Oral cavity & oropharynx
Potentially malignant & dysplasia
Leukoplakia
Editorial Board Member: Kelly Magliocca, D.D.S., M.P.H.
Editor-in-Chief: Debra L. Zynger, M.D.

Last author update: 15 February 2021
Last staff update: 15 February 2021
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Oral leukoplakia[TI] review[PT]
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Molecular / cytogenetics description | Molecular / cytogenetics images | Sample pathology report | Differential diagnosis | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Stojanov IJ. Leukoplakia. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/oralcavityleukoplakia.html. Accessed September 9th, 2025.
Definition / general
- Hyperkeratotic (white) plaque / patch of mucosa exhibiting clonality and representing precursor lesion to squamous cell carcinoma
- Approximately 40% of leukoplakias exhibit keratinizing dysplasia (Oral Surg Oral Med Oral Pathol Oral Radiol 2014;118:713)
- Remaining exhibit hyperkeratosis / parakeratosis characterized genomically by KMT2C, TP53, TIAM1 or other mutations (Oral Dis 2019;25:1707)
- Term leukoplakia / leukoplakic also used descriptively in clinical setting to denote any white lesion without a readily apparent diagnosis
- Such use may skew understanding of leukoplakia biology / behavior due to preponderance of frictional / reactive keratoses in oral cavity, which are not always recognizable clinically but have no malignant potential (Head Neck Pathol 2019;13:423)
- Defined by WHO as a white plaque of questionable risk having excluded (other) known diseases or disorders that carry no increased risk for cancer (J Oral Pathol Med 2007;36:575)
- Leukoplakia may occur throughout the upper aerodigestive tract
Essential features
- Hyperkeratotic (white) plaque / patch of mucosa exhibiting clonality and representing precursor lesion to squamous cell carcinoma
- Approximately 40% of leukoplakias exhibit keratinizing dysplasia; the remainder are characterized by hyperkeratosis alone
- Annual malignant transformation rate is 3% and most strongly predicted by presence of dysplasia on biopsy; increasing duration, increasing size and nonhomogenous appearance also associated with malignant transformation
- Leukoplakia exhibiting hyperkeratosis that is not frictional / reactive exhibits a malignant transformation rate of approximately 5%, similar to that of mild epithelial dysplasia
- Histologic appearance of leukoplakia indistinguishable from proliferative (verrucous) leukoplakia and requires clinical correlation
- Surgical excision reduces risk of malignant transformation approximately 3 times
Terminology
- Leukoplasia, erythroleukoplakia, erythroplakia
ICD coding
