
Microbiology & infectious diseases
Parasites-gastrointestinal (not liver)
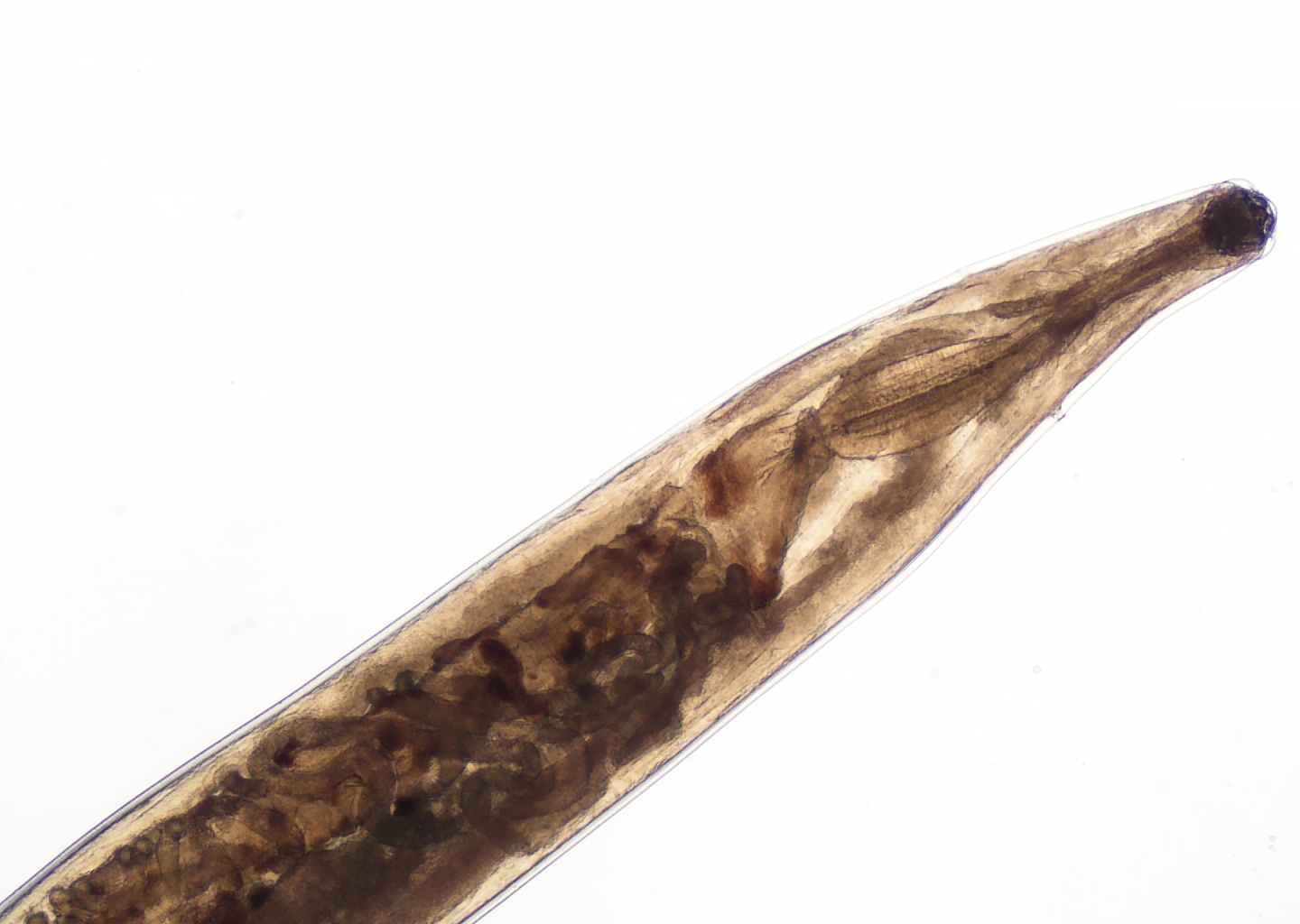
Hookworm
Deputy Editor-in-Chief: Patricia Tsang, M.D., M.B.A.


