
4 August 2005 - Case #15
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Peter Morawiecki, Great Lakes, Illinois, USA.

Case #15
Clinical history:
A 62 year old Black man had a more than 1 year history of a slowly enlarging thumb mass. Clinically, it was believed to be an epidermal cyst. Xrays failed to show any abnormalities.
Microscopic images:

What is your diagnosis?
Diagnosis: Aggressive digital papillary adenocarcinoma
Discussion:
Aggressive digital papillary adenocarcinoma is a rare sweat gland tumor that occurs primarily on the digits of the hands and feet and adjacent skin. Although these tumors were initially divided into adenomas and adenocarcinomas, a recent AFIP study concluded that histologic features could not predict which tumors would act aggressively and the authors recommended that all of these tumors be called adenocarcinomas (Am J Surg Pathol 2000;24:775).
These tumors primarily affect males, with a mean age of 52 years (range: 19 - 83 years). Average tumor size is 2 cm (range: 0.4 - 4 cm) and tumors are present for an average of 2 - 3 years before excision. They are usually (85%) on the hand, with the remainder on the feet. They frequently are associated with pain.
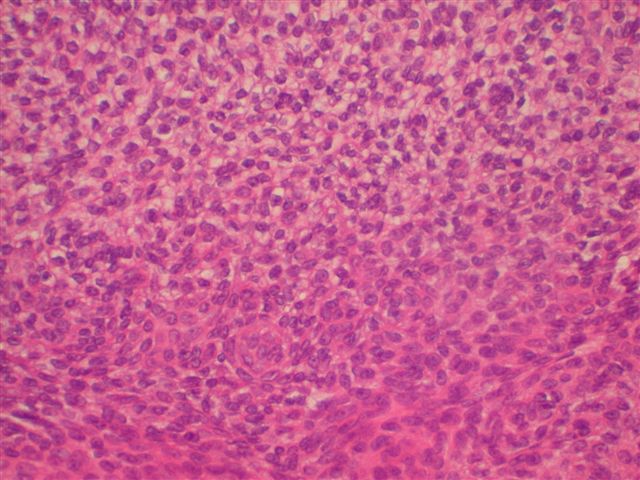
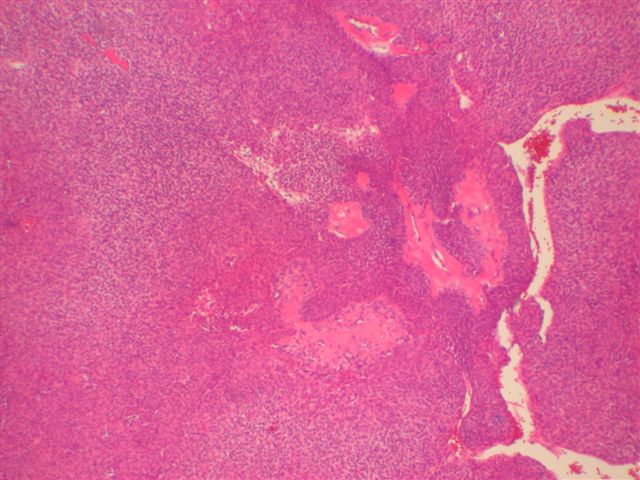
Morphologically, they have a distinctive solid and cystic growth pattern with either true papillae containing fibrovascular cores or pseudopapillae composed of heaped up epithelium. Although not prominent in this case, there are usually fused back to back gland-like structures in solid areas. Cystic areas are formed by central degeneration or necrosis of solid areas or from collection of eosinophilic secretory material. In 18% of cases, only solid areas are present without cystic spaces. There is variable tumor circumscription, mitotic activity, atypia and necrosis. There may be focal clear cell change, squamous differentiation or apocrine type secretion.
These tumors may recur, particularly if the initial excision is inadequate and no reexcision or amputation is performed. They are considered to have a low but significant (14%) metastatic potential. Recommended treatment is reexcision or amputation as necessary to ensure adequate margins.