- ICD-10: K13.21 - Leukoplakia of oral mucosa, including tongue
Epidemiology
- Worldwide prevalence approximately 0.5% (Oral Oncol 2003;39:770, Oral Oncol 2009;45:317)
- Characteristically a disease of older males (M:F = 3:1)
Sites
- May present on any mucosal surface
- Associated with highest incidences of malignant transformation when occurring on ventrolateral tongue or floor of mouth (Oral Oncol 2009;45:317)
Pathophysiology
- Leukoplakia exhibiting keratinizing dysplasia characterized by genomic alterations including TP53 mutations and loss of heterozygosity at 3p and 9p (Cancer Prev Res (Phila) 2012;5:1081)
- Leukoplakia exhibiting hyperkeratosis alone characterized by genomic alterations including KMT2C, TP53 and TIAM1 mutations (Oral Dis 2019;25:1707)
- Genetic progression model of head and neck cancer not well worked out, particularly with regards to early precursor lesions (Clin Cancer Res 2000;6:347)
Etiology
- Associated with smoking / smokeless tobacco, alcohol and areca nut (betel quid) use
- HPV associated with only a very small percentage of cases (Mod Pathol 2017;30:1646)
Clinical features
- Hyperkeratosis on mucosal sites not amenable to frictional / factitial trauma, particularly when sharply demarcated, considered clinically concerning (J Oral Maxillofac Surg 2017;75:723)
- Biopsy proven leukoplakia may clinically appear homogenous or nonhomogenous (Oral Oncol 2009;45:317)
- Homogenous leukoplakia: uniformly thin or thick hyperkeratosis, frequently sharply demarcated
- Nonhomogenous leukoplakia: irregular texture with fissuring, nodular / verrucous components or erythematous components (erythroleukoplakia)
- Proliferative (verrucous) leukoplakia: uncommon and significantly more aggressive (60 - 100% malignant transformation rate) disease characterized by multifocal oral mucosal involvement and a predilection for middle aged / elderly females with no / minimal history of tobacco or alcohol exposure (Oral Dis 2018;24:749)
- Best considered a separate disease on the basis of differing demographic / clinical presentation, biologic behavior and patient management considerations
Diagnosis
- Biopsy required for diagnosis and risk stratification
- Leukoplakia with dysplasia readily diagnosed on basis of conventional histopathologic features of epithelial dysplasia (Head Neck Pathol 2019;13:423)
- Leukoplakia without dysplasia requires clinicopathologic correlation and exclusion of frictional / factitial features as identified clinically or histopathologically
Prognostic factors
- Annual malignant transformation rate 3% (Oral Oncol 1998;34:270)
- Presence of epithelial dysplasia most significant risk factor for malignant transformation (Oral Oncol 2009;45:317, Mod Pathol 2017;30:S112)
