Heart & vascular pathology
General
Histology
Authors: Andrew J. Layman, M.D., Melanie C. Bois, M.D.
Resident / Fellow Advisory Board: David B. Chapel, M.D.


Last author update: 21 September 2022
Last staff update: 21 September 2022
Copyright: 2015-2025, PathologyOutlines.com, Inc.
PubMed Search: Histology [title] heart [TIAB] free full text[sb]
Table of Contents
Definition / general | Essential features | Physiology | Clinical features | Laboratory | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Immunohistochemistry & special stains | Electron microscopy description | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Layman AJ, Bois MC. Histology. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/hearthistology.html. Accessed September 14th, 2025.
Definition / general
- Specialized muscle cells, namely cardiomyocytes, allow for synchronized contractions to facilitate the pumping of blood throughout the body
Essential features
- Heart wall consists of 3 layers: endocardium, myocardium and epicardium
- Variation in the relative thickness of each of these layers exists between ventricles and atria, and between left and right sided chambers
- Myocardium is primarily composed of cardiac myocytes: specialized striated muscle cells organized in fascicles and bands
Physiology
- Heart serves as a pump that drives 2 parallel vascular circuits:
- Systemic circuit:
- Blood is ejected from the left ventricle through the aortic valve during systole at a normal pressure of 120 mmHg
- Blood travels through the ascending aorta, aortic arch and descending aorta; it then progresses through peripheral arteries, arterioles and eventually the systemic capillary beds, before entering the venous return
- Systemic venous blood returns to the right atrium from the superior and inferior vena cava at a pressure of < 5 mmHg
- Pulmonic circuit:
- Spontaneous contraction of the right atrium moves deoxygenated blood through the tricuspid valve to the right ventricle
- Ventricular contraction (systole) moves blood from the ventricle through the pulmonic valve to the pulmonary artery at a normal pressure of 25 mmHg
- Blood travels through the arteries and arterioles of the lung before reaching the alveolar capillaries
- Newly oxygenated blood returns to the left atrium via 4 pulmonic veins at a normal pressure of approximately 10 mmHg
- Left atrial contraction moves blood through the mitral valve into the left ventricle
- Coronary circulation
- The subendocardium is the last layer in the cardiac wall to receive blood flow from the coronary arteries and is most prone to ischemic injury
- Systemic circuit:
- The cardiac conduction system allows for coordinated atrioventricular contraction via the conduction of electrical impulses by specialized myocardial cells (J Interv Card Electrophysiol 2016;46:9)
- Sinoatrial (SA) node:
- Pacemaker of the heart located near the sinotubular junction, where the superior vena cava meets the right atrium
- Depolarization of the sinoatrial node cells allows for conduction of the electrical impulse through the conduction tracts within the wall of the right atrium:
- Posterior tract (Thorel tract)
- Middle tract (Wenckebach tract)
- Anterior tract (Bachmann bundle): extends to left atrium
- Depolarization also facilitates atrial contraction
- Atrioventricular (AV) node:
- Receives impulses from the sinoatrial nodal tracts, in order to propagate electrical cardiac impulse and facilitate ventricular contraction
- Located in the right atrium, in the space between the ostium of the coronary sinus, septal leaflet of the tricuspid valve and tendon of Todaro (Koch triangle) (Koch triangle)
- Bundle of His:
- Located in the membranous septum that separates the right atrium from the left ventricle
- Relays electrical impulses to the left and right bundle branches of the ventricular (muscular) septum
- Sinoatrial (SA) node:
Clinical features
- Clinical evaluation of cardiac structure and function is multifaceted and may include:
- Imaging:
- Echocardiogram
- Stress echocardiogram
- Xray / computerized tomography
- Cardiac MRI
- Coronary artery angiography
- Testing:
- Electrocardiogram
- Biopsy (see below)
- Serology (see Laboratory section)
- Imaging:
- Common cardiac pathology specimens include:
- Endomyocardial biopsy (J Clin Pathol 2006;59:121):