Last author update: 23 August 2023
Last staff update: 24 July 2025
Copyright: 2019-2025, PathologyOutlines.com, Inc.
PubMed Search: Hookworm

Table of Contents
Definition / general | Essential features | Epidemiology | Sites | Pathophysiology | Diagrams / tables | Clinical features | Diagnosis | Laboratory | Case reports | Treatment, prevention and control | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Peripheral smear description | Positive stains | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Adams SH, Pritt BS, Totten AH. Hookworm. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/parasitologyhookworm.html. Accessed September 3rd, 2025.
Definition / general
- Intestinal hookworm infection (necatoriasis and ancylostomiasis) is caused by the nematodes Necator americanus, Ancylostoma duodenale and Ancylostoma ceylanicum
- A. caninum (dog hookworm) may cause eosinophilic enteritis in humans but does not reach reproductive maturity
- Ancylostomiasis is historically known as uncinariasis
- Estimated 500 million people infected with hookworms worldwide (Lancet 2015;386:743)
- Extraintestinal hookworm infection (cutaneous larva migrans), caused by A. caninum, A. brazilense and Uncinaria stenocephala, is discussed in the Skin nontumor chapter
Essential features
- Intestinal hookworm infection attributed to the hookworms Necator americanus, Ancylostoma duodenale and Ancylostoma ceylanicum
- Predominates in tropical / subtropical regions with poor sanitation / hygiene
- Chronic iron deficiency anemia and malnutrition are major clinical features of infection, though hookworm dermatitis (ground itch at the site of initial penetration) and pneumonitis (Löeffler syndrome) are also important manifestations
Epidemiology
- Risk factors: extreme poverty, poor sanitation and hygiene, open defecation, discharge of raw sewage to the ground outside of a treatment system (straight piping), rural habitation, walking barefoot on contaminated soil, travel to / immigration from endemic areas (PLoS Med 2014;11:e1001620, Am J Trop Med Hyg 2005;73:386)
- Use of human fecal sludge fertilizer (night soil) (Trop Med Int Health 2018;23:692)
- Age: hookworm infection intensity increases with age, plateaus in adulthood (like strongyloidiasis; unlike other soil transmitted helminth infections) (N Engl J Med 2004;351:799)
- Geographic location
- Tropics and subtropical coastal regions with poor sanitation (N Engl J Med 2004;351:799)
- Necator americanus and Ancylostoma duodenale: Asia, Latin America, Caribbean, Africa, Australia, possibly the rural United States (Am J Trop Med Hyg 2017;97:1623, Am J Trop Med Hyg 2011;85:680, Trop Med Infect Dis 2023;8:212)
- Only N. americanus is found in southern India; N. americanus also predominates in the Americas
- In the Middle East, North Africa and northern India, only A. duodenale is found
- Recent detection of N. americanus in the rural United States was based on PCR only and not confirmed by microscopy
- Ancylostoma ceylanicum: Southeast Asia (Laos, Malaysia, Thailand), Australia, Japan, South Africa, Madagascar, Guyana, Suriname, Pacific Islands, United Arab Emirates (Int J Parasitol 2013;43:1009, Clin Microbiol Infect 2015;21:426, Emerg Infect Dis 2017;23:252)
Sites
- Larval stage: skin (ground itch) → vascular system → lungs (Löeffler syndrome) → bronchi → trachea → esophagus (N Engl J Med 2004;351:799)
- Adult worms: small intestines
- Eggs: intestine → fecal material → environment
Pathophysiology
- Eggs passed in feces to environment hatch into rhabditiform larvae (L1) within 48 hours, molt twice to L3 larvae (infectious stage) and quest for host (can survive for 3 - 4 weeks)
- L3 larvae penetrate skin upon contact with host (ground itch) and migrate via vasculature to lung capillaries and into pulmonary parenchyma (Adv Parasitol 2004;58:197)
- Hookworm pneumonitis (Löeffler syndrome) caused during pulmonary migration; larvae then migrate up the trachea and oropharynx and are swallowed (Adv Parasitol 2004;58:197)
- In the small intestine (typically distal jejunum), larvae develop into the adult stage in 6 - 8 weeks and attach to the intestinal mucosa
- Adults attach to host submucosa by specialized mouthparts and feed on host blood (intestinal hookworm infection) (Nat Rev Dis Primers 2016;2:16088)
- Following mating, female adult is able to produce 10,000 - 28,000 eggs/day (PLoS Med 2005;2:e67)
- Life span: 1 year (A. duodenale); upward of 3 - 5 years (N. americanus)
- Rhabditiform larvae can rarely become dormant in skeletal muscles (Clin Microbiol Rev 2001;14:689)
- A. ceylanicum and A. caninum may also be acquired by oral ingestion
- A. duodenale may possibly be acquired by oral ingestion and via the transmammary route (N Engl J Med 2004;351:799, Lancet Microbe 2022;3:e72, Clin Microbiol Rev 2001;14:689, Adv Parasitol 2004;58:197)
Diagrams / tables
Images hosted on other servers:

