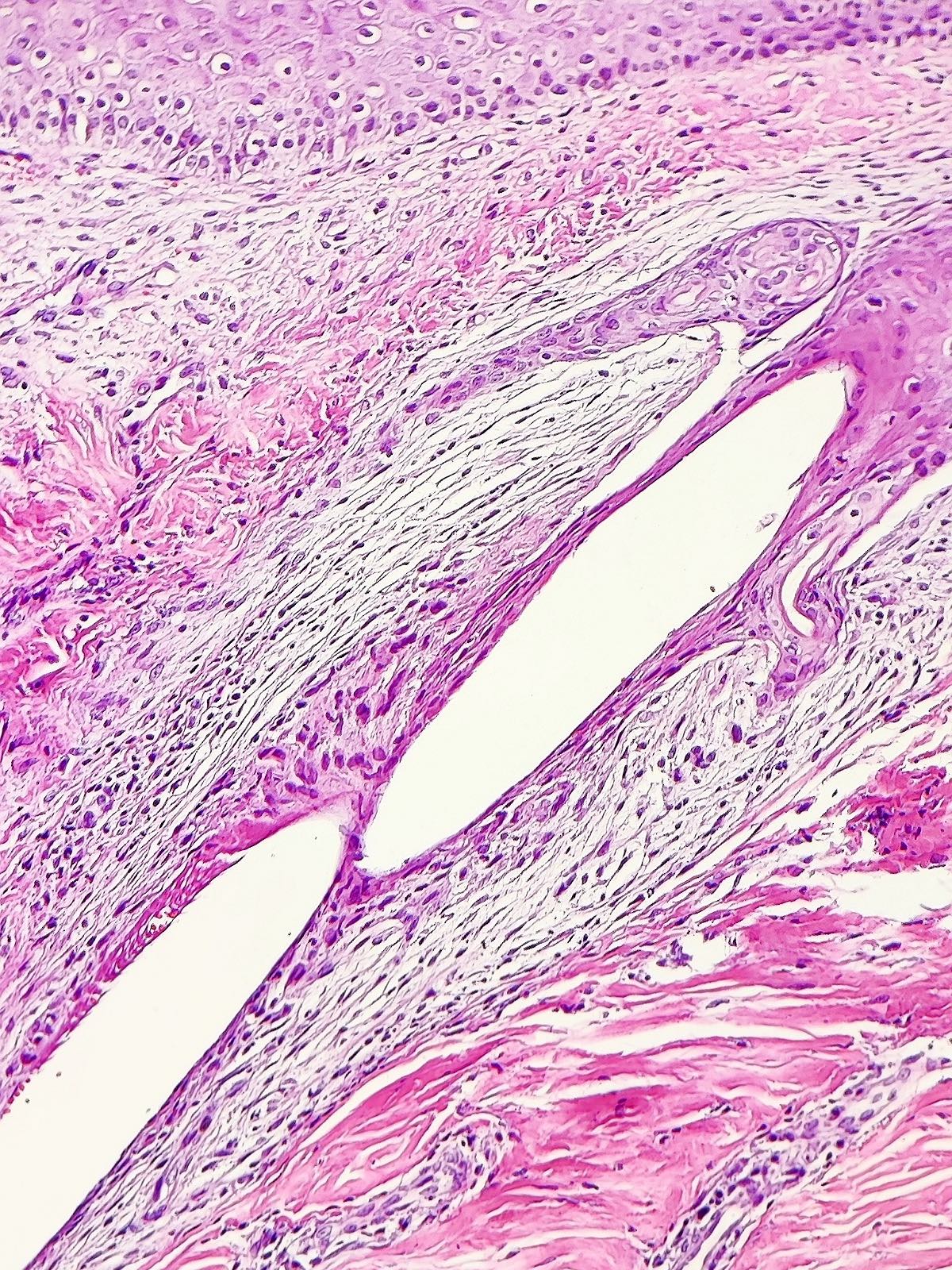
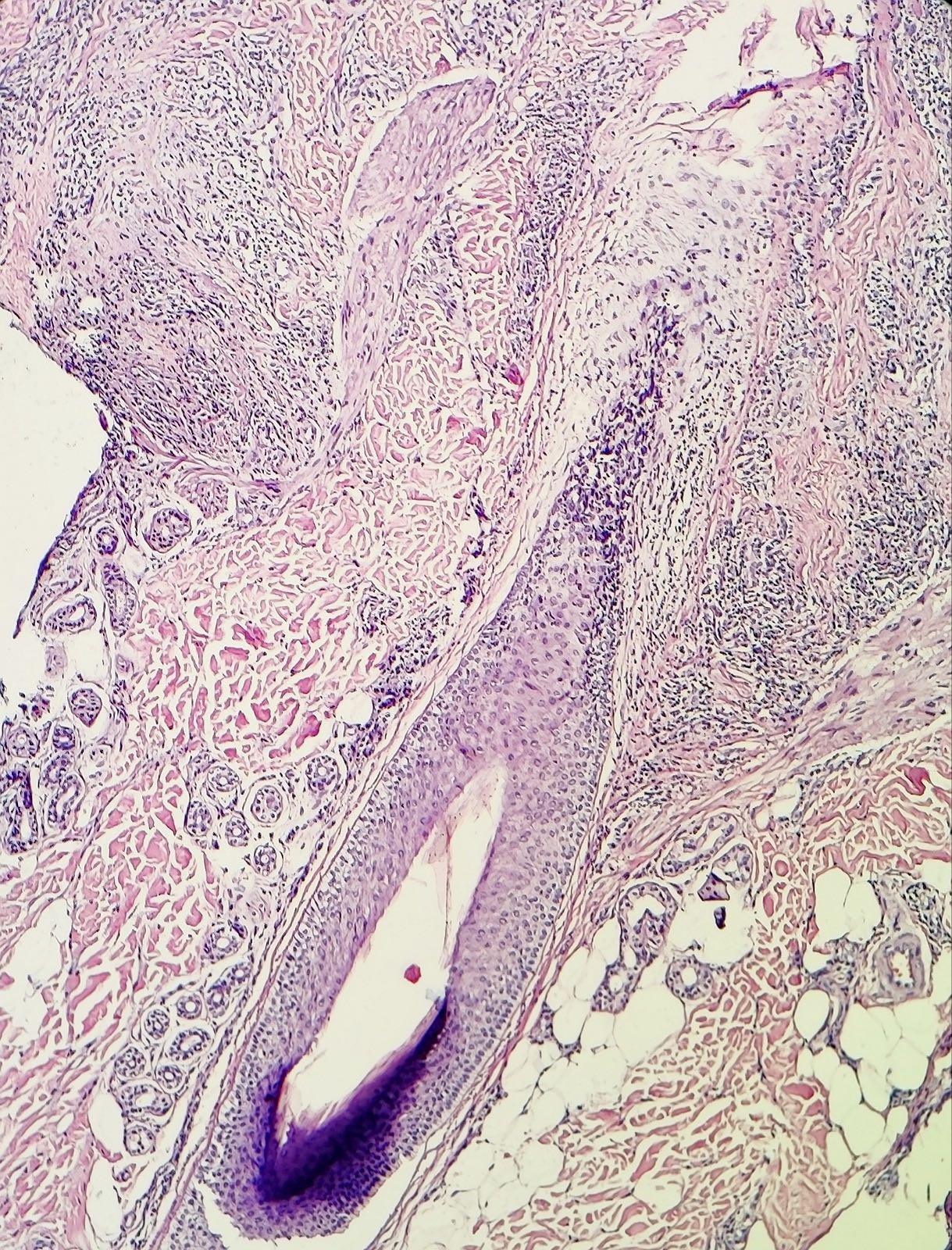
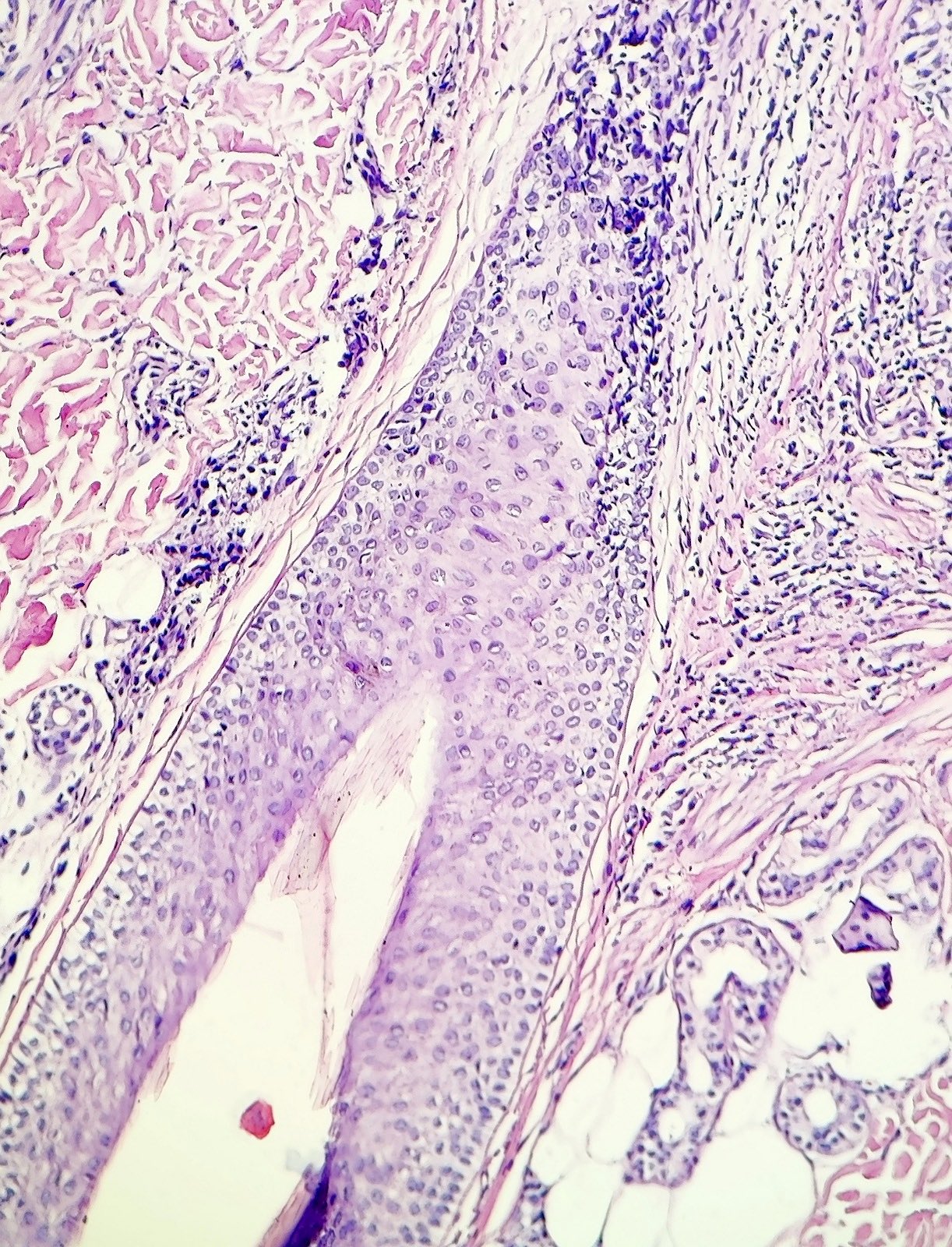
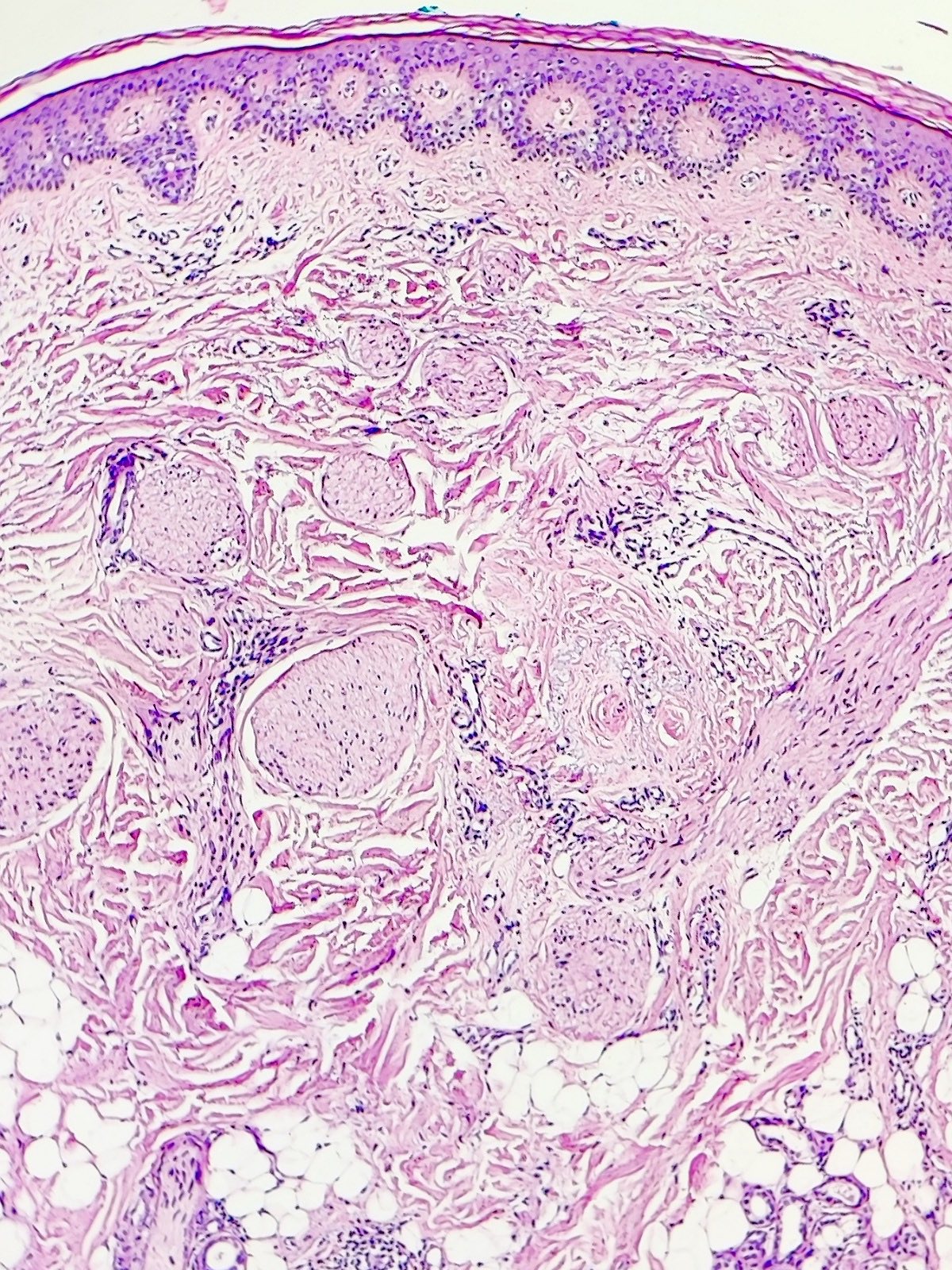
- Follicular infundibuloisthmic involvement by lichenoid infiltration of lymphocytes (hugging the collar region of the hair follicle, not deeper parts) (JID Innov 2022;2:100113, Clin Cosmet Investig Dermatol 2018;11:91)
- Deeper inflammation (mainly in FFA) does not exclude the diagnosis when there is high clinicopathologic suspicion (J Am Acad Dermatol 2017;76:1183)
- Absence or rare involvement of interfollicular epidermis with lichenoid inflammation (Clin Cosmet Investig Dermatol 2018;11:91)
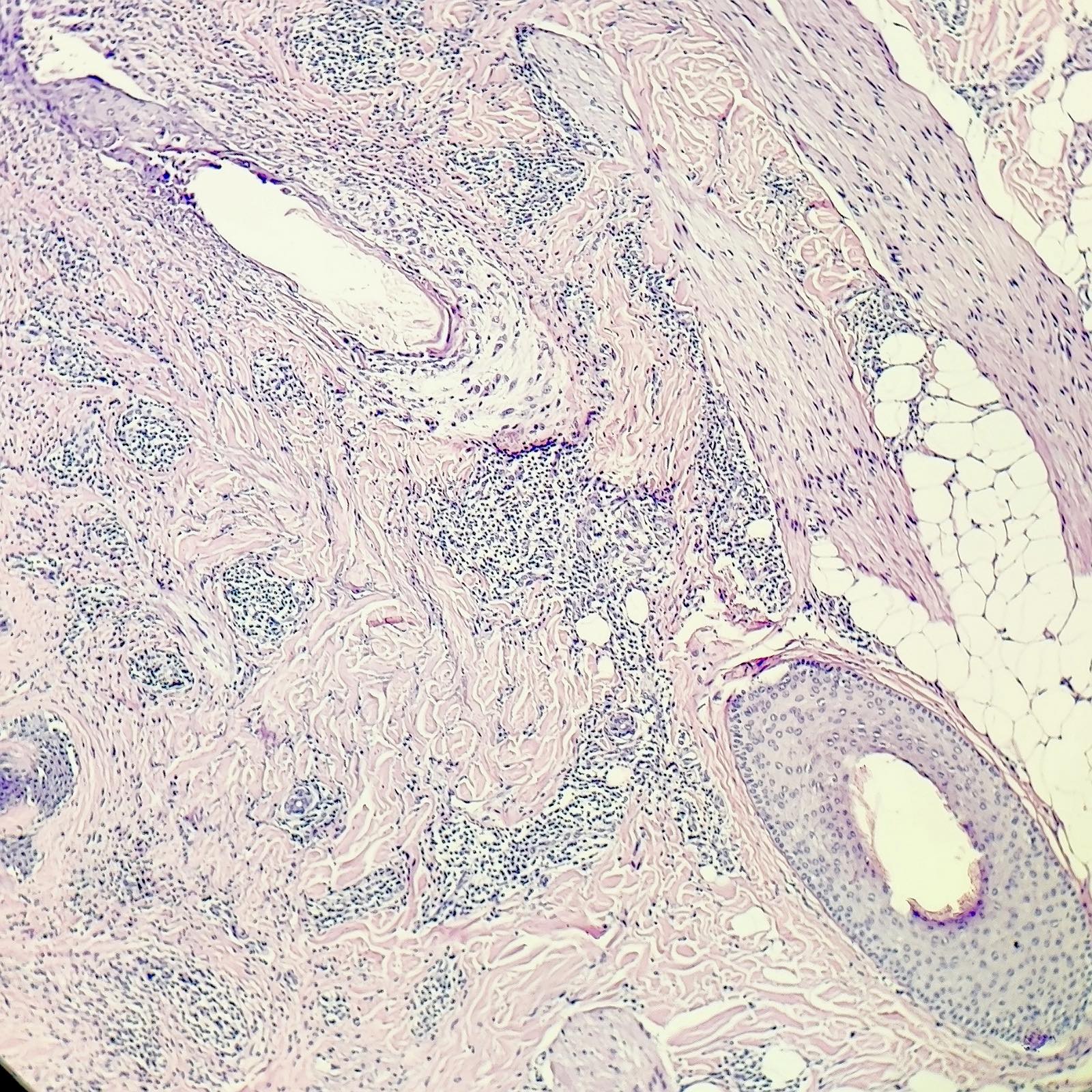
- Lymphohistiocytic and occasional eosinophilic infiltration around hair follicles (An Bras Dermatol 2022;97:348)