- Interventionalist uses a bioptome via an endovascular procedure, to sample endocardium and myocardium from the right ventricular septum
- Most common indication for endomyocardial biopsy is in the setting of transplant rejection monitoring
- In the appropriate clinical context, biopsies may also be used for the evaluation of heart disease, especially if there is concern for myocarditis, amyloidosis, hemochromatosis, drug toxicity or storage disorders
- Septal myectomy:
- Surgeon enters the left ventricle, either through the aortic valve (after aortotomy) or through the apical ventricular wall (ventriculotomy)
- Endocardium and myocardium are shaved for evaluation of septal abnormalities seen on echocardiogram
- Most common indication / etiology is hypertrophic cardiomyopathy but in the right demographic ruling out amyloidosis or storage disease is prudent
- Apical core resection: full thickness ventricular wall excision, allowing for placement of a ventricular assist device
- Atriotomy: normally excised for access to the heart chambers in a valve replacement procedure
- Atrial appendage: may be excised during procedures to replace heart valves, to reduce stroke risk in atrial fibrillation or for coronary artery bypass (Eur J Cardiothorac Surg 2018;53:i33)
- Orthotopic heart transplant
- Autopsy
- Endomyocardial biopsy (J Clin Pathol 2006;59:121):
Laboratory
- Serologic markers of acute coronary syndrome (UpToDate: Biomarkers of Myocardial Injury Other Than Troponin [Accessed 15 January 2021]):
- Troponin I / troponin T:
- Normal proteins present in myocardium which are released into systemic circulation following myocyte injury
- May remain elevated for up to 10 - 14 days post insult
- Creatinine kinase (CK / CK-MB):
- Enzyme that is present in both cardiac and skeletal muscle
- Elevations begin 4 - 6 hours post insult and resolve within 36 - 48 hours
- Isoenzyme CK-MB is proportionally greater in cardiac muscle but is present in larger absolute quantities in skeletal muscle
- Formerly the preferred test of choice, now replaced by troponin due to its higher specificity for cardiac injury than CK-MB
- Myoglobin:
- Heme complexed protein that is present in wide range of cell types and is released in response to damage
- Low specificity makes this an antiquated test that should rarely be employed
- Lactate dehydrogenase:
- Legacy test, no longer in use
- Troponin I / troponin T:
- Serologic markers of heart failure (UpToDate: Natriuretic Peptide Measurement in Heart Failure [Accessed 15 January 2021]):
- Brain natriuretic peptide (BNP, proBNP, NT proBNP)
- Three distinct proteins / cleavage products initially found in brain but also present in ventricular myocytes
- Released in response to increased ventricular pressure
- Elevated BNP is highly sensitive but not very specific for heart failure
- Atrial natriuretic peptide (ANP)
- Protein present in atrial myocytes
- Released in response to dilation of atria due to increased volumes
- Brain natriuretic peptide (BNP, proBNP, NT proBNP)
Gross description
- Isolated myocardial specimens:
- Endocardium: thin, shiny, translucent layer without fibrotic (tan-white) thickening
- Myocardium: uniform tan-brown to red striated tissue with firm but pliable texture
- No areas of gray-brown mottling and no areas of dense fibrosis
- Epicardium: thin, shiny and translucent without fibrosis; epicardial fat may be present
- Explant and autopsy specimens:
- Evaluation of the surgical or autopsy specimen should be conducted with a systematic approach (Allen: Moss & Adams' Heart Disease in Infants, Children, and Adolescents, 8th Edition, 2012)
- In addition to review of clinical history, gross evaluation should include the following:
- Position in the thoracic cavity
- Sidedness (situs)
- Evaluation of systemic connections and epicardial surface
- Coronary artery distribution and patency
- Inspection of endocardium and myocardium via short axis sectioning and opening of chambers along lines of blood flow
- Inspection for septal defects
- Evaluation of semilunar and atrioventricular valves
- Determination of atrioventricular concordance
- Measurement of heart weight, wall thickness and chamber dimension (at midventricular level)
Gross images
Normal cardiac specimen
Contributed by Melanie C. Bois, M.D.