The differential diagnosis includes other eccrine tumors, including malignant eccrine acrospiroma / hidradenoma, malignant eccrine spiradenoma and papillary eccrine adenoma. Malignant eccrine acrospiroma typically does not occur in the digits or have papillary patterns or back to back glands. Malignant eccrine spiradenoma typically has a 2 cell pattern of central basaloid cells and large peripheral cells and occurs anywhere on the body, not limited to the digits. They also lack papillary patterns and back to back glands. Papillary eccrine adenoma is a well circumscribed tumor with dilated ducts of variable size and a double layer of epithelial cells forming papillae that project into the lumen. It does occur in the digits but almost always has benign behavior.
This particular case was sent to the AFIP, whose diagnosis was consistent with aggressive digital papillary adenocarcinoma. However, other dermatopathologists called it a cystic hidradenoma or an acrospiroma.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Peter Morawiecki, Great Lakes, Illinois, USA.
Website news:
(1) This week's case is sponsored by Invitrogen. Invitrogen offers Zymed total system solution for pathology reagents and automation. From antibodies, kits and probes for IHC and CISH to immunostainers for automation, you can be confident that Zymed products will always deliver high quality staining results and offer the cutting edge pathology solutions you need. Note: sponsors do NOT have access in any manner to email addresses or other personal information in the possession of PathologyOutlines.com.
Visit and follow our Blog to see recent updates to the website.
