
16 September 2005 - Case #20
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Shylashree Chikkamuniyappa Edalur, Hematopathology fellow, University of Texas Health Science Center, San Antonio, Texas, USA.
Case #20
Clinical history:
The patient is a 22 year old, otherwise healthy man with Maffucci syndrome, who presented with pain and swelling of his hands and feet with prominent vascular soft tissue swellings. Radiographs of the hands showed multiple expansile lytic lesions (enchondromas) with focal soft tissue calcifications (figure 1).
Gross description:
The specimen consisted of multiple excisional biopsies of skin measuring from 0.3 to 2.0 cm in diameter. Grossly, they were dark red-brown soft tissue nodules with a white, hard, marble-like cut surface.
Radiology and micro images:

What is your diagnosis?
Diagnosis: Spindle cell hemangioma
Discussion:
Maffucci syndrome is a rare, nonhereditary, congenital disorder of multiple enchondromas and soft tissue hemangiomas (Medscape: Maffucci Syndrome [Accessed 20 October 2023]). There is no racial or sexual predilection. Pathological fractures are common and 20% develop malignant tumors, usually chondrosarcomas and rarely angiosarcomas. The soft tissue hemangiomas usually occur in young adults and affect the distal extremities, especially the hands. They may be cavernous, capillary, phlebectatic (dilated veins) or spindle cell hemangiomas and occur in various parts of the body.
Spindle cell hemangiomas, originally described in 1986 as spindle cell hemangioendotheliomas, are uncommon lesions that commonly occur in children or young adults, although they can occur at all ages (Am J Surg Pathol 1986;10:521). They initially form solitary nodules and later multiple nodules within the distal extremities, often the subcutis of the hand. They produce few symptoms, causing delay in treatment.
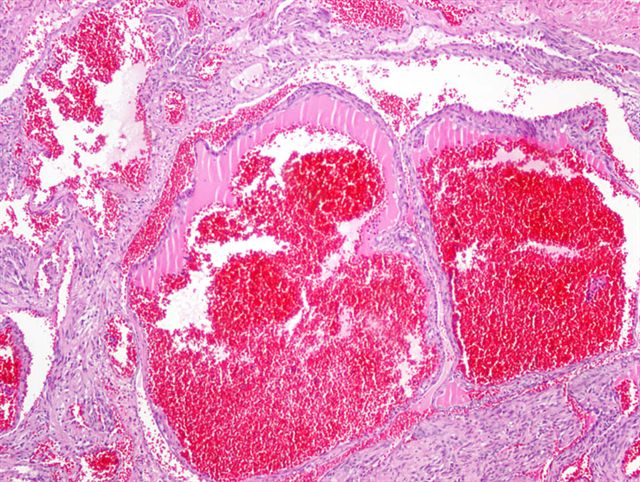
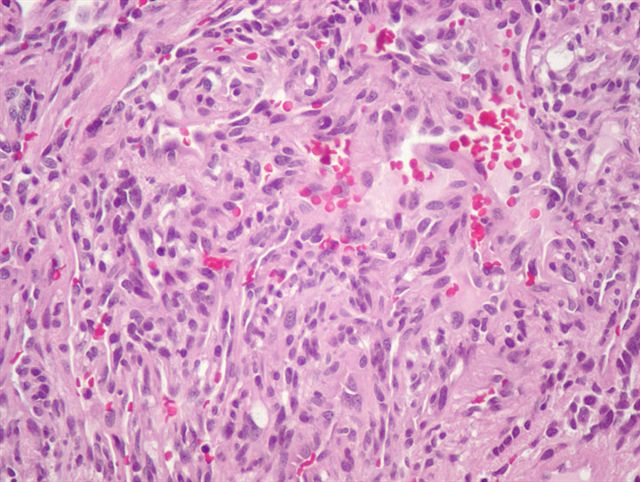
Grossly, spindle cell hemangiomas are usually firm nodules. Microscopically, they are often partly or completely intravascular and resemble both a cavernous hemangioma and Kaposi sarcoma. They are composed of thin walled cavernous blood vessels lined by flattened endothelial cells containing red blood cells and thrombi. The thrombi may develop into calcified phleboliths. The area between vessels contains bland, spindled, kaposiform-like areas, composed of collapsed vessels, pericytes and fibroblastic cells. The spindled areas may contain distinctive round or epithelioid cells containing vacuoles and intracytoplasmic lumens, suggestive of epithelioid hemangioendothelioma. There is no / minimal atypia and low / no mitotic activity. The spindle cells are immunoreactive for vimentin and actin but are negative for CD34.
Spindle cell hemangiomas are benign lesions with no metastatic potential, although 60% recur. They are believed to be vascular malformations in which variation of blood flow causes alternating areas of vascular expansion and collapse (Am J Surg Pathol 1996;20:1196). Recurrences may represent contiguous spread along or multifocal involvement of a vessel.