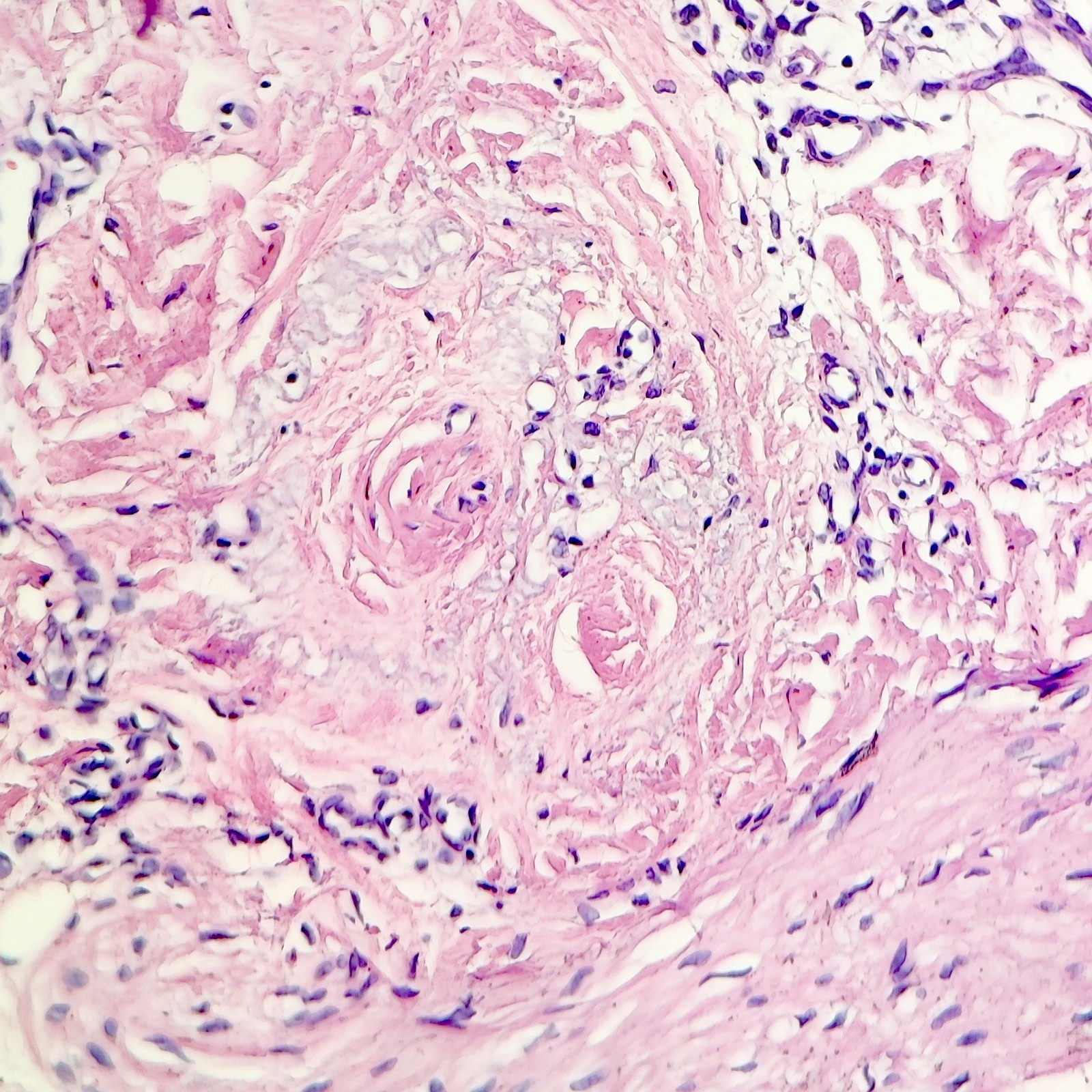
- Concentric perifollicular mucinous fibroplasia in the upper dermis (with an onion skin appearance) (Clin Cosmet Investig Dermatol 2018;11:91, JID Innov 2022;2:100113)
- Vacuolization of the follicular basal layer or squamatization at the interface of hair follicle and dermis (Front Med (Lausanne) 2021;8:737813)
- Cleft between the hair follicle and peripheral dermis (JID Innov 2022;2:100113, An Bras Dermatol 2022;97:348)
- Follicular scarring, characterized by fibrous streamers replacing hair follicles at the late stage (Front Med (Lausanne) 2021;8:737813, An Bras Dermatol 2022;97:348)
- Dilated eccrine ducts (like other scarring alopecias) (Am J Dermatopathol 2017;39:668)
- Hair tufting: tends to be in groups of 2 - 3 follicles in lymphocytic scarring alopecia (4 follicles or more in a group can be suggestive of neutrophilic causes)
