
Anus & perianal area
Other nonneoplastic
Tailgut cyst
Editorial Board Member: Naziheh Assarzadegan, M.D.
Deputy Editor-in-Chief: Aaron R. Huber, D.O.


Last author update: 31 July 2023
Last staff update: 31 July 2023
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Tailgut cyst

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Diagrams / tables | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Paulsen JD, Polydorides AD. Tailgut cyst. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/anustailgutcyst.html. Accessed May 13th, 2024.
Definition / general
- Cystic developmental anomaly of the retrorectal / presacral space that is thought to arise from remnants of the embryonic tailgut
Essential features
- Congenital, well demarcated, usually multiloculated, cystic lesion of the retrorectal / presacral space that is thought to arise from remnants of the embryonic tailgut
- Preoperative diagnosis relies on imaging, as fine needle biopsy is not recommended due to risk of infection or seeding of tumor cells
- Multiple types of epithelial linings have been described; stratified squamous epithelium is most common (~75%)
- Cyst wall shows disorganized / irregular smooth muscle bundles without neural plexi
- Prognosis depends upon presence or absence of malignant transformation, which can be seen in up to ~25% of cases (usually as either adenocarcinoma or well differentiated neuroendocrine tumor)
Terminology
- Retrorectal / perianal cystic hamartoma (misnomer, as there is no good evidence that this lesion is hamartomatous) (Histopathology 2023;82:232)
- Retrorectal space cyst
- Cyst of postanal intestine
- Myoepithelial hamartoma of rectum (Dis Colon Rectum 1961;4:409)
ICD coding
- ICD-10: K62.89 - other specified diseases of anus and rectum
Epidemiology
- Rare; incidence is estimated at 1 per 40,000 hospital admissions based on Mayo Clinic data (Dis Colon Rectum 1985;28:644)
- Can occur at any age
- Most commonly develops in the fifth decade of life (Ann Coloproctol 2019;35:268)
- Uncommon in children
- Female predominance (F:M = 3 - 9:1) (Ann Coloproctol 2019;35:268)
Sites
- Retrorectal / presacral space
- Retrorectal / presacral space is a potential space defined by the following boundaries (AJR Am J Roentgenol 2017;209:790)
- Anterior: rectum
- Superior: pelvic peritoneal reflection
- Inferior: levator ani muscles
- Posterior: presacral fascia, sacrum and coccyx
