Colon
Drug induced colitides
Mycophenolate mofetil associated colitis
Author: Catherine E. Hagen, M.D.
Deputy Editor-in-Chief: Raul S. Gonzalez, M.D.

Last author update: 12 May 2020
Last staff update: 17 September 2021
Copyright: 2020-2025, PathologyOutlines.com, Inc.
PubMed Search: Mycophenolate mofetil[TI] colitis

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Negative stains | Sample pathology report | Differential diagnosis | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Hagen CE. Mycophenolate mofetil associated colitis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/colonmmfcolitis.html. Accessed September 22nd, 2025.
Definition / general
- Gastrointestinal tract toxicity related to mycophenolate therapy
- Mycophenolate mofetil (CellCept) is a therapeutic immunosuppressant agent that inhibits the proliferation of B and T cells through noncompetitive, reversible inhibition of inosine monophosphate dehydrogenase and is used for (Pharmacotherapy 1997;17:1178):
- Prevention of acute rejection of solid organ transplants
- Treatment of various inflammatory and autoimmune disorders
- Prophylaxis of acute graft versus host disease (GVHD) and treatment of chronic graft versus host disease
Essential features
- Gastrointestinal tract toxicity commonly seen in transplant patients taking mycophenolate, particularly renal transplant recipients
- Symptoms resolve with medication withdrawal or dose reduction
- Histologically characterized by crypt apoptosis, crypt injury, lamina propria eosinophils and architectural distortion
- Lack of neuroendocrine cell aggregates, presence of eosinophils and paucity of apoptotic microabscesses can help distinguish from graft versus host disease
Terminology
- Also called CellCept colitis
ICD coding
- ICD-10: Z79.899 - other long term (current) drug therapy
Epidemiology
- Mean age about 35 - 50 (World J Gastrointest Endosc 2017;9:405, Clin Transplant 2014;28:1244)
- M:F = 1:1
- More common among solid organ transplant patients, especially kidney transplant recipients (World J Gastrointest Endosc 2017;9:405, Ann Gastroenterol 2015;28:366)
- Reported incidence among patients taking mycophenolate is approximately 30% (Clin Transplant 2014;28:1244)
Sites
- Anywhere in gastrointestinal tract can be involved:
- Colon > upper gastrointestinal tract
- Right colon > left colon / rectum (Ann Gastroenterol 2015;28:366)
Pathophysiology
- Not well understood
- Possible mechanisms include direct toxic effect of drug, antimetabolite effect on enterocytes leading to reduced crypt proliferation or immune dysregulation (Histopathology 2013;63:649, Am J Surg Pathol 2008;32:1367)
Etiology
- Some correlation with mycophenolate dosage (Transplantation 1998;65:1450)
Clinical features
- Watery diarrhea, nausea, vomiting
- Severe cases can result in malabsorption and weight loss
- Onset varies widely from within 6 months of starting mycophenolate to > 10 years (Case Rep Gastrointest Med 2016;2016:3058407)
- Endoscopically characterized by ulceration, erythema, hyperemia and coarse appearing mucosa but endoscopic appearance may also be normal (World J Gastrointest Endosc 2017;9:405, Ann Gastroenterol 2015;28:366)
Diagnosis
- Endoscopy with tissue biopsy
- Symptom resolution following drug withdrawal / dose reduction
- Exclusion of other etiologies (e.g. infection, other drugs, etc.)