Heart, anterior view

Heart, short axis section
Microscopic (histologic) description
- Endocardium (innermost layer):
- Thin tissue which lines all 4 chambers of the heart
- Consists of 3 layers: endothelium, subendothelium and elastic layer
- Endothelium is a thin single cell layer that is continuous with the endothelial lining of the systemic vasculature
- Subendothelial layer may have variable thickness; it is most prominent in the left atrium
- Elastic layer is the thickest layer of the endocardium and shows prominent elastic fibers admixed with smooth muscle cells
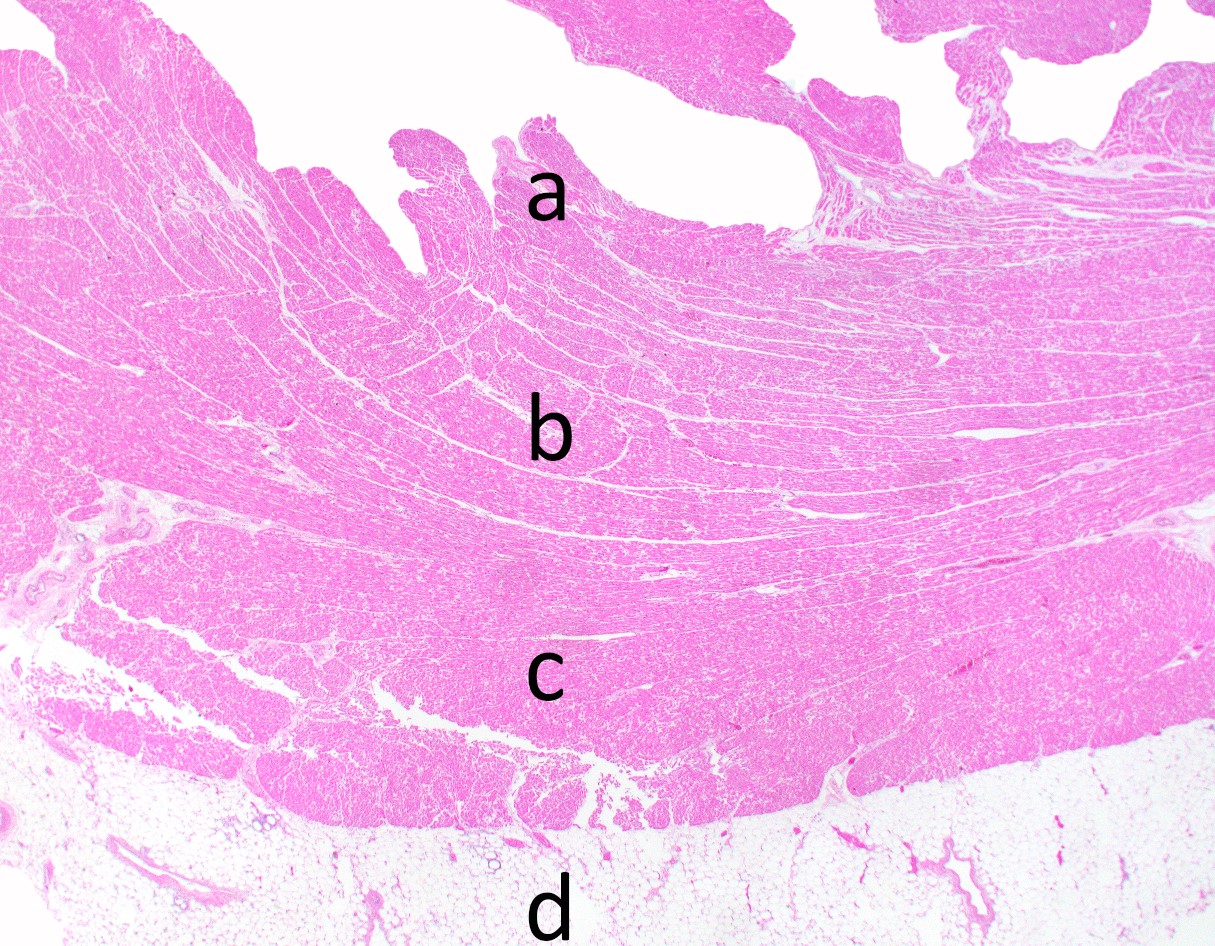
- Myocardium (middle layer):
- Organized in 3 layers / regions:
- Subepicardial (superficial)
- Middle
- Subendocardial (deep)
- Cardiac myocytes:
- Striated involuntary muscle cells measuring approximately 10 - 20 micrometers in diameter (3 - 5 red blood cells thick)
- Components:
- Sarcolemma: thin cell membrane
- Nucleus: small, round and basophilic, approximately the size of 1 red blood cell