Global distribution of human hookworm infection

Hookworm life cycle
Clinical features
- Mostly asymptomatic (67 - 75%); clinical manifestations relative to worm burden
- Chronic iron deficiency (microcytic) anemia, intestinal blood loss, protein deficiency, malnutrition (high worm burden) and adverse pregnancy outcomes (rare) (Nutr Rev 1997;55:223)
- A. duodenale is associated with greater blood loss than N. americanus
- 0.1 - 0.2 mL of blood loss per day (per each adult A. duodenale)
- 0.01 - 0.02 mL of blood loss per day (per each adult N. americanus) (Despommier: Parasitic Diseases, 7th Edition, 2019)
- Plasma hypoproteinemia, hypoalbuminemia, characteristic abdominal distension, edema, alopecia, failure to thrive
- A. duodenale is associated with greater blood loss than N. americanus
- Hookworm dermatitis (ground itch) is characterized by vascular dermatitis at the site of larval entry (N Engl J Med 2004;351:799)
- Erythematous pruritic macules and papules, scattered or in groups, on the soles, toe webs and ankles; later, these become vesicular, purulent and ulcerated (James: Andrews' Diseases of the Skin, 13th Edition, 2019)
- Hookworm pneumonitis (Löffler syndrome): increased blood and pulmonary eosinophilia, fever cough and alveolar hemorrhage during larval migration though lung (Chest 2014;145:883, N Engl J Med 2004;351:799)
Diagnosis
- Most commonly diagnosed by finding eggs in concentrated stool exam (i.e., ova and parasite exam [O&P]; formalin ethyl acetate sedimentation or related technique, sensitivity: 30 - 88%) (Trop Parasitol 2017;7:86)
- Cannot differentiate species based on morphology
- Occasionally L1 larvae seen in stool with processing delay; must differentiate from Strongyloides stercoralis L1 larvae (Trop Parasitol 2017;7:86)
- Direct visualization of adult hookworms in small intestine by endoscopy (e.g., during routine screening colonoscopy) or rarely, gross identification in stool specimen
- PCR / NAAT tests for diagnosis and species identification rare; serology for identification only in a research setting (Trop Parasitol 2017;7:86)
- Detection in histologic sections (adults or egg in intestinal mucosa), 5 - 15 mm in length, body cavity (0.5 mm diameter), thick cuticle, buccal capsule with teeth or cutting plates blunt posterior with spicules (male) or tapered posterior (female)
- Hookworm pneumonitis: larvae can rarely be identified in sputum or gastric washing specimens during the pulmonary migration stage but it is mainly a clinical diagnosis (Trop Parasitol 2017;7:86, Chest 2014;145:883)
Laboratory
- Low hematocrit, low ferritin, eosinophilia (60% of infections) (Trop Parasitol 2017;7:86)
Case reports
- 2 month old Italian girl with an A. duodenale infection by likely transplacental transmission (Ital J Pediatr 2021;47:26)
- 24 year old Korean man with A. duodenale in refractory irritable bowel syndrome (Clin Endosc 2013;46:671)
- 62 year old man in Chongqing, China with decreasing central vision in 1 eye (Lancet Infect Dis 2018;18:582)
- 19 of 55 (34.5%) fecal samples in rural Lowndes County, Alabama showed PCR positivity for N. americanus (Am J Trop Med Hyg 2017;97:1623)
- 2.1% of stool samples in California refugee clinic showed positivity for hookworms (Am J Trop Med Hyg 2005;73:386)
Treatment, prevention and control
- Anthelmintic drugs: albendazole, mebendazole, pyrantel pamoate and supportive care including iron supplementation, blood transfusion in at risk populations
- Annual deworming programs in endemic regions
- Long term community prevention requires improvements in water, sanitation and hygiene in addition to targeted anthelmintic therapy to prevent cycle of reinfection (Trends Parasitol 2003;19:405, PLoS Med 2014;11:e1001620)
- Vaccines not available but research is ongoing for candidate compounds (Vaccine 2022;40:6084, J Allergy Clin Immunol 2022;150:157)
Clinical images
Images hosted on other servers:

Edema from heavy hookworm infection

Adult A. caninum hookworms in canine small intestine
Gross description
- Adults are tan-white, tubular / cylindrical, linear, with head often slightly bent in hook shape; have oval buccal capsule at the anterior end
- Males have an expanded posterior end and females have a pointed / tapered posterior end
- Ancylostoma spp.: adults are between 8 and 13 mm in length (females slightly larger); diameter between 0.4 and 0.6 mm
- N. americanus: adults are between 5 and 9 mm (males) and 9 and 11 mm (females) in length; diameter is ~0.5 mm (Adv Parasitol 2004;58:197)
Gross images
Contributed by Bobbi S. Pritt, M.D., M.Sc.