Prognostic factors
- Patients universally do well following withdrawal or dose reduction
Case reports
- 31 year old woman with mycophenolate induced colitis after 10 years of use (Case Rep Gastrointest Med 2016;2016:3058407)
- 33 year old man with late onset mycophenolate mofetil related colitis (Am J Health Syst Pharm 2014;71:1858)
- 44 year old woman with systemic sclerosis and mycophenolate mofetil induced colitis (BMJ Case Rep 2018;2018:bcr-2018-224829)
- 55 year old man, a heart transplant recipient, with mycophenolate mofetil induced colitis (BMJ Case Rep 2018;2018:bcr-2017-224035)
- 64 year old man with mycophenolate mofetil induced colitis mimicking ischemic colitis (Case Rep Gastroenterol 2014;8:95)
Treatment
- Dose reduction or discontinuation of mycophenolate
Clinical images
Images hosted on other servers:


Endoscopic appearance
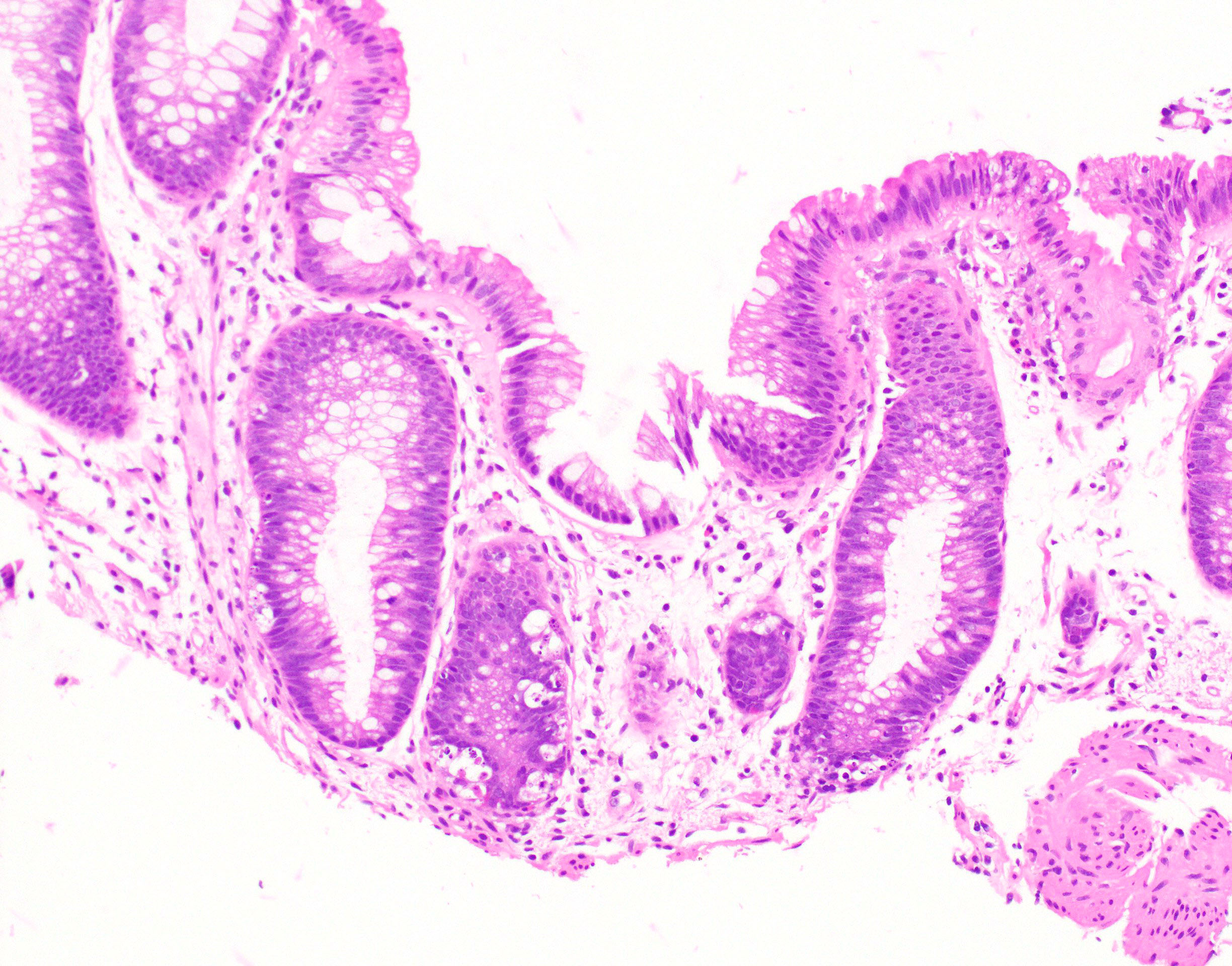
Microscopic (histologic) description
- Crypt apoptosis with no or few apoptotic microabscesses
- Increased eosinophils (> 15/10 high powered fields) present in lamina propria
- Neutrophilic inflammation may also be present in lamina propria; cryptitis and crypt abscess may be present but usually focal (J Clin Pathol 2013;66:8)
- Lack of lamina propria endocrine cell aggregates
- Architectural distortion
- Pseudopyloric gland metaplasia can be seen (Int J Surg Pathol 2003;11:295)
- Injured dilated eosinophilic crypts may be present but typically to a lesser degree than graft versus host disease
- Can have Crohn's-like appearance with patchy inflammation and lymphoid hyperplasia (Int J Surg Pathol 2003;11:295)
- Cases are not routinely graded but if necessary the Lerner system can be used (Am J Surg Pathol 2013;37:1319)
Microscopic (histologic) images
Contributed by Catherine E. Hagen, M.D.