- Lateral: iliac vessels and ureters
Pathophysiology
- Considered a developmental anomaly
- Precise embryological origin is uncertain but likely is a remnant of the distal hindgut that extends into the vestigial / embryonic tail (Histopathology 2023;82:232)
- Involution of the embryonic tailgut occurs by the eighth week of gestation; failure of regression is thought to give rise to tailgut cyst (Arch Pathol Lab Med 2000;124:725)
Diagrams / tables
Images hosted on other servers:

Retrorectal space
Clinical features
- Clinical presentation
- ~50% asymptomatic
- Symptoms are usually nonspecific and due to local mass effect
- Constipation, decreased stool caliber, rectal pain, rectal fullness, obstruction, tenesmus, rectal bleeding (usually painless), discomfort while sitting, dysuria, urinary retention, lower limb neurological symptoms due to sacral plexus compression (Ann Coloproctol 2019;35:268)
- Rarely presents as prolapsing cyst through the anus (Eur J Pediatr Surg 2013;23:e3)
- Physical exam findings
- Palpable mass (usually nontender) on digital rectal exam
- Funnel shaped dimple in the postanal midline (European J Pediatr Surg Rep 2013;1:51)
- Fissures and fistulas, often recurrent
- Secondary infection may lead to sepsis or abscess formation
Diagnosis
- Pelvic magnetic resonance imaging (MRI)
- Ultrasound guided needle biopsy is not recommended due to risk of infection or seeding of tumor cells (Int J Colorectal Dis 2007;22:1283)
Radiology description
- Ultrasound
- Cystic lesion with internal echoes from inflammatory debris or mucus
- Computed tomography (CT)
- Well defined cystic mass in retrorectal space
- Water or soft tissue density
- Loss of well defined margins and bone destruction may be seen with malignant transformation
- Pelvic MRI (Ann Coloproctol 2019;35:268)
- Well defined cystic mass in retrorectal space
- Hypointense T1 weighted
- Hyperintense on T2 weighted
- Loss of well defined margins and bone destruction may be seen with malignant transformation
- Well defined cystic mass in retrorectal space
Radiology images
Images hosted on other servers:

Retrorectal cystic mass

Malignant transformation
Prognostic factors
- Prognosis depends upon presence or absence of malignant transformation
- Excision is curative in cases without malignant transformation
- Overall metastatic potential of cases with malignant transformation is unclear, although distant metastasis has been reported (Medicine (Baltimore) 2020;99:e20941, Clin Case Rep 2023;11:e6893)