Female and male Ancycloctoma duodenale
Microscopic (histologic) description
- Eggs are thin shelled and colorless, evaluated on wet mount with Lugol's iodine; contain < 8 blastomeres with space between blastomeres and outer shell (Adv Parasitol 2004;58:197, Cross: Enteric Nematodes of Humans [Accessed 3 August 2023])
- Range of 55 - 65 μm long by 36 - 40 μm wide (cannot speciate with eggs) (Adv Parasitol 2004;58:197, Res Rep Trop Med 2021;12:181)
- Adult hookworm: typically only seen in worms extracted during colonoscopy and in formalin fixed paraffin embedded H&E sections (BMJ Case Rep 2014;2014:bcr2014204065, J Clin Gastroenterol 1997;24:100, Endoscopy 2007;39:E306)
- Eggs / adult forms in intestinal (duodenum / jejunum) mucosa (BMJ Case Rep 2014;2014:bcr2014204065)
- Length (5 - 15 mm) on longitudinal cut and diameter (~0.5 mm) on transverse cut in tissue sections
- Buccal capsule (mouth) can be used for species differentiation (best on intact specimens): mouth with 4 hook-like teeth (Ancylostoma spp.); cutting plates (N. americanus)
- L1 larvae may embryonate in stool with delay in fresh stool specimen processing (Res Rep Trop Med 2021;12:181)
- 250 - 350 μm in length and have long buccal canal, inconspicuous genital primordium
- Hookworm dermatitis: dermal lymphocytic infiltrate with eosinophils (dermal hypersensitivity reaction), findings are not specific; rarely, specimen may contain larvae
Microscopic (histologic) images
Contributed by Bobbi S. Pritt, M.D., M.Sc. and @surgpathcases on Instagram

Multiple spicules of male Ancycloctoma duodenale

Buccal canal comparison, hookworm and Strongyloides

Hookworm egg with thin, colorless shell


Cutting plates of N. americanus

Hookworm
Cytology description
- Cytology useful in evaluation of sputum / BAL samples
Peripheral smear description
- Though L3 larvae migrate through the peripheral vasculature, they are generally not identified on peripheral blood smear
Positive stains
- Lugol's iodine stain: nonspecific; contrast dye that aids in differentiating parasites from background cells on concentrated stool wet preparations
- Methylene blue - glycerol has been described (J Parasitol Res 2014;2014:672018)
Differential diagnosis
- Hookworm eggs in stool specimens:
- Trichuris trichiura eggs:
- Barrel shaped, thick shelled, yellow to brown in color (bile staining), polar plugs at either end (Trop Parasitol 2017;7:86)
- Ascaris lumbricoides eggs (Trop Parasitol 2017;7:86):
- Thick walled eggs with outer bumpy (mamillated) shell
- Bile staining
- May mimic hookworm eggs if mamillated layer is lost (i.e., decorticated state)
- Trichostrongylus sp. eggs:
- Thin shelled and colorless like hookworm eggs but larger and have a longer length to width ratio than hookworm eggs, measuring 75 - 95 μm in length by 40 - 50 μm in width (CDC: Trichostrongylosis [Accessed 18 July 2023])
- Oesophagostomum sp. (nodular worm) eggs (CDC: Oesophagostomiasis [Accessed 18 July 2023]):
- Morphologically indistinguishable from hookworm eggs
- Geographically, human infection is seen mainly in northern Togo and Ghana
- Clinically presents as right lower abdominal pain; adults reside in large intestine
- Schistosoma japonicum eggs:
- Small / unapparent spine
- Larger than hookworm eggs (> 70 μm long)
- Trichuris trichiura eggs:
- Adult stage:
- Ascaris lumbricoides:
- Larger, with both females (20 - 49 cm long, 3 - 6 mm diameter) and males (15 - 31 cm long, 2 - 4 mm diameter)
- Posterior end is curved
- Trichuris trichiura:
- Whip shaped worm
- 30 - 50 mm long with varying diameter based on section
- Enterobius vermicularis (Dtsch Arztebl Int 2019;116:213):
- Females (8 - 13 mm) are similar in size to hookworm; males are 2 - 5 mm
- Visible distinctive muscular and bulbous portions of esophagus
- Adults aggregate in cecum, appendix or ascending colon
- Clinical history of perianal pruritus
- Significant anemia or eosinophilia uncommon
- Other common mimickers include mucus cords, vegetable matter and chewing gum (Lab Med 2008;39:114)
- Ascaris lumbricoides:
- L1 larvae:
- May embryonate in stool with delay in processing, hookworm L1 larvae should be differentiated from Strongyloides stercoralis L1 larvae (normal stool finding)
- Hookworm L1 larvae:
- 250 - 350 μm long with long buccal canal
- Inconspicuous genital primordium
- S. stercoralis L1 larvae:
- 180 - 380 μm long with short buccal canal
- Prominent genital primordium
- Hookworm L1 larvae:
- May embryonate in stool with delay in processing, hookworm L1 larvae should be differentiated from Strongyloides stercoralis L1 larvae (normal stool finding)
- Skin infection:
- Tinea pedis, bacterial intertrigo, urticarial dermatitis
Additional references
Practice question #1