- Vellus hair involvement and prominent sebaceous glands (findings in the facial papules of FFA) (Arch Dermatol 2011;147:1424, J Am Acad Dermatol 2018;78:e45)
Microscopic (histologic) images
Contributed by Pooria Zare, M.D., M.P.H. and Mazaher Ramezani, M.D.
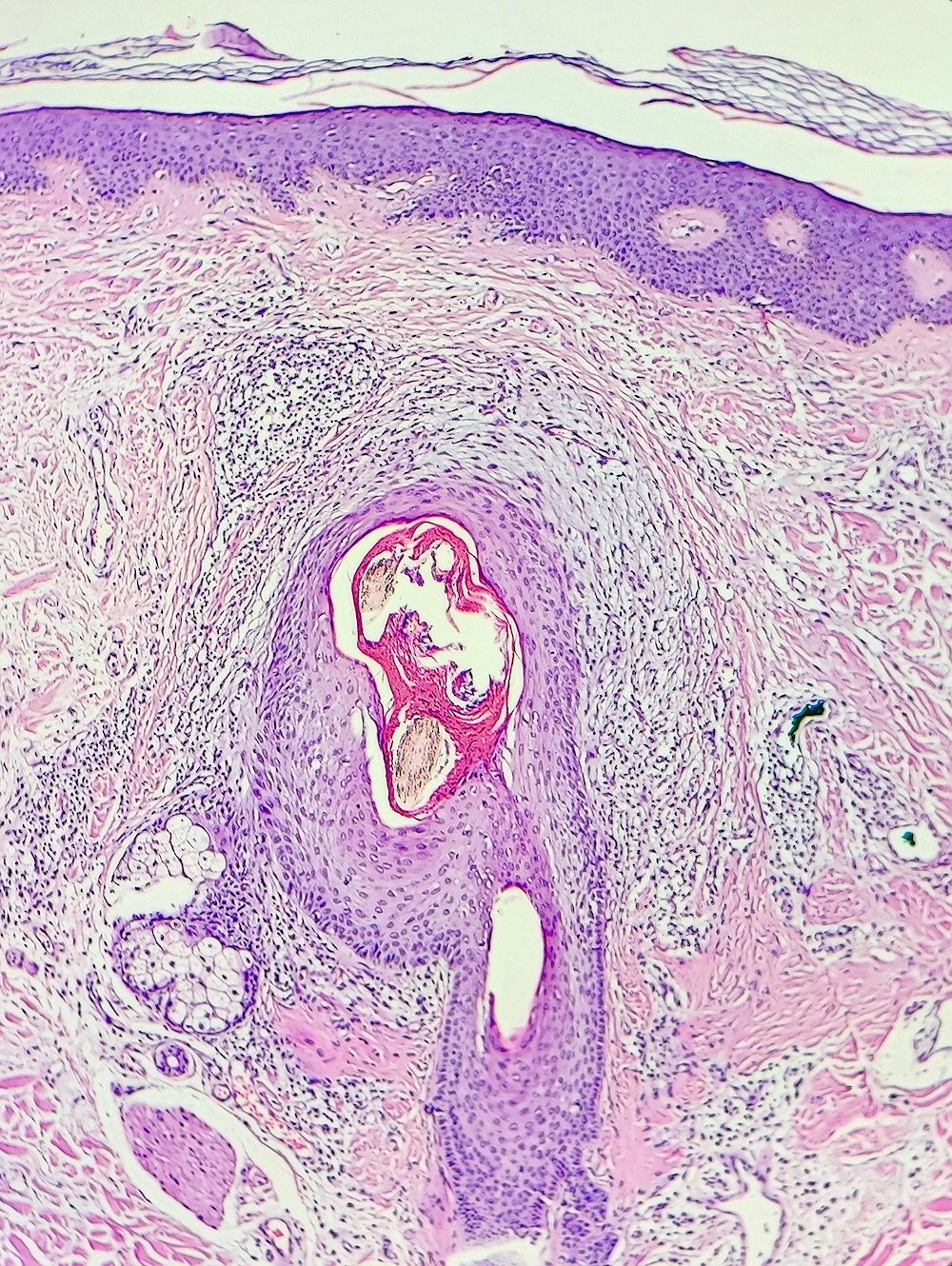
Inflammation
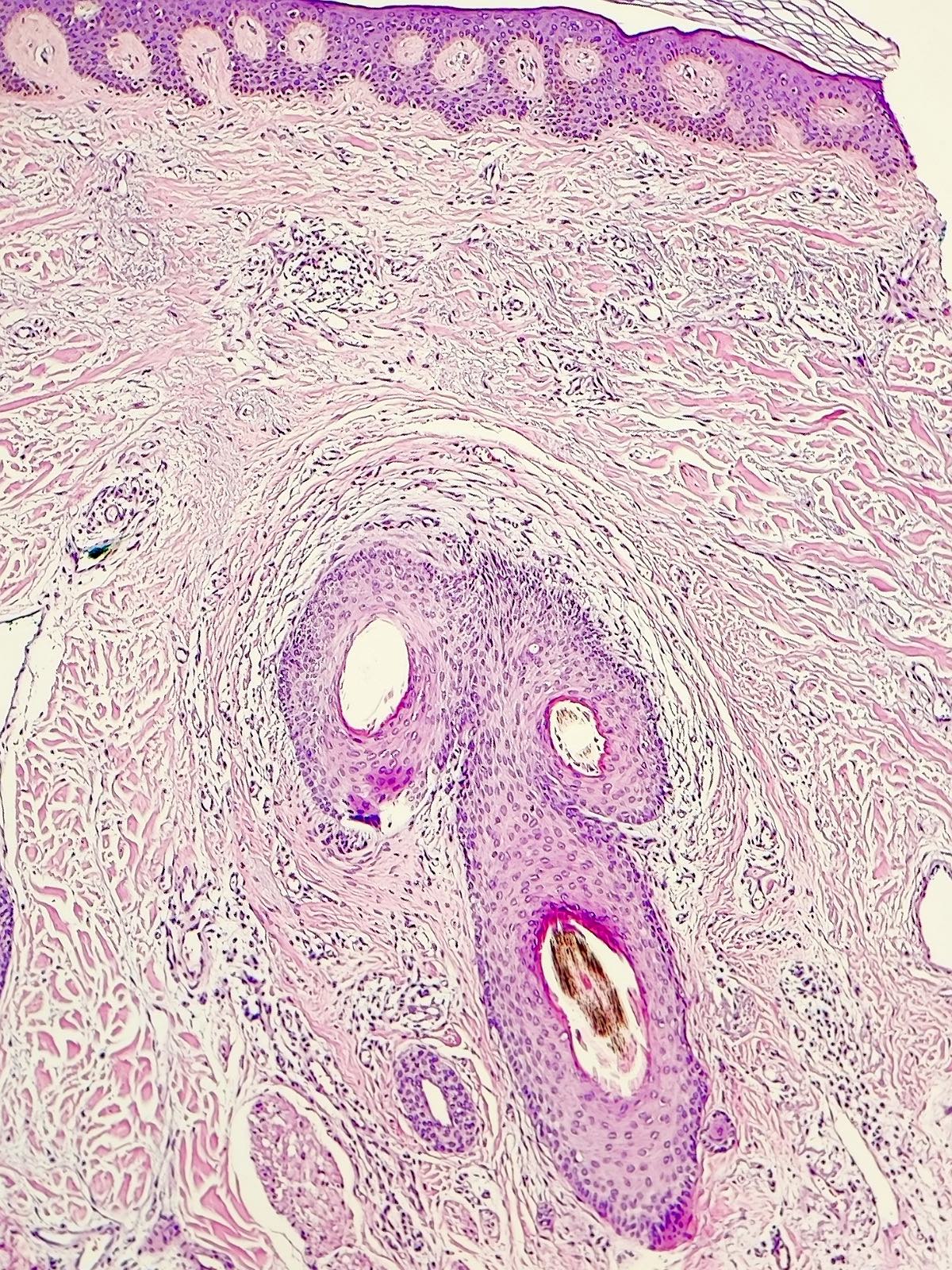
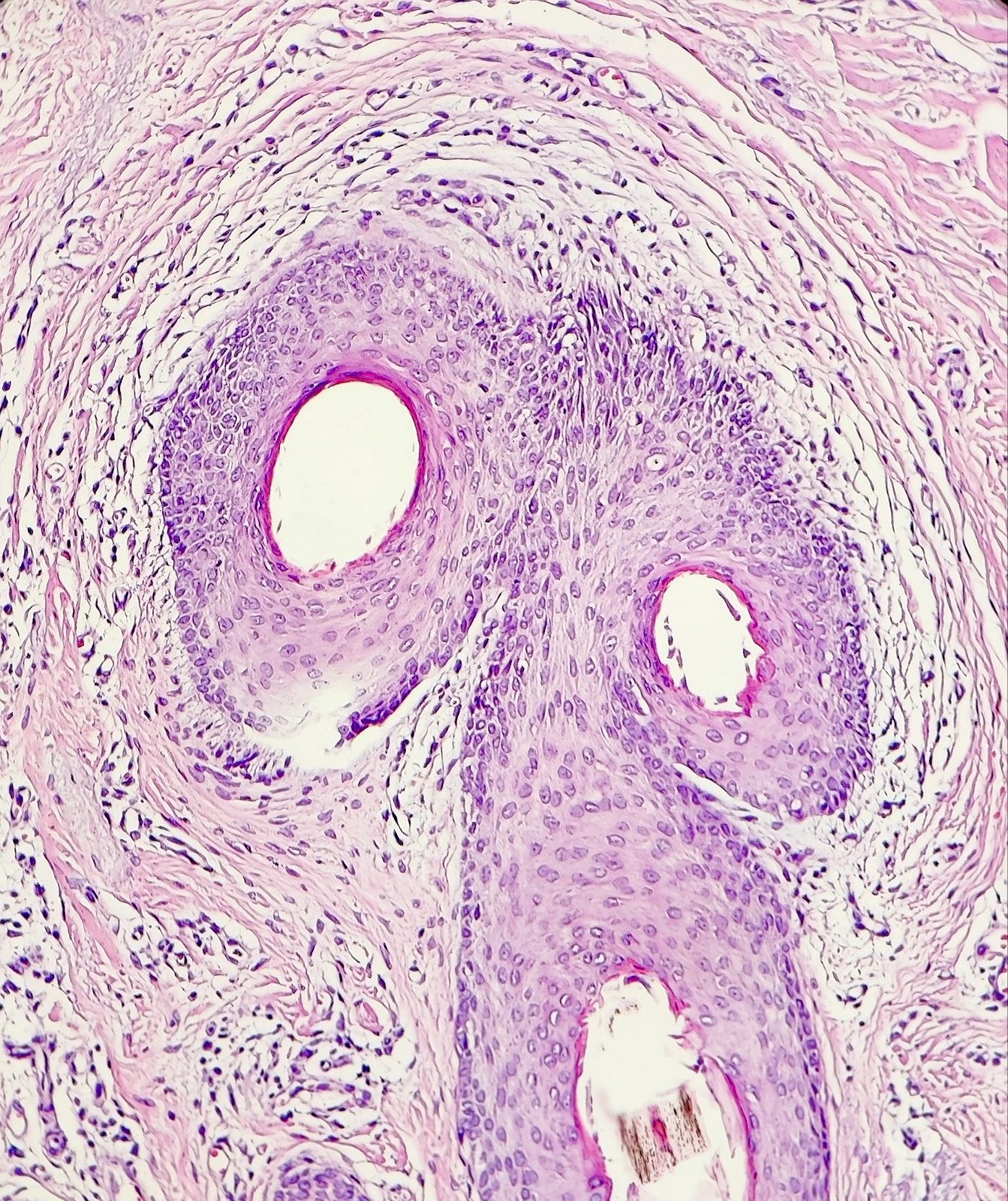
Tufting
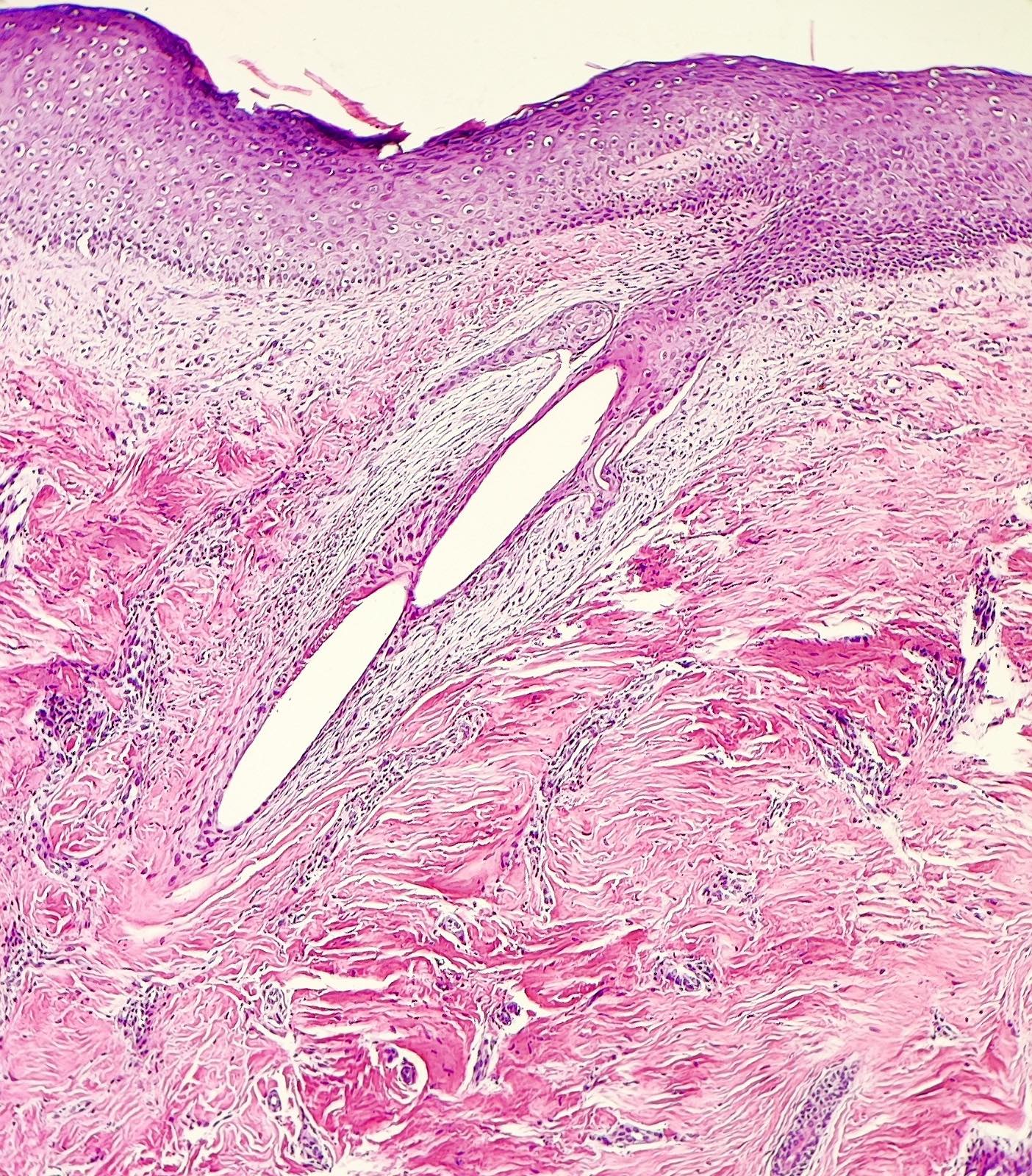
Infundibuloisthmic involvement
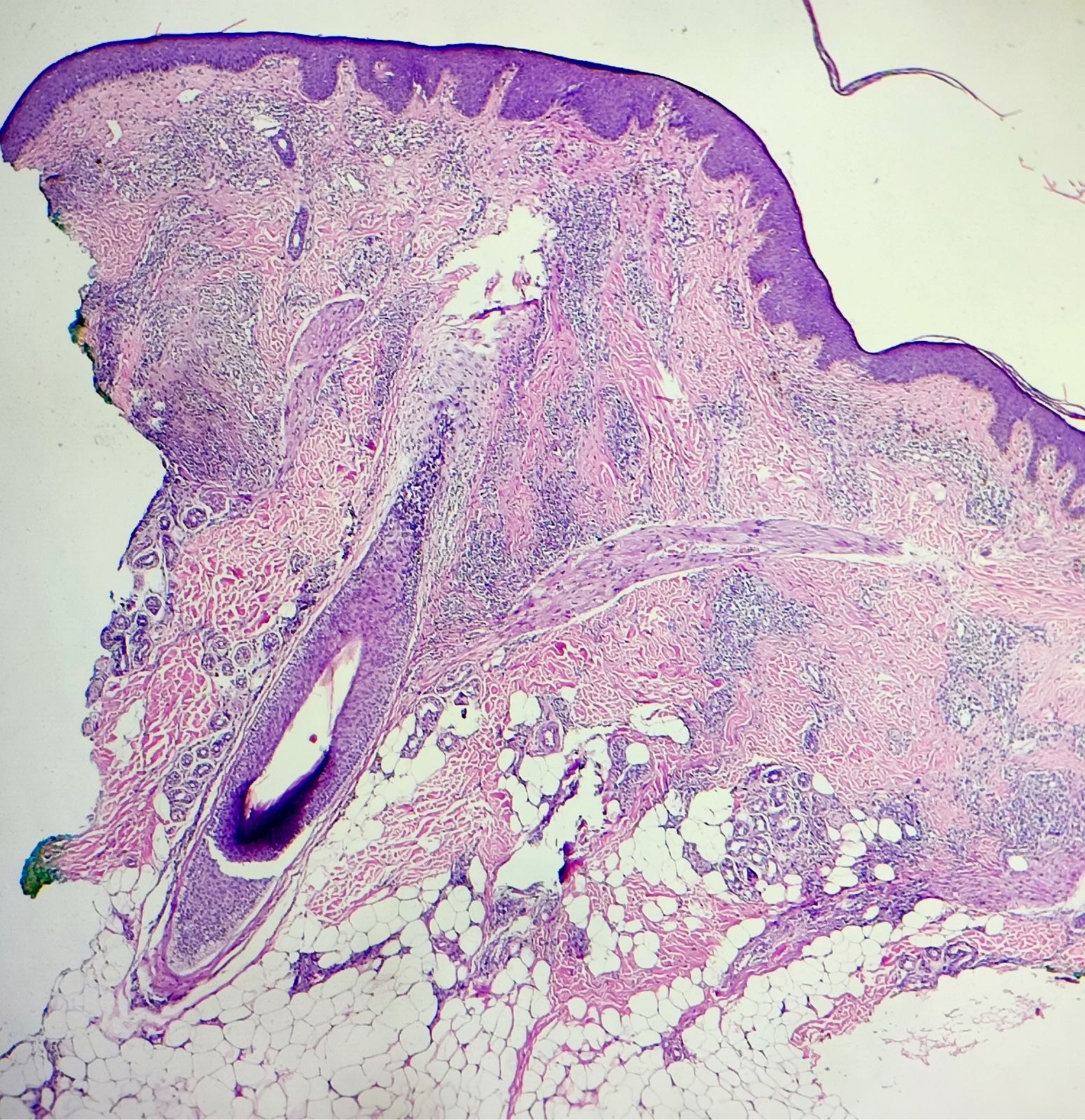
Upper follicular involvement
Scar
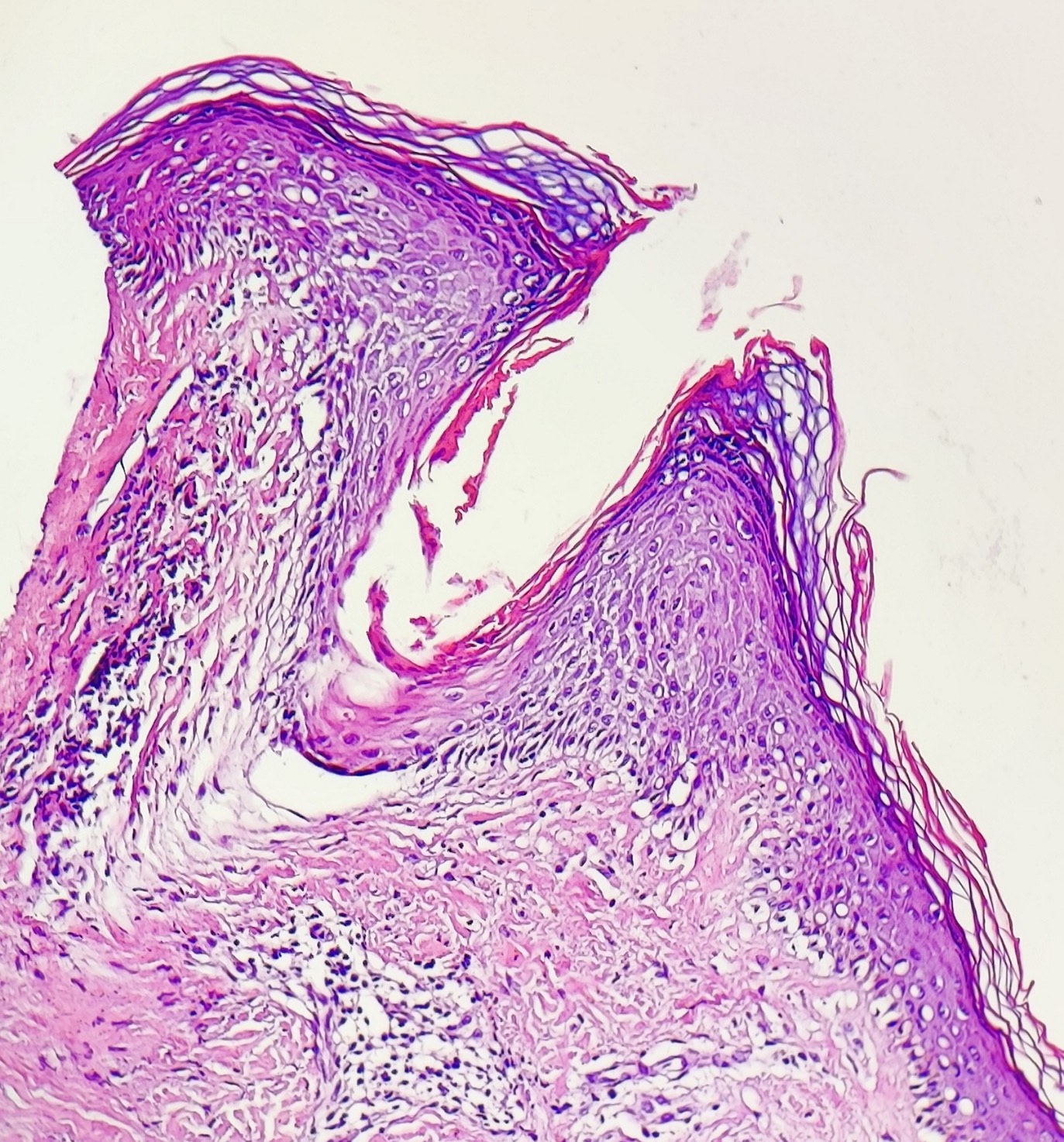
Follicular plugging
Follicular lichenoid inflammation
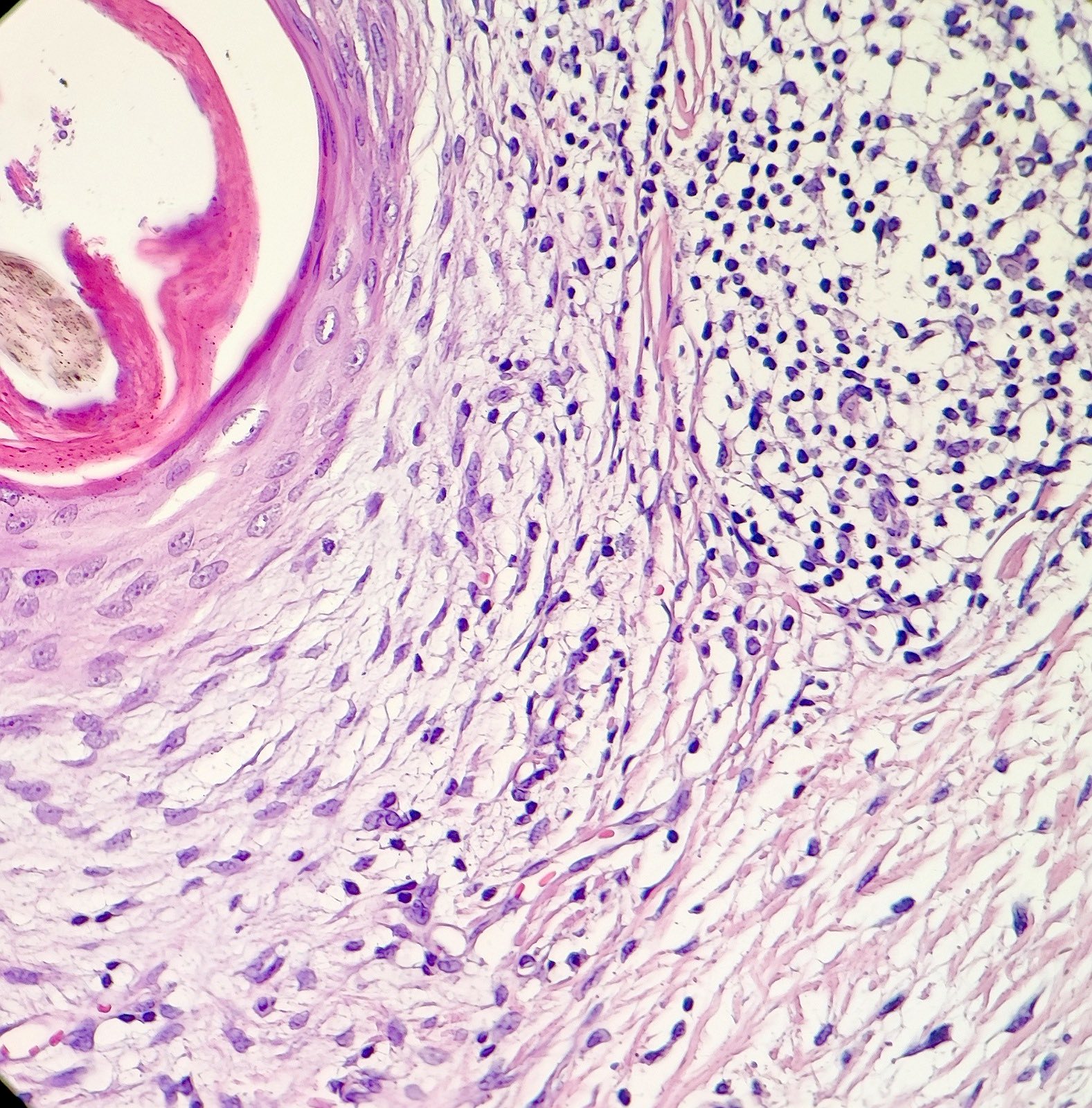
Lymphohistiocytic infiltrate and mucin
Immunofluorescence description