(1) This week's case is sponsored by Invitrogen. Invitrogen offers Zymed total system solution for pathology reagents and automation. From antibodies, kits and probes for IHC and CISH to immunostainers for automation, you can be confident that Zymed products will always deliver high quality staining results and offer the cutting edge pathology solutions you need. Note: sponsors do NOT have access in any manner to email addresses or other personal information in the possession of PathologyOutlines.com.
Visit and follow our Blog to see recent updates to the website.
Case #15
Clinical history:
A 62 year old Black man had a more than 1 year history of a slowly enlarging thumb mass. Clinically, it was believed to be an epidermal cyst. Xrays failed to show any abnormalities.
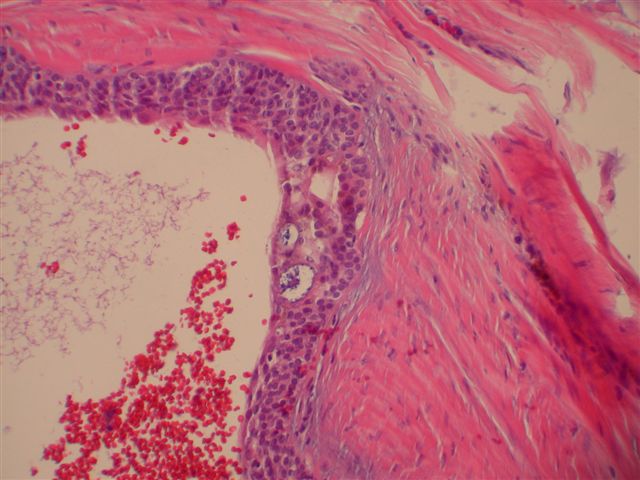
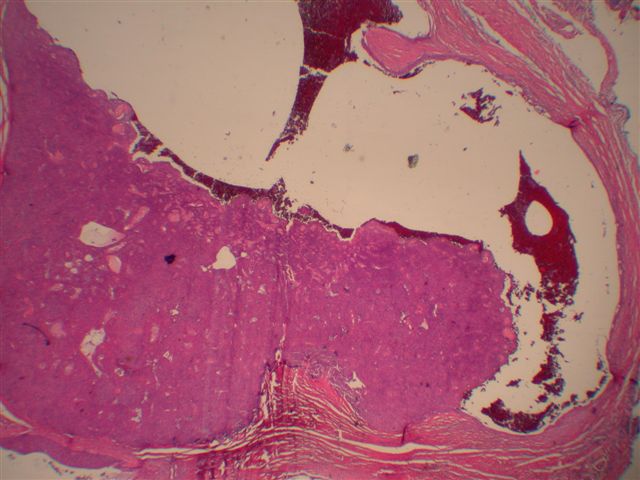
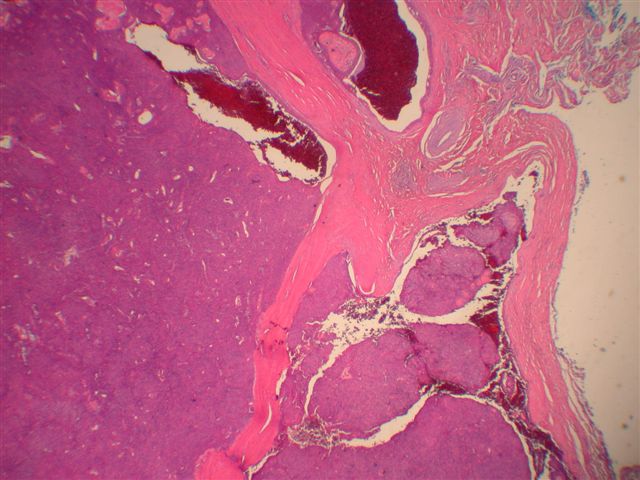
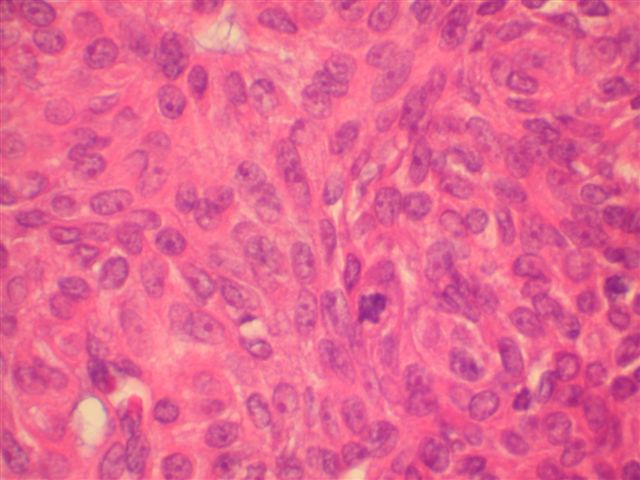
Microscopic images:
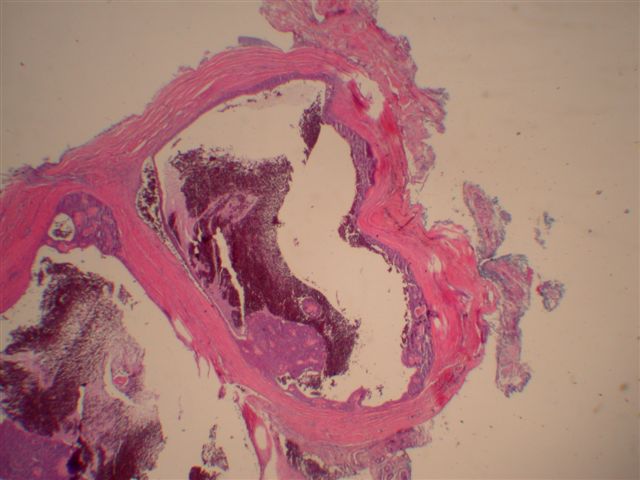
Low power
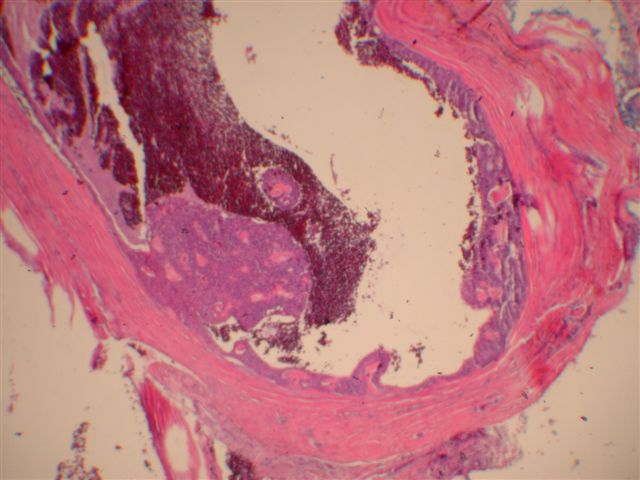
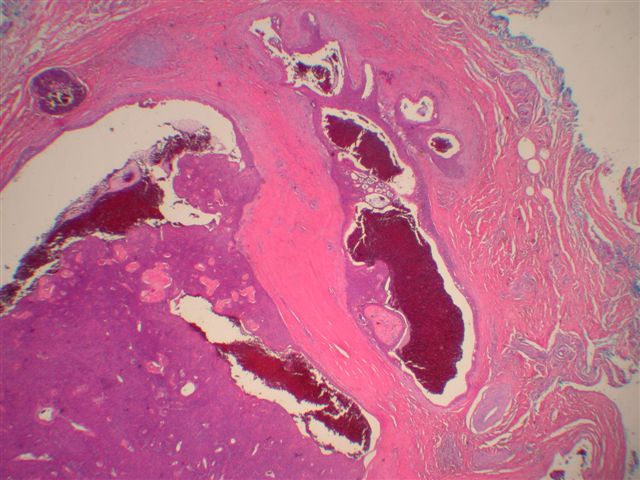
Medium power
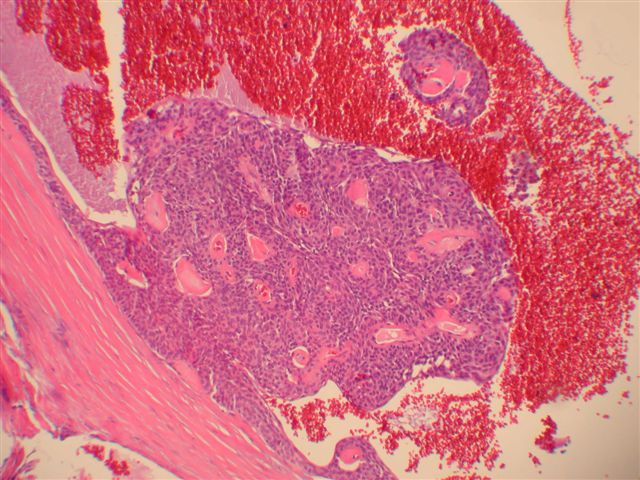
High power
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Aggressive digital papillary adenocarcinoma
Discussion:
Aggressive digital papillary adenocarcinoma is a rare sweat gland tumor that occurs primarily on the digits of the hands and feet and adjacent skin. Although these tumors were initially divided into adenomas and adenocarcinomas, a recent AFIP study concluded that histologic features could not predict which tumors would act aggressively and the authors recommended that all of these tumors be called adenocarcinomas (Am J Surg Pathol 2000;24:775).
These tumors primarily affect males, with a mean age of 52 years (range: 19 - 83 years). Average tumor size is 2 cm (range: 0.4 - 4 cm) and tumors are present for an average of 2 - 3 years before excision. They are usually (85%) on the hand, with the remainder on the feet. They frequently are associated with pain.