The differential diagnosis includes cavernous hemangioma and Kaposi sarcoma. Cavernous hemangiomas lack the spindle cell component of spindle cell hemangioma. Kaposi sarcoma has honeycomb-like vascular spaces with interweaving, elongated spindle cells that are strongly CD34+ and rarely contains dilated cavernous vessels or epithelioid endothelial cells (Arch Pathol Lab Med 2005;129:1187). The differential diagnosis may also include epithelioid hemangioendothelioma, due to the intracytoplasmic lumina.
References: Spitz: Genodermatoses - A Full-Color Clinical Guide to Genetic Skin Disorders, 1st Edition, 1996, Weiss: Enzinger and Weiss's Soft Tissue Tumors, 4th Edition, 2001
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Shylashree Chikkamuniyappa Edalur, Hematopathology fellow, University of Texas Health Science Center, San Antonio, Texas, USA.
Website news:
(1) This week's case is sponsored by Invitrogen. Invitrogen offers Zymed total system solution for pathology reagents and automation. From antibodies, kits and probes for IHC and CISH to immunostainers for automation, you can be confident that Zymed products will always deliver high quality staining results and offer the cutting edge pathology solutions you need. (Note: sponsors do NOT have access to email addresses or other personal information in the possession of PathologyOutlines.com.)
Visit and follow our Blog to see recent updates to the website.
(1) This week's case is sponsored by Invitrogen. Invitrogen offers Zymed total system solution for pathology reagents and automation. From antibodies, kits and probes for IHC and CISH to immunostainers for automation, you can be confident that Zymed products will always deliver high quality staining results and offer the cutting edge pathology solutions you need. (Note: sponsors do NOT have access to email addresses or other personal information in the possession of PathologyOutlines.com.)
Visit and follow our Blog to see recent updates to the website.
Case #20
Clinical history:
The patient is a 22 year old, otherwise healthy man with Maffucci syndrome, who presented with pain and swelling of his hands and feet with prominent vascular soft tissue swellings. Radiographs of the hands showed multiple expansile lytic lesions (enchondromas) with focal soft tissue calcifications (figure 1).
Gross description:
The specimen consisted of multiple excisional biopsies of skin measuring from 0.3 to 2.0 cm in diameter. Grossly, they were dark red-brown soft tissue nodules with a white, hard, marble-like cut surface.
Radiology and micro images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Spindle cell hemangioma
Discussion:
Maffucci syndrome is a rare, nonhereditary, congenital disorder of multiple enchondromas and soft tissue hemangiomas (Medscape: Maffucci Syndrome [Accessed 20 October 2023]). There is no racial or sexual predilection. Pathological fractures are common and 20% develop malignant tumors, usually chondrosarcomas and rarely angiosarcomas. The soft tissue hemangiomas usually occur in young adults and affect the distal extremities, especially the hands. They may be cavernous, capillary, phlebectatic (dilated veins) or spindle cell hemangiomas and occur in various parts of the body.
Spindle cell hemangiomas, originally described in 1986 as spindle cell hemangioendotheliomas, are uncommon lesions that commonly occur in children or young adults, although they can occur at all ages (Am J Surg Pathol 1986;10:521). They initially form solitary nodules and later multiple nodules within the distal extremities, often the subcutis of the hand. They produce few symptoms, causing delay in treatment.
Grossly, spindle cell hemangiomas are usually firm nodules. Microscopically, they are often partly or completely intravascular and resemble both a cavernous hemangioma and Kaposi sarcoma. They are composed of thin walled cavernous blood vessels lined by flattened endothelial cells containing red blood cells and thrombi. The thrombi may develop into calcified phleboliths. The area between vessels contains bland, spindled, kaposiform-like areas, composed of collapsed vessels, pericytes and fibroblastic cells. The spindled areas may contain distinctive round or epithelioid cells containing vacuoles and intracytoplasmic lumens, suggestive of epithelioid hemangioendothelioma. There is no / minimal atypia and low / no mitotic activity. The spindle cells are immunoreactive for vimentin and actin but are negative for CD34.
Spindle cell hemangiomas are benign lesions with no metastatic potential, although 60% recur. They are believed to be vascular malformations in which variation of blood flow causes alternating areas of vascular expansion and collapse (Am J Surg Pathol 1996;20:1196). Recurrences may represent contiguous spread along or multifocal involvement of a vessel.
The differential diagnosis includes cavernous hemangioma and Kaposi sarcoma. Cavernous hemangiomas lack the spindle cell component of spindle cell hemangioma. Kaposi sarcoma has honeycomb-like vascular spaces with interweaving, elongated spindle cells that are strongly CD34+ and rarely contains dilated cavernous vessels or epithelioid endothelial cells (Arch Pathol Lab Med 2005;129:1187). The differential diagnosis may also include epithelioid hemangioendothelioma, due to the intracytoplasmic lumina.
References: Spitz: Genodermatoses - A Full-Color Clinical Guide to Genetic Skin Disorders, 1st Edition, 1996, Weiss: Enzinger and Weiss's Soft Tissue Tumors, 4th Edition, 2001