- Could be positive in
- Colloid bodies containing IgM or IgG in the dermis around follicular epithelium, with globular or clustered pattern (not linear)
- Papillary dermis with irregular depositions of C3 or fibrinogen
- Reference: An Bras Dermatol 2022;97:348
Positive stains
- CK903: positive in colloid bodies (Am J Dermatopathol 2016;38:353)
- CD68: more positive cells in LPP than FFA (An Bras Dermatol 2022;97:348, J Clin Med 2023;12:3259)
Negative stains
- CD123: highly specific in distinguishing DLE from LPP, especially when large clusters (10 or more cells) of plasmacytoid dendritic cells are present (An Bras Dermatol 2020;95:307, Int J Trichology 2020;12:62, Postepy Dermatol Alergol 2022;39:298)
Sample pathology report
- Skin, scalp, punch biopsy:
- Lymphocytic scarring alopecia compatible with lichen planopilaris (see comment)
- Comment: Infundibuloisthmic involvement and perifollicular mucinous fibroplasia are features in favor of diagnosis. Clinicopathologic correlation is recommended.
Differential diagnosis
- Discoid lupus erythematosus (DLE):
- Interfollicular epidermal involvement with lichenoid inflammation or vacuolization
- Thick and tortuous epidermal basement membrane
- Patchy lymphoplasmacytic infiltration of the superficial and deep (periadnexal and perivascular) dermis
- Interstitial mucin deposition
- Perieccrine inflammation
- Dermal clusters of CD123 positive plasmacytoid dendritic cells
- Folliculitis decalvans:
- Mixed neutrophilic and lymphoplasmacytic inflammation
- Absence of interface change in dermoepidermal junction
- Central centrifugal cicatricial alopecia:
- Mixed neutrophilic and lymphocytic inflammation