Case reports
- 50 year old woman with defecation difficulty (Medicine (Baltimore) 2020;99:e20941)
- 54 year old woman with pelvic and perineal pain (Autops Case Rep 2019;10:e2019115)
- 57 year old man with thin stool and lower pelvic heaviness (Ann Coloproctol 2020;36:54)
Treatment
- Complete surgical resection with adequate margins
- Confirmation of diagnosis
- Symptom relief
- Prevention of malignant transformation
- Surgical approach may be anterior (transabdominal with laparoscopy), posterior (paracoccygeal) or combined, depending on tumor size and position (Ann Coloproctol 2019;35:268)
- Adjuvant chemotherapy and radiotherapy in cases with carcinoma transformation
Clinical images
Images hosted on other servers:

Posterior approach view
Gross description
- Well circumscribed cystic mass
- Usually multiloculated (~80%) (Am J Clin Pathol 1988;89:139)
- Variable solid areas
- Cysts may contain clear serous fluid, green fluid, amorphous debris, mucinous material or mud-like (opaque brown pasty) contents
- Size
- Range: 1 - 22 cm (Diagn Cytopathol 2000;22:376)
- Average: 3.9 cm (Am J Clin Pathol 1988;89:139)
Gross images
Images hosted on other servers:

Intact resection

Mud-like contents

Tailgut cyst adenocarcinoma
Microscopic (histologic) description
- Multiple types of cyst lining have been described
- Stratified squamous epithelium (most common, ~75%), likely representing a metaplastic response to inflammation (Am J Clin Pathol 1988;89:139)
- Keratinizing or nonkeratinizing
- Columnar epithelium
- Pseudostratified, stratified, goblet cell containing, ciliated
- Transitional epithelium
- Mucinous epithelium
- Cuboidal epithelium
- Stratified squamous epithelium (most common, ~75%), likely representing a metaplastic response to inflammation (Am J Clin Pathol 1988;89:139)
- More than 1 type of epithelial lining may be seen within a single cyst
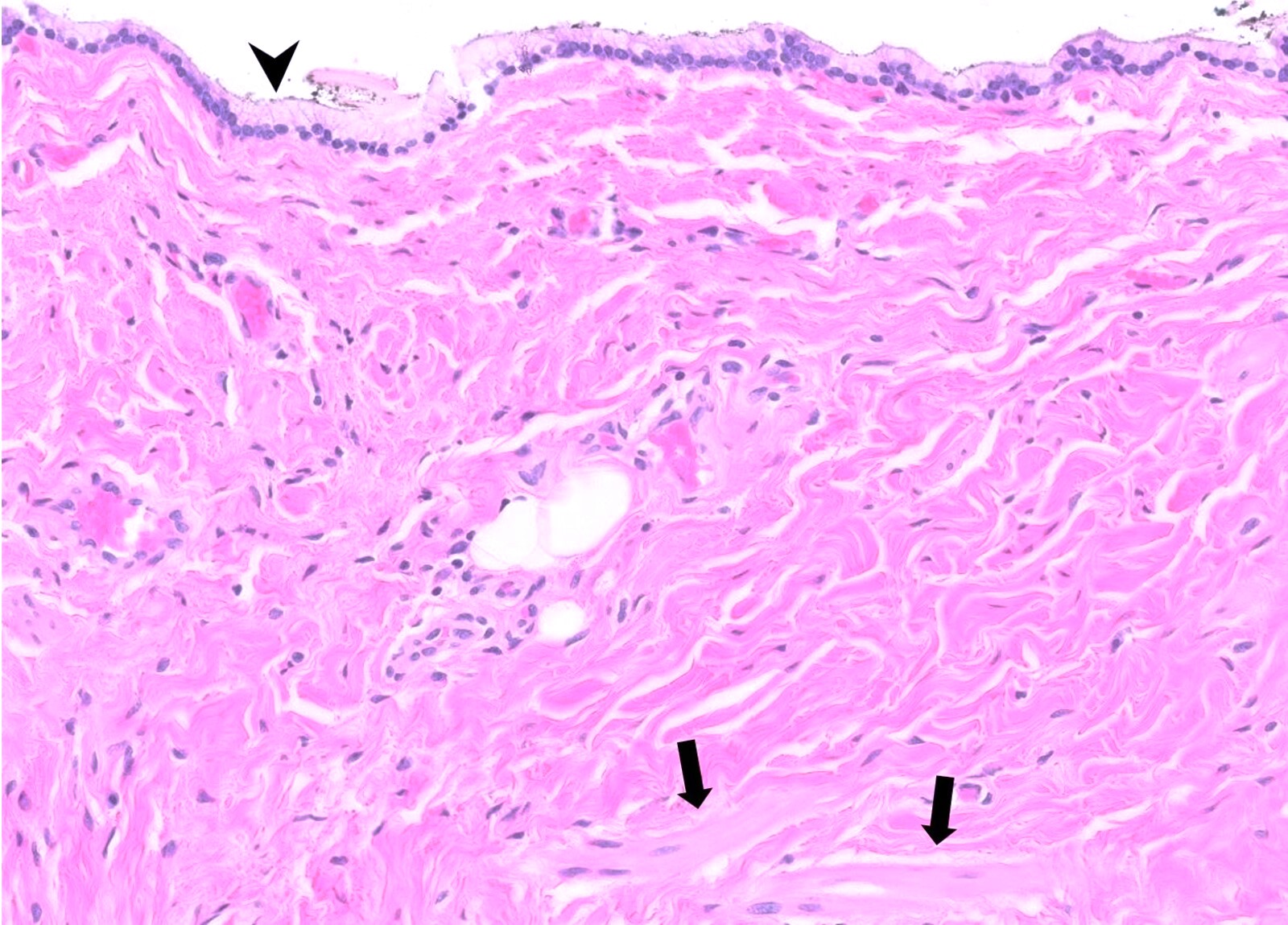
- Surrounding dense fibroconnective tissue stroma with disorganized / irregular smooth muscle bundles that lack neural plexi
- Histologic evidence of rupture may be seen
- Acute and chronic inflammation
- Xanthogranulomatous reaction
- Neoplastic transformation in ~25% of cases as per comprehensive 2019 meta analysis (Colorectal Dis 2019;21:869)
- Adenocarcinoma (most common, ~43%)