Morphologically, they have a distinctive solid and cystic growth pattern with either true papillae containing fibrovascular cores or pseudopapillae composed of heaped up epithelium. Although not prominent in this case, there are usually fused back to back gland-like structures in solid areas. Cystic areas are formed by central degeneration or necrosis of solid areas or from collection of eosinophilic secretory material. In 18% of cases, only solid areas are present without cystic spaces. There is variable tumor circumscription, mitotic activity, atypia and necrosis. There may be focal clear cell change, squamous differentiation or apocrine type secretion.
These tumors may recur, particularly if the initial excision is inadequate and no reexcision or amputation is performed. They are considered to have a low but significant (14%) metastatic potential. Recommended treatment is reexcision or amputation as necessary to ensure adequate margins.
The differential diagnosis includes other eccrine tumors, including malignant eccrine acrospiroma / hidradenoma, malignant eccrine spiradenoma and papillary eccrine adenoma. Malignant eccrine acrospiroma typically does not occur in the digits or have papillary patterns or back to back glands. Malignant eccrine spiradenoma typically has a 2 cell pattern of central basaloid cells and large peripheral cells and occurs anywhere on the body, not limited to the digits. They also lack papillary patterns and back to back glands. Papillary eccrine adenoma is a well circumscribed tumor with dilated ducts of variable size and a double layer of epithelial cells forming papillae that project into the lumen. It does occur in the digits but almost always has benign behavior.
This particular case was sent to the AFIP, whose diagnosis was consistent with aggressive digital papillary adenocarcinoma. However, other dermatopathologists called it a cystic hidradenoma or an acrospiroma.