- Sarcoplasm:
- Contains longitudinal myofibers composed of myofilaments, giving it the striated appearance
- Myofilaments (actin and myosin) are arranged in a staggered pattern to form the sarcomere, the contractile unit of the myocyte
- Interstitium:
- Composed of fibroblasts, extracellular matrix, adipocytes and scattered inflammatory cells
- Penetrating capillaries and arterioles originating from the epicardial coronary arteries are present throughout the interstitium and supply blood and oxygen to the cardiac myocytes, in an epicardial to subendocardial distribution
- Organized in 3 layers / regions:
- Epicardium (outermost layer) (Prog Cardiovasc Dis 2017;59:327):
- Composed of mesothelial cells that are part of the innermost layer of pericardium (visceral pericardium), along with subjacent fibroconnective and vascular tissue
- Benign fibrotic thickening may occur over the anterior surface of the heart giving rise to the soldier's patch
- Epicardial fat may also be considered part of the epicardial layer
- Reference: Buja: Cardiovascular Pathology, 4th Edition, 2015
Microscopic (histologic) images
Contributed by Melanie C. Bois, M.D.
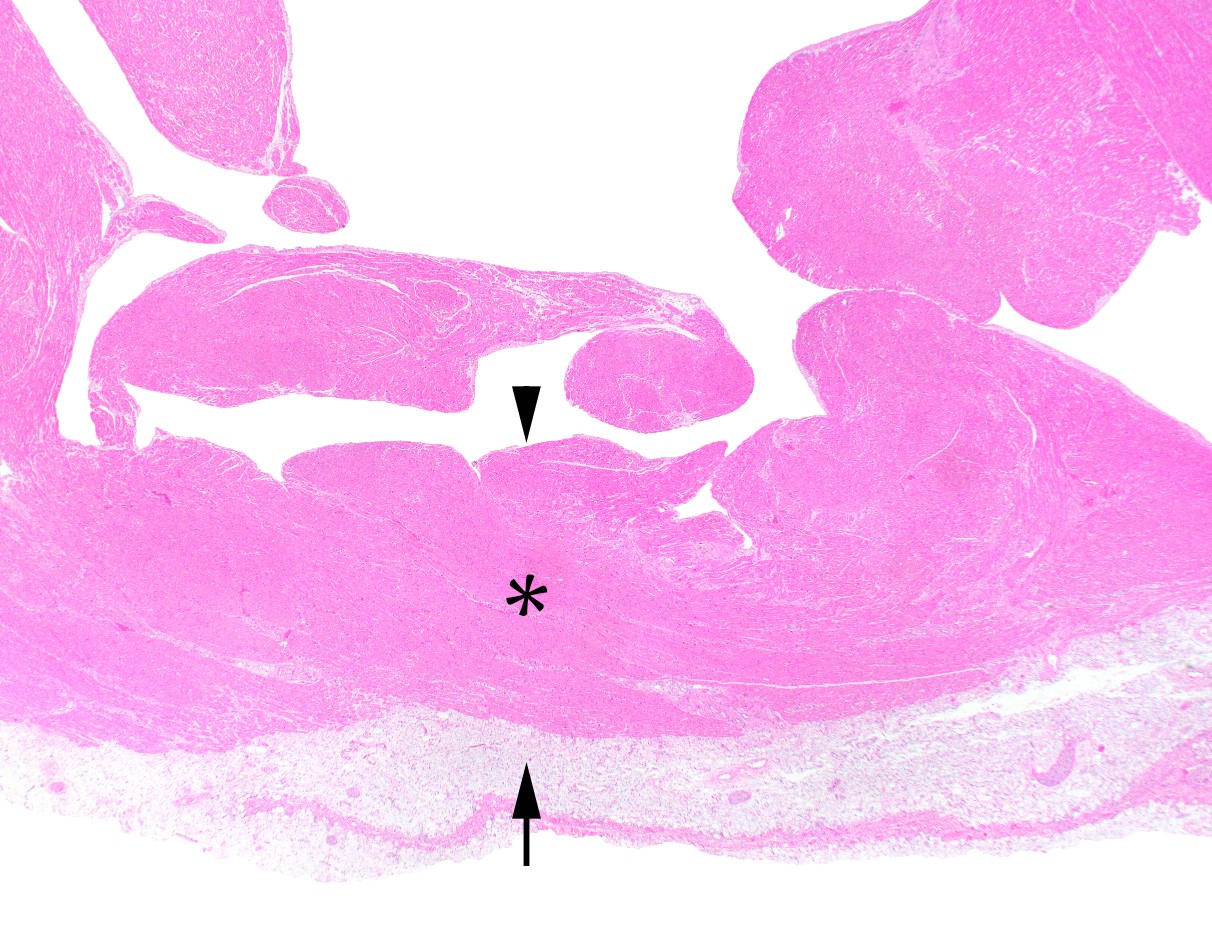
Heart, microscopy
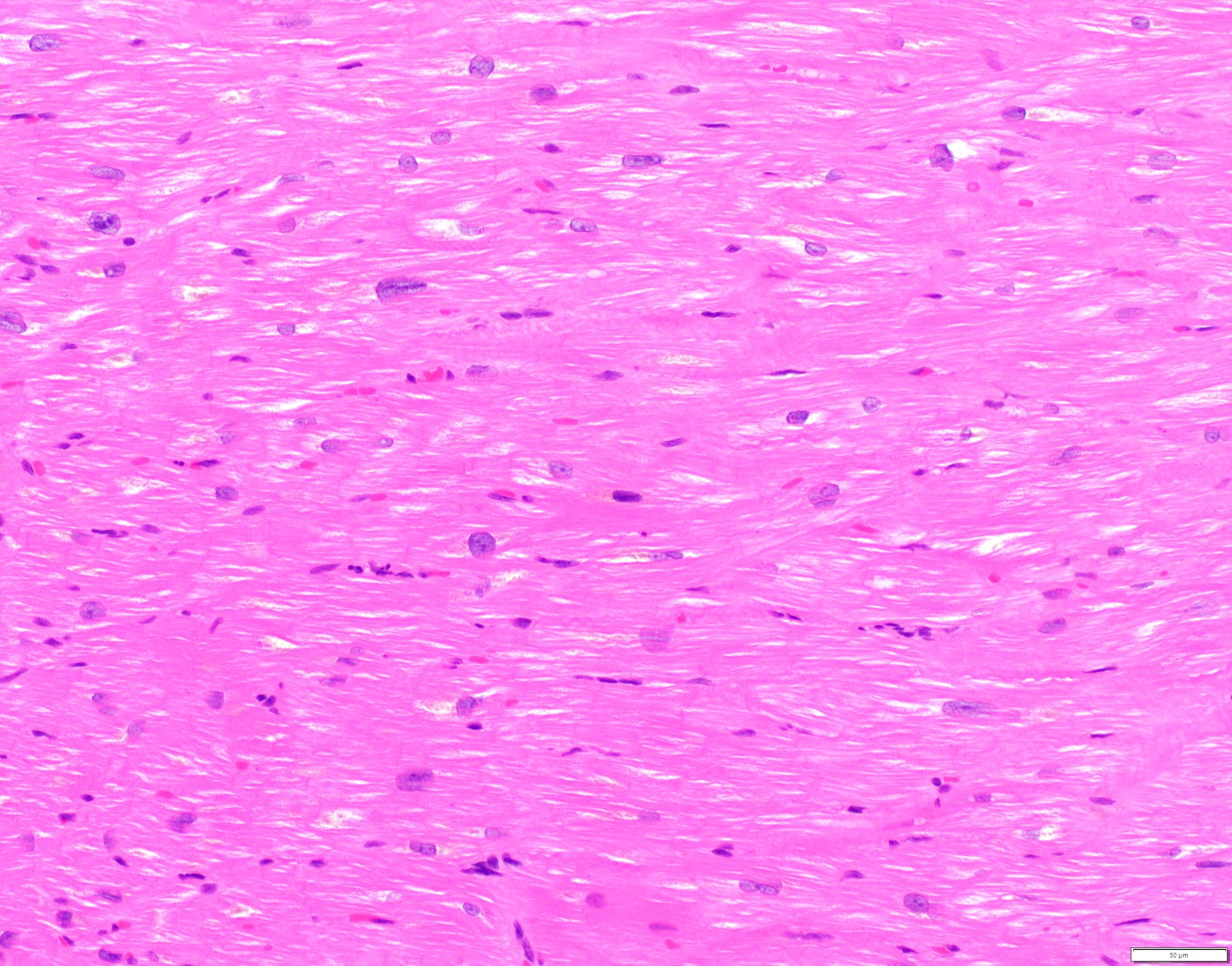
Cardiomyocytes
Immunohistochemistry & special stains
- Immunohistochemical stain targeting skeletal muscle will also stain cardiac myocytes
- IHC: actin, desmin, vimentin (Cytobios 1986;45:195)
- Special stains may be used in evaluation of normal myocardium:
- Congo red in the evaluation for amyloid (apple green birefringence) (Hum Pathol 2014;45:1766)
- Sulfated Alcian blue in the evaluation for amyloid (sea foam green) (J Clin Pathol 1976;29:22)
- Prussian blue in the evaluation for iron (Rev Esp Patol 2019;52:45)
- Masson trichrome in the evaluation for interstitial fibrosis (Circulation 2018;138:1224)
Electron microscopy description
- Sarcomere (Environ Health Perspect 1978;26:159):
- Composed of myofilaments arranged in a staggered pattern (alternatively actin and myosin)
- Bound by perpendicular electron dense Z bands
- Contraction pulls Z bands closer and relaxation allows for them to move further apart
- Orderly spacing of parallel myofilaments
- Nucleus:
- Fine chromatin with single nucleolus
- Mitochondria:
- Circular to ovoid structures of relatively uniform size with prominent layered cristae
- Intercalated disk:
- Jagged electron dense line representing cell - cell junctions between myocytes
- Lipofuscin:
- Radio dense material associated with age related changes
- Often perinuclear in distribution
Practice question #1
Which location is the last to receive blood flow from the coronary arteries (i.e. the zone most prone to ischemic injury)?
- Subendocardium
- Midmural myocardium
- Subepicardium
- Epicardium
Practice answer #1
Practice question #2
Which structure is referred to as the pacemaker of the heart?
- Atrioventricular node
- Bachmann bundle
- Bundle of His
- Sinoatrial node
Practice answer #2