- Syringoma-like dilated eccrine ducts (nonspecific, may be seen in other scarring alopecias; clinicopathologic correlation is necessary) (Am J Dermatopathol 2017;39:668)
- Pseudopelade of Brocq:
- End stage scarring alopecia
- Most common cause of this disease is LPP
Additional references
Board review style question #1
Which of the following features is most typical in the above case of lichen planopilaris (LPP) / frontal fibrosing alopecia (FFA)?
- Extension of inflammation to the subcutis
- Follicular tufting
- Involvement of the upper portion of the follicle
- Presence of miniaturization of hairs
Board review style answer #1
C. Involvement of the upper portion of the follicle. The picture shows a case of lichen planopilaris with involvement of the upper portion of the follicle, which is a hallmark of the disease. Answer D is incorrect because miniaturization of hairs is mostly seen in androgenetic alopecia and is not a feature of classic LPP. Answer B is incorrect because follicular tufting may be seen in LPP but it is also observed in other cases with follicular invasion by inflammatory cells, including folliculitis decalvans. Answer A is incorrect because the extension of inflammation to the subcutis is not a prominent feature in LPP; it is more commonly seen in discoid lupus erythematosus (DLE).
Comment Here
Reference: Lichen planopilaris
Comment Here
Reference: Lichen planopilaris
Board review style question #2
What is the most common cause of lymphocytic scarring alopecia in White predominant populations?
- Discoid lupus erythematosus
- Folliculitis decalvans
- Lichen planopilaris
- Pseudopelade of Brocq
Board review style answer #2
C. Lichen planopilaris. The most common cause of lymphocytic scarring alopecia is classic lichen planopilaris (LPP). Answer A is incorrect because discoid lupus erythematosus (DLE) is one of the examples of lymphocytic scarring alopecia but it is not the most common. It is associated with patchy lymphoplasmacytic infiltration of the superficial and deep dermis, including periadnexal and perivascular areas. Answer D is incorrect because pseudopelade of Brocq represents end stage scarring alopecia, mainly characterized by the absence of inflammation. Answer B is incorrect because folliculitis decalvans involves follicles with inflammatory cells, including lymphocytes, neutrophils and plasma cells.
Comment Here
Reference: Lichen planopilaris
Comment Here
Reference: Lichen planopilaris