- Well differentiated neuroendocrine tumors (~39%)
- Limited to case reports: squamous cell carcinoma, adenosquamous carcinoma, transitional cell carcinoma and sarcoma (An Bras Dermatol 2018;93:733, J Surg Case Rep 2015;2015:rjv085)
Microscopic (histologic) images
Contributed by John D. Paulsen, M.D. and Alexandros D. Polydorides, M.D., Ph.D.
Dense fibroconnective tissue stroma
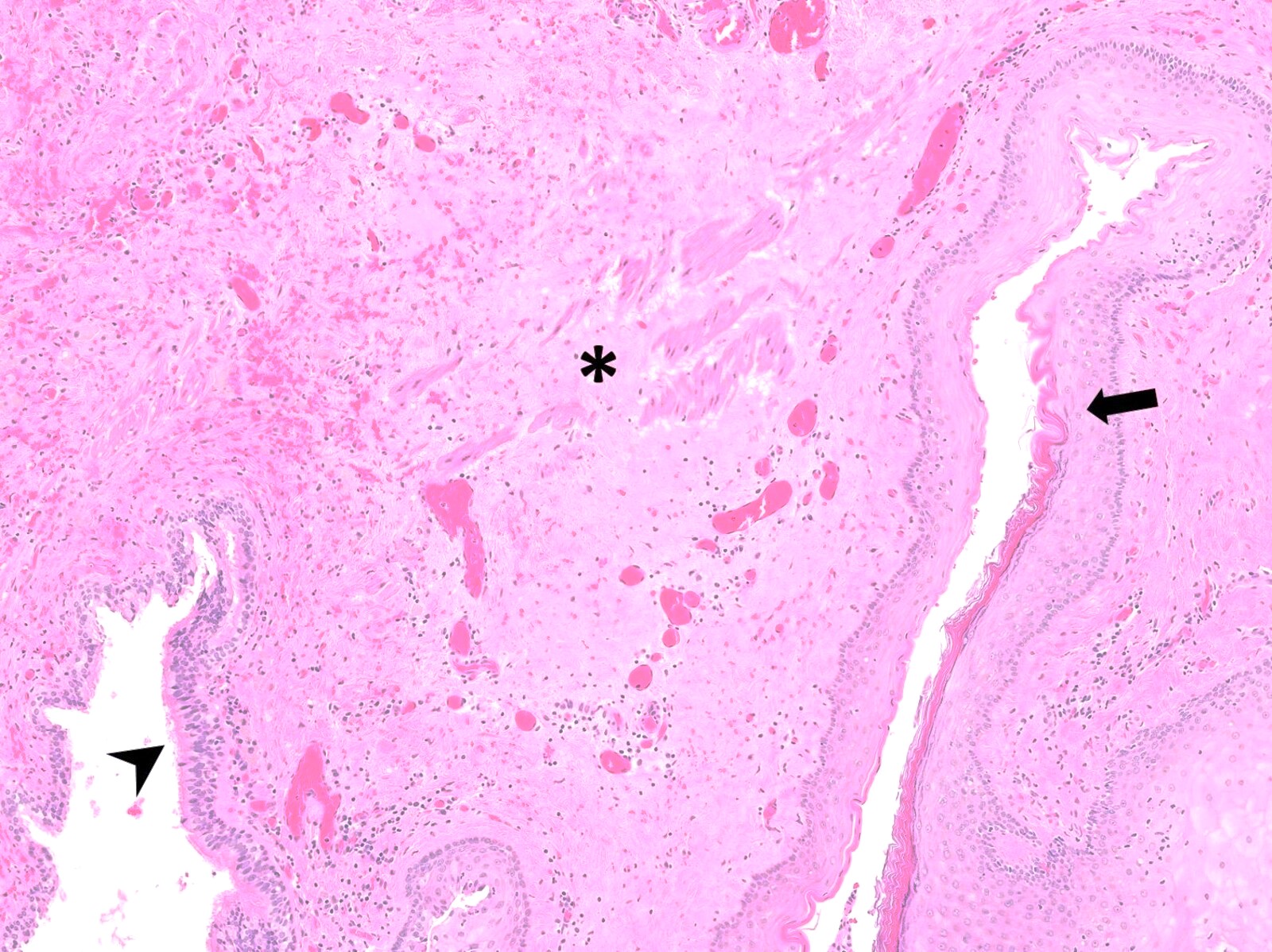
Disorganized smooth muscle
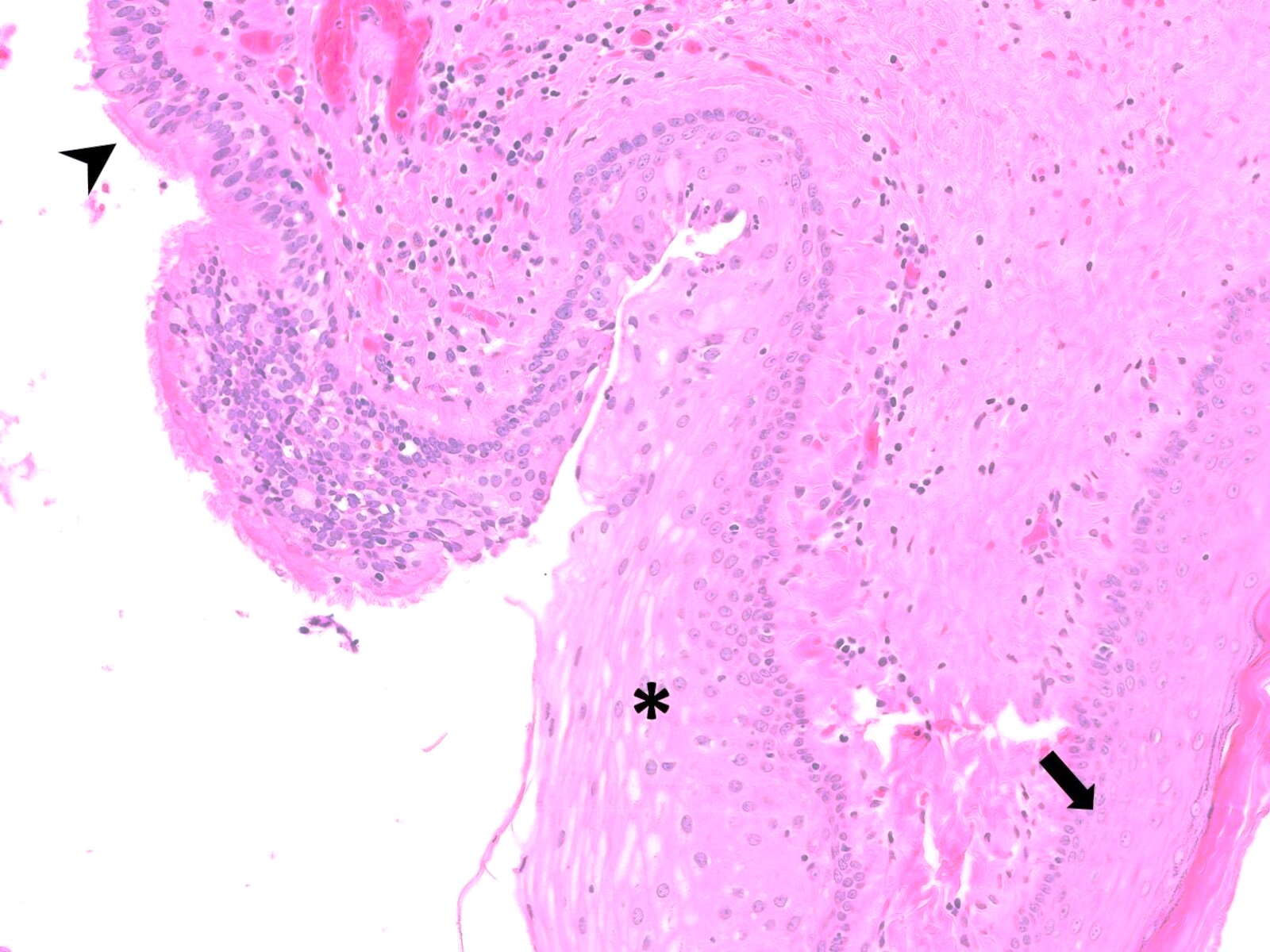
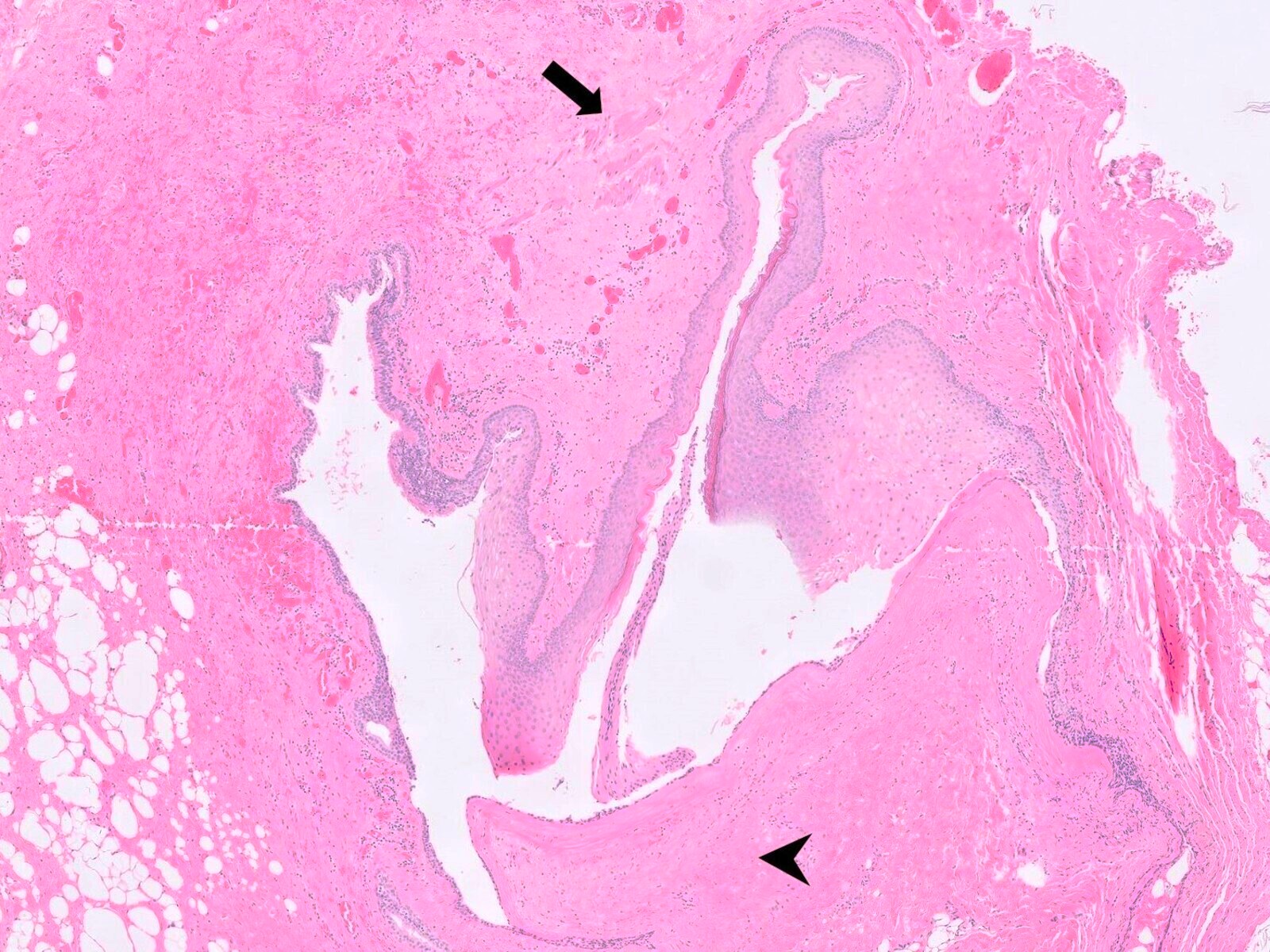
Epithelial linings
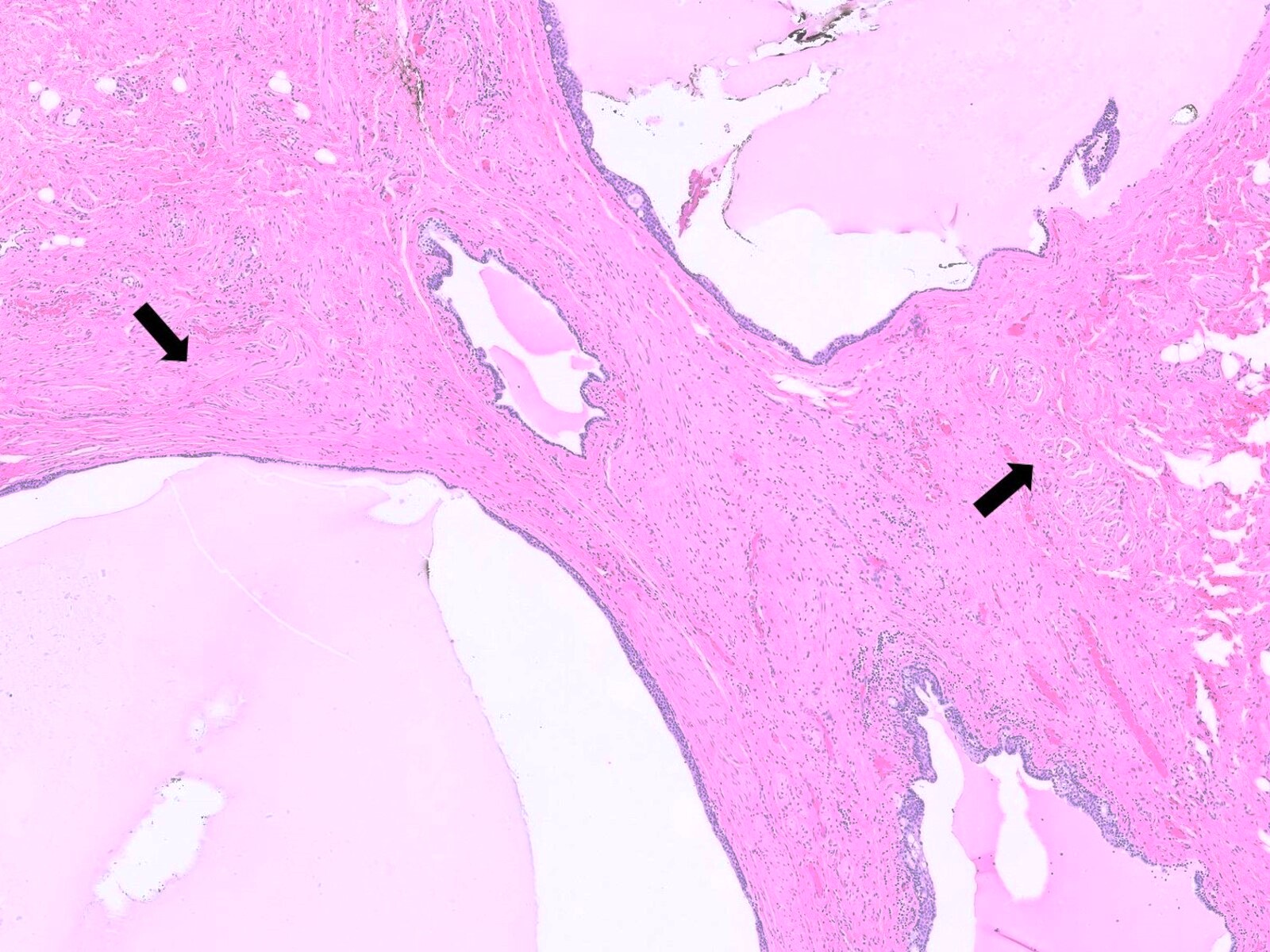
Multiple loculations
Mucinous columnar epithelium
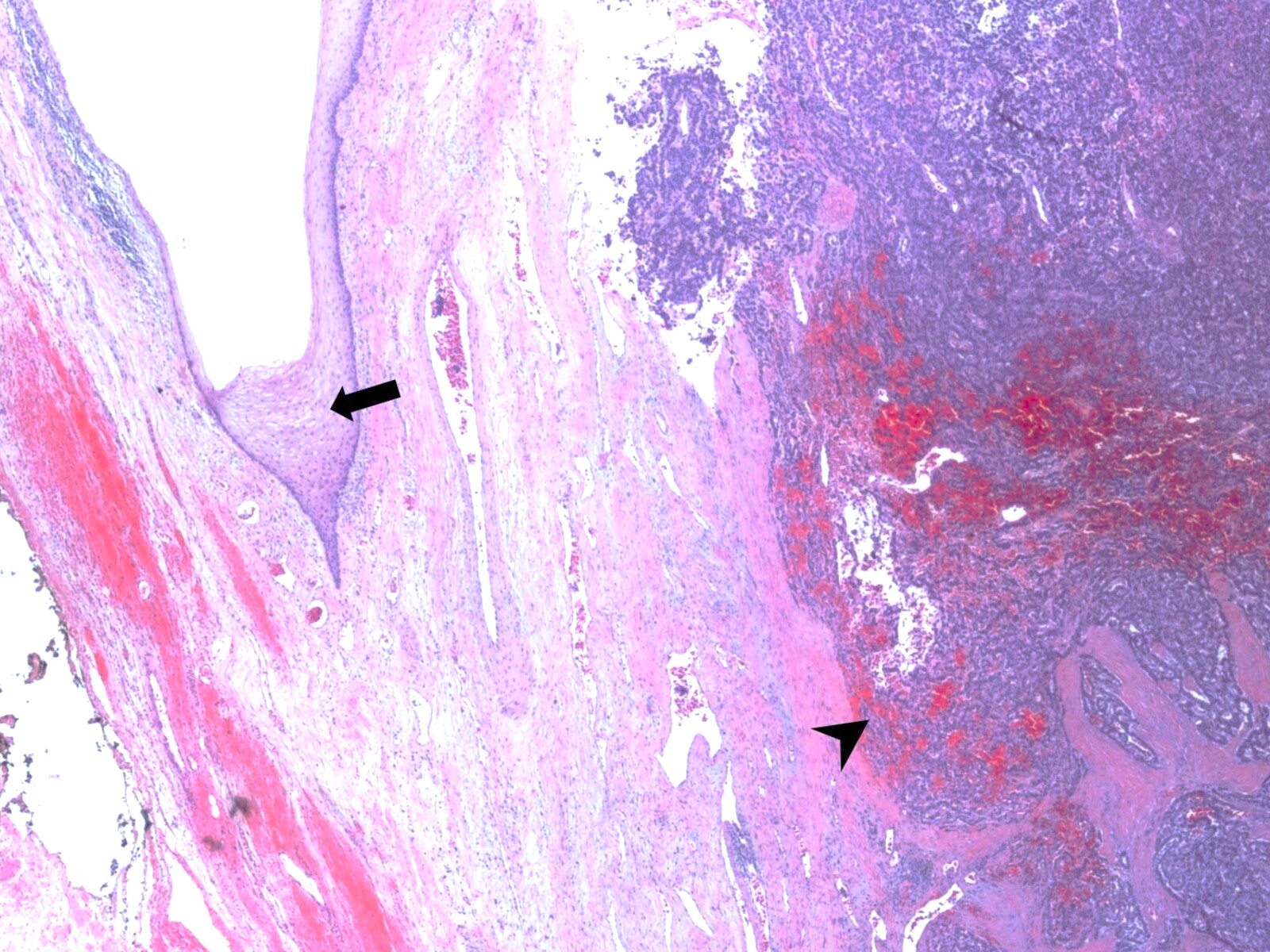
Neoplastic transformation, neuroendocrine tumor
Sample pathology report
- Retrorectal space, excision:
- Tailgut cyst (see comment)
- Comment: Sections show a benign cyst lined by stratified squamous, transitional and ciliated columnar epithelium. Disorganized bundles of smooth muscle are present in the cyst wall, without neural plexi. The findings are consistent with a diagnosis of tailgut cyst (synonym: retrorectal cystic hamartoma). There is focal epithelial disruption with associated xanthogranulomatous inflammation, suggestive of rupture.