Hookworm eggs are identified on routine stool ova and parasite exam. How are the hookworms Necator americanus and Ancylostoma duodenale differentiated morphologically?
- Ancylostoma duodenale eggs have barrel shaped, thick shelled, polar plugs at either end, while Necator americanus eggs lack these features
- Ancylostoma duodenale eggs show bile staining, while Necator americanus eggs do not
- It is impossible to morphologically differentiate Necator americanus and Ancylostoma duodenale eggs
- Necator americanus eggs have a small spine, while Ancylostoma duodenale eggs have have no spine
- Necator americanus eggs have a thick shell with an external mammillated layer, while Ancylostoma duodenale eggs have a thinner shell and a variable mammillated layer
Practice answer #1
C. It is impossible to morphologically differentiate Necator americanus and Ancylostoma duodenale eggs. Hookworm eggs, both Necator americanus and Ancylostoma duodenale, are thin shelled and colorless, without bile staining. Hookworm eggs generally only develop larvae in soil after fecal excretion over weeks' time. It is impossible to morphologically differentiate Necator americanus and Ancylostoma duodenale eggs. Identification to the species level is not necessary for clinical management. Hookworm eggs identified is sufficient for case sign out. Answer D is incorrect because a small lateral spine is a feature of Schistosoma japonicum eggs. Answer E is incorrect because a thick shell with an external mammillated layer is seen in eggs of fertilized Ascaris lumbricoides; the unfertilized eggs have a thinner shell and variable mammillated layer; both forms show bile staining. Answer A and B are incorrect because a barrel shape, thick shell, bile staining and polar plugs at either end are features of Trichuris trichiura eggs.
Comment Here
Reference: Hookworm
Comment Here
Reference: Hookworm
Practice question #2
A 73 year old woman visiting the United States from a rural village in India presents with weight loss, fatigue and epigastric pain. Labs show hemoglobin (Hb) 7 g/dL, ferritin 9 ng/mL and 850 eosinophils/μL. Fecal occult blood test is positive. Colonoscopy reveals numerous worms adherent to the proximal small bowel mucosa. Inspection of a retrieved specimen shows a tan-white, 9 mm long worm with a smooth surfaced cylindrical body with one end sharply bent. What is the identity of this worm?
- Ancylostoma duodenale
- Ascaris lumbricoides
- Enterobius vermicularis
- Oesophagostomum
- Trichuris trichiura
Practice answer #2
A. Ancylostoma duodenale. A hookworm has a smooth cylindrical body with a characteristic bent hook shaped head (Ancylostoma etymologically is crooked / curved mouth) and measures 5 - 11 mm in length. Answer C is incorrect because clinically, Enterobius vermicularis commonly presents with rectal pruritis rather than weight loss or fatigue, only rarely causes significant anemia and eosinophilia is unusual. Strongyloides stercoralis is much smaller than hookworm, measuring only ~2 mm long and is usually threaded through the small intestinal mucosa so that it is not readily visible. The organism itself would generally not be identified endoscopically without microscopic evaluation (World J Gastroenterol 2008;14:1768). Answer E is incorrect because Trichuris trichiura (or whipworm) resembles a whip, having a thickened body at one end and a narrow body at the opposing end. Trichuris prefers the large intestine over the duodenum inhabited by Ancylostoma duodenale. Trichuris is also considerably longer than hookworm, measuring 3 - 5 cm, compared to the 0.5 - 1.1 cm long hookworm. Answer B is incorrect because Ascaris lumbricoides are easily distinguishable from hookworm due to the size and length of Ascaris (15 - 49 cm), grossly resembling a common earthworm (Lumbricus) in size. Answer D is incorrect because oesophagostomiasis commonly presents as right lower abdominal pain and is most often seen in patients from Togo and Ghana. Though morphologically similar to hookworm, adult Oesophagostomum worms reside in the large intestine.
Comment Here
Reference: Hookworm
Comment Here
Reference: Hookworm