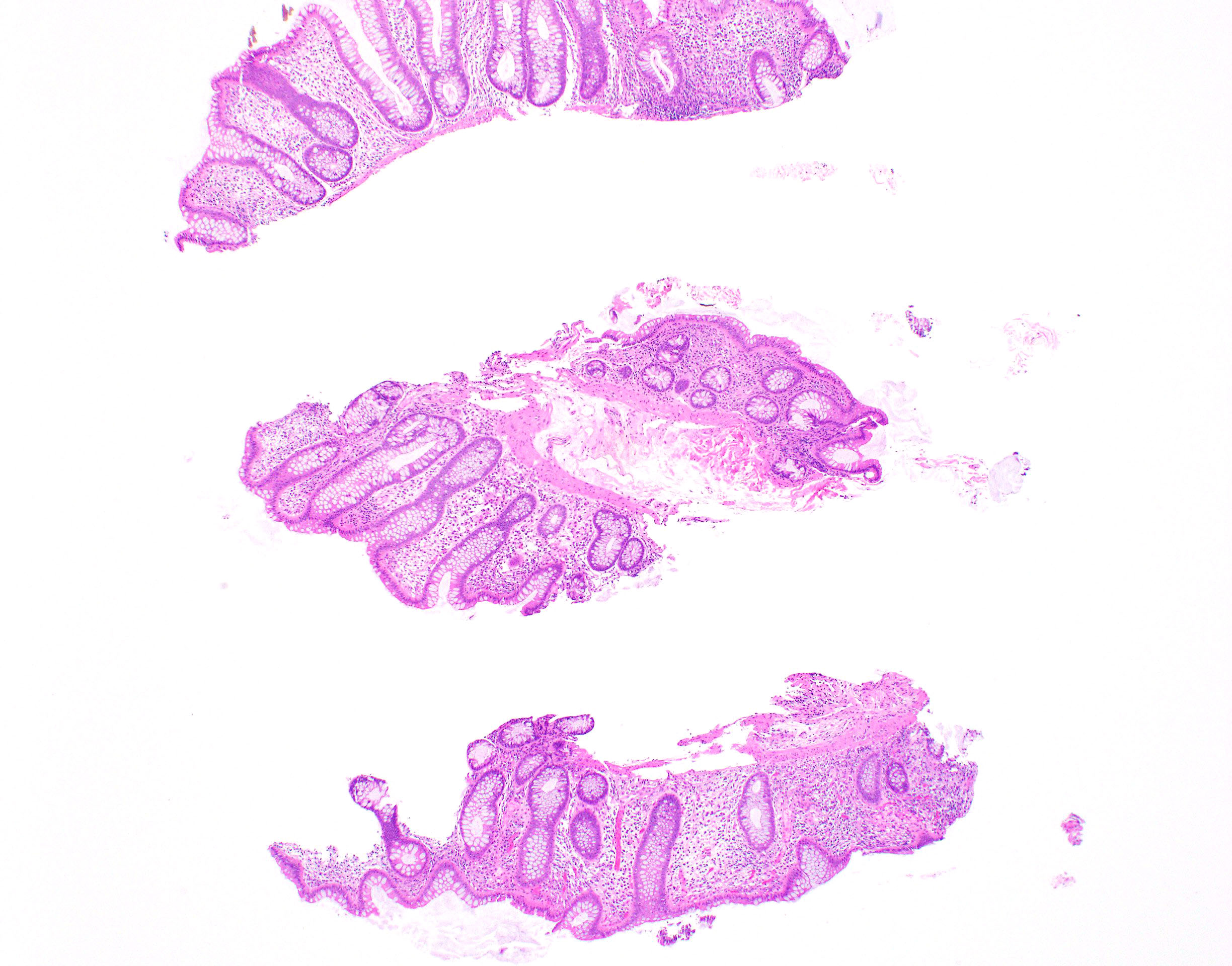
Architectural distortion
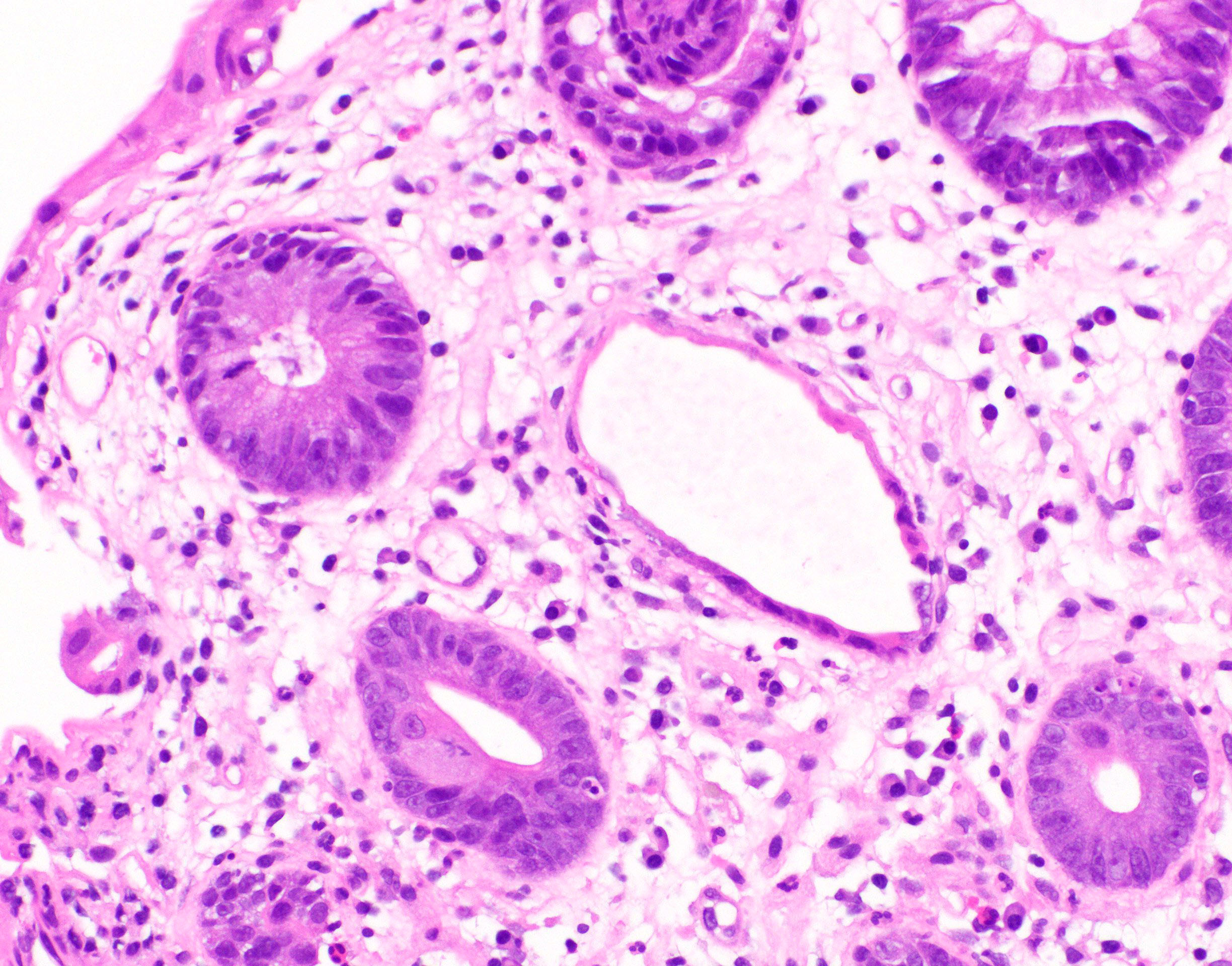
Injured crypt
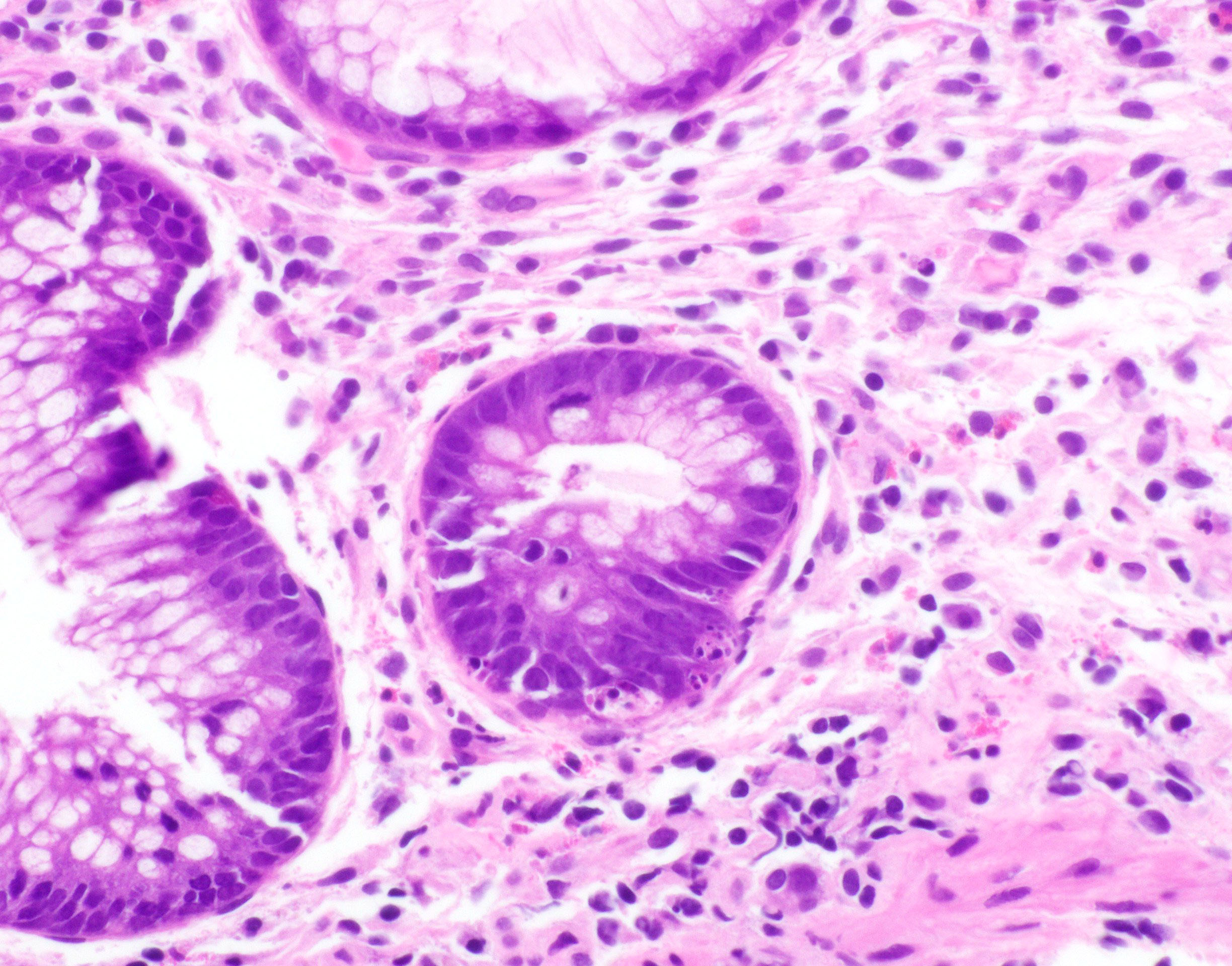
Apoptosis
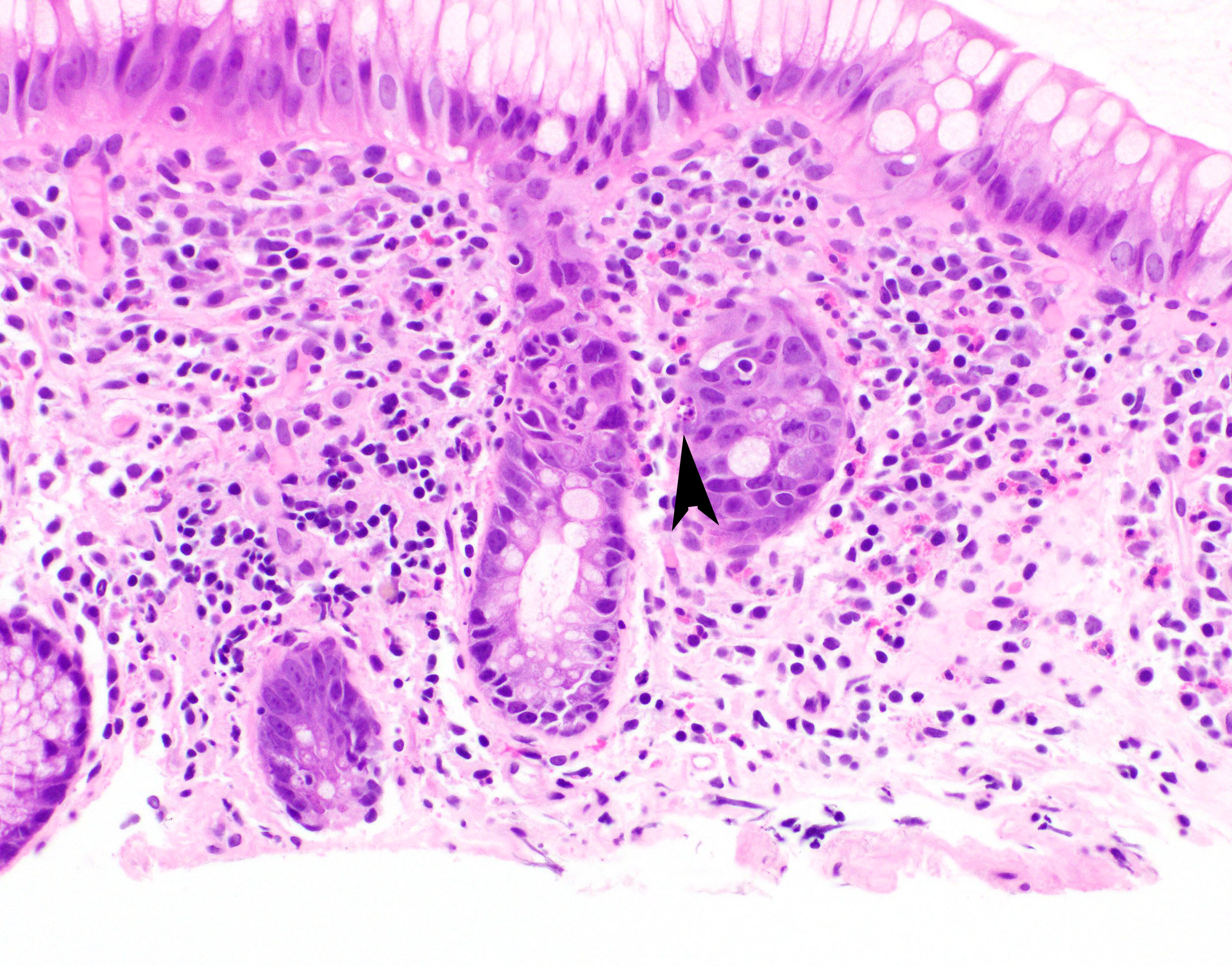
Inflammation
Negative stains
- CMV immunostain
Sample pathology report
- Colon, biopsy:
- Colonic mucosa with increased crypt apoptosis and mild architectural distortion (see comment)