Differential diagnosis
- Rectal duplication cyst:
- Lined by rectal mucosa with crypts
- May show heterotopic elements (e.g., gastric, bronchial)
- Cyst lumen contains mucin
- Well developed smooth muscle layer resembling muscularis propria (2 layers, often with nerve plexi)
- Shows continuity with rectum, grossly or microscopically
- Usually unilocular
- Lined by rectal mucosa with crypts
- Epidermoid cyst:
- Lined by keratinizing squamous epithelium
- Cyst lumen contains keratinous debris
- No associated smooth muscle or adnexal structures within cyst wall
- Usually unilocular
- Dermoid cyst:
- Lined by keratinizing squamous epithelium
- Cyst wall shows associated skin adnexal structures (hair follicles, sebaceous glands, sweat glands)
- Cyst lumen contains keratinous debris and oily material
- No associated smooth muscle within cyst wall
- Usually unilocular
- Neurenteric cyst:
- Lined by columnar or cuboidal cells with or without cilia
- Diagnosis is established by presence of glial tissue or connection to spinal cord
- Anterior sacral meningocele:
- Lined by attenuated arachnoid cells
- Communicates with subarachnoid space
- Usually unilocular
- Radiographic scimitar sign is pathognomonic (Dis Colon Rectum 1988;31:806)
- Anal gland cyst:
- Communicates with anal duct or crypt
- Located near anal sphincter
- Cyst lumen contains mucin
- Sacrococcygeal teratoma:
- Contains derivatives of 2 or more germ layers (ectoderm, mesoderm, endoderm)
- Mature tissue elements, immature tissue elements or both may be seen
- Usually solid but cystic areas may develop (Dis Colon Rectum 1988;31:806)
- Most present in infancy or childhood
- Sacrococcygeal chordoma:
Board review style question #1
A 54 year old woman presented with rectal fullness and was found to have a cystic tumor in the retrorectal space on pelvic magnetic resonance imaging (MRI). The lesion was surgically resected and is shown above. Which of the following, if found on histologic examination, would be most suggestive of a tailgut cyst?
- Cyst lining comprised of attenuated arachnoid cells
- Cyst lining of rectal mucosa with associated well developed smooth muscle layer within the cyst wall
- Fibroconnective tissue containing disorganized smooth muscle bundles within the cyst wall
- Keratinizing stratified squamous epithelial lining with associated skin adnexal structures
- Physaliphorous cells showing immunoreactivity for brachyury
Board review style answer #1
C. Fibroconnective tissue cyst wall containing disorganized smooth muscle bundles is characteristic of tailgut cysts. Answer B is incorrect because an associated well developed smooth muscle layer that is muscularis propria-like and often with nerve plexi is seen in rectal duplication cysts. Answer A is incorrect because a cyst lining comprised of attenuated arachnoid cells is featured in anterior sacral meningoceles. Answer D is incorrect because keratinizing stratified squamous epithelial lining with associated skin adnexal structures is seen in dermoid cysts. Answer E is incorrect because physaliphorous cells showing immunoreactivity for brachyury is found in cystic sacrococcygeal chordomas.
Comment Here
Reference: Tailgut cyst
Comment Here
Reference: Tailgut cyst
Board review style question #2
A 59 year old woman presented with constipation and was found to have a cystic tumor in the presacral space. The lesion was surgically resected and submitted for histopathological evaluation. A diagnosis of tailgut cyst was rendered. Which of the following is true regarding the diagnosis?
- Fine needle biopsy is recommended prior to surgical excision
- Prognosis depends upon the presence or absence of malignant transformation
- Squamous cell carcinoma is invariably present on microscopic examination when the lesion is completely submitted for histopathological evaluation
- Tends to be unilocular
- The cyst wall usually contains a well developed smooth muscle layer with nerve plexi
Board review style answer #2
B. The prognosis of tailgut cysts depends upon the presence or absence of malignant transformation. It is reported that up to ~25% of tailgut cysts show malignant transformation, most commonly as adenocarcinoma or well differentiated neuroendocrine tumors, although squamous cell carcinoma, adenosquamous carcinoma, transitional cell carcinoma and sarcoma have also been reported. Answer A is incorrect because fine needle biopsy is not recommended prior to surgical excision due to risk of infection or seeding of tumor cells. Answer C is incorrect because squamous cell carcinoma arising in association with tailgut cyst is extremely rare and limited to case reports. Answer D is incorrect because tailgut cysts are typically multilocular (~80%). Answer E is incorrect because tailgut cysts show disorganized / irregular smooth muscle bundles without nerve plexi within the cyst wall, as opposed to rectal duplication cysts, which show a well developed smooth muscle layer (muscularis propria-like) with nerve plexi.
Comment Here
Reference: Tailgut cyst
Comment Here
Reference: Tailgut cyst