- Comment: Given the patient’s reported use of mycophenolate, the histologic features are suggestive of mycophenolate colitis (or give differential diagnosis as appropriate).
Differential diagnosis
- Cytomegalovirus (CMV) colitis:
- Presence of viral inclusions on H&E or immunohistochemistry
- Graft versus host disease (GVHD):
- Fewer lamina propria eosinophils
- Presence of apoptotic microabscesses
- Presence of endocrine cell aggregates in lamina propria (Am J Surg Pathol 2013;37:1319)
- Exceedingly rare in solid organ transplant patients
- Inflammatory bowel disease:
- Prominent neutrophilic cryptitis and crypt abscess with architectural distortion
- Limited crypt apoptosis
- Clinical history is important (bloody diarrhea, lack of mycophenolate use)
Practice question #1
A 45 year old man who underwent a kidney transplant one year ago presents complaining of watery diarrhea. A colonoscopy and biopsy are performed. CMV immunohistochemistry is negative. Based on the histologic findings, which of the following is the most likely diagnosis?
- Graft versus host disease
- Infectious colitis
- Mycophenolate toxicity
- Ulcerative colitis
Practice answer #1
Practice question #2
Which of the following histologic features is not helpful in distinguishing mycophenolate toxicity from graft versus host disease?
- Apoptotic microabscesses
- Architectural distortion
- Endocrine cell aggregates
- Eosinophilic inflammation
Practice answer #2