- Severe epithelial dysplasia: 28.4% risk
- Moderate epithelial dysplasia: 22.5% risk
- Mild epithelial dysplasia: 5.7% risk
- Hyperkeratosis: 4.9% risk
- Reported overall malignant transformation rates of 0.36 - 34% difficult to interpret due to historical inclusion of frictional / reactive keratoses in leukoplakia cohorts and variability in followup duration (J Oral Pathol Med 2016;45:155)
- Length of duration, increasing size and nonhomogenous appearance associated with increased risk of malignant transformation
Case reports
- 21 year old man with amalgam associated leukoplakia (J Oral Sci 2016;58:445)
- 59 and 66 year old men with tongue leukoplakia and squamous cell carcinoma (Mol Med Rep 2017;16:6780)
- 75 year old man with tongue lesion (Cleve Clin J Med 2020;87:133)
Treatment
- Surgical excision results in 3 times reduction in risk of malignant transformation (Head Neck 2009;31:1600)
- Leukoplakia with high grade (moderate / severe) dysplasia should be excised whenever possible
- Close clinical observation may be appropriate for extensive leukoplakia or patients with comorbidities but otherwise appears to have a limited role when conservative surgical management is possible (J Oral Maxillofac Surg 2017;75:723)
Clinical images
Contributed by Ivan J. Stojanov, D.M.D., M.M.Sc.

Left posterior maxillary leukoplakia

Right posterior maxillary leukoplakia
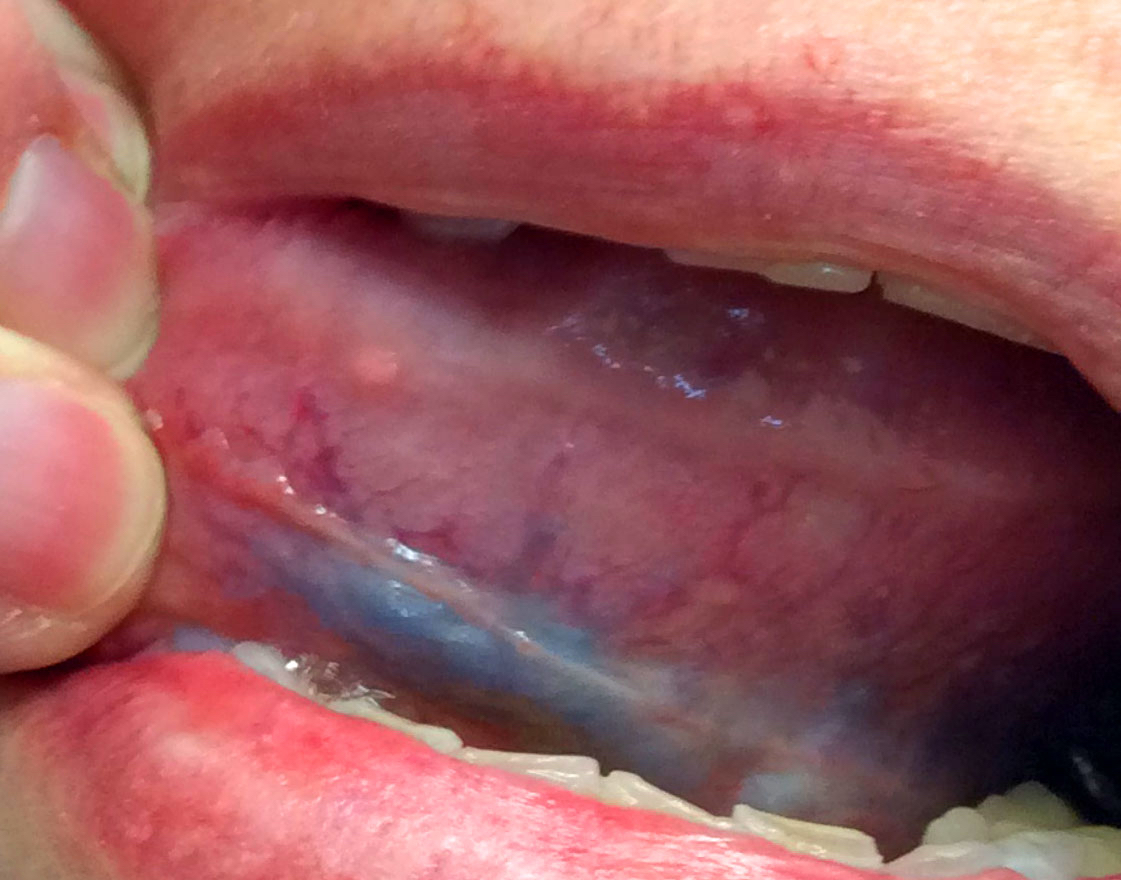
Left ventral tongue leukoplakia
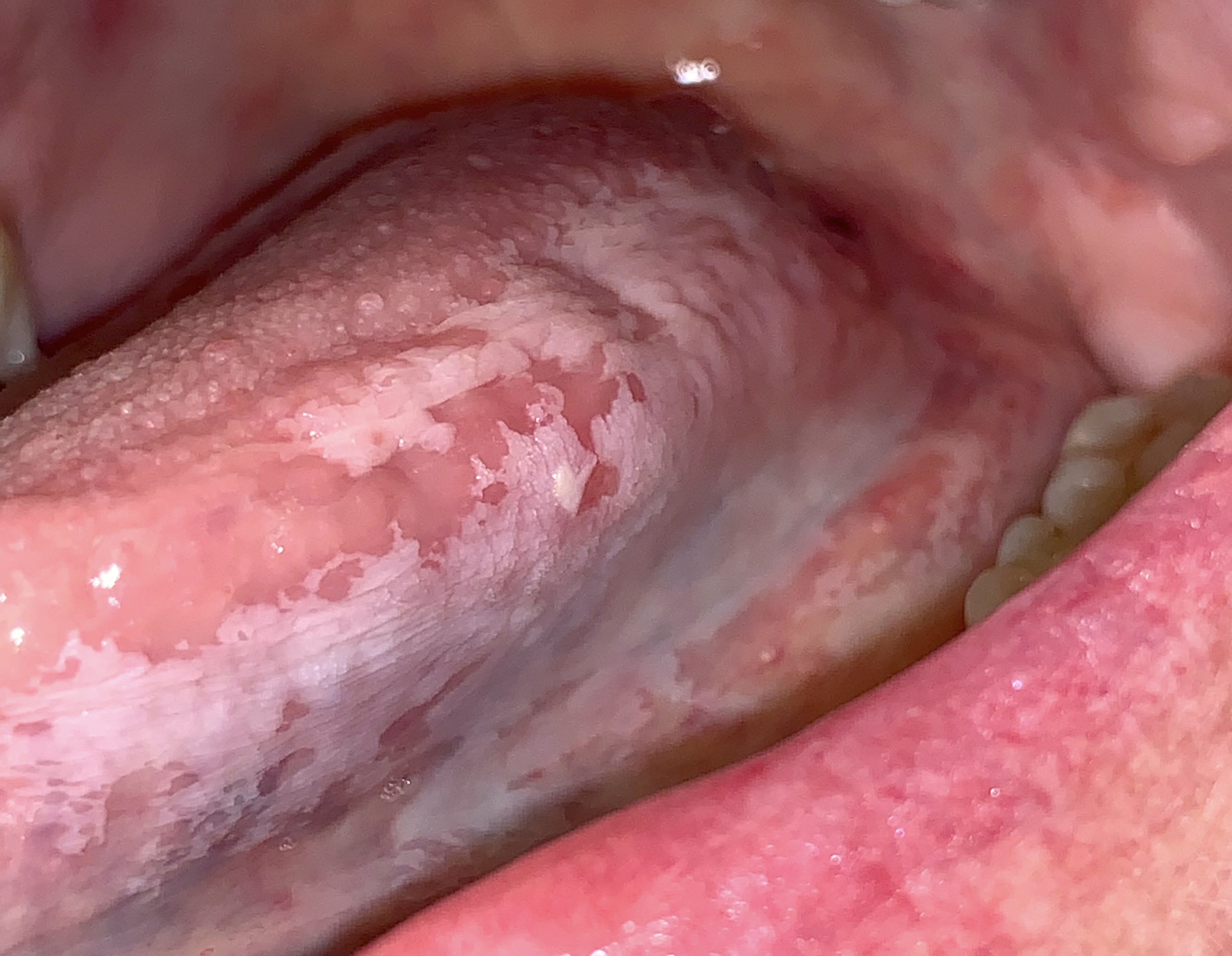
Extensive leukoplakia of tongue
Microscopic (histologic) description
- Leukoplakia with dysplasia exhibits characteristic architectural and cytological features of keratinizing dysplasia
- Features include hyperkeratosis / parakeratosis, epithelial atrophy or hyperplasia with bulbous rete ridges, basal cell hyperplasia with nuclear hyperchromasia or increased nuclear cytoplasmic ratio, variable suprabasal or atypical mitoses, dyskeratosis or glassy cytoplasm, dyscohesion
- Approximately 33% of dysplasias are characterized by an inflammatory infiltrate and should not be misdiagnosed as lichen planus (Oral Surg Oral Med Oral Pathol Oral Radiol 2014;117:511)
- Leukoplakia without dysplasia exhibits hyperkeratosis with no histologic features of a frictional / reactive process but is otherwise less well characterized
- Histologic features include (Head Neck Pathol 2019;13:423):
- Compact hyperkeratosis with hypergranulosis
- Subtle verrucoid architecture
- Epithelial atrophy or hyperplasia
- If the periphery of the leukoplakia is sampled, hyperkeratosis will appear sharply demarcated
- Histologic features include (Head Neck Pathol 2019;13:423):
- Some leukoplakias without dysplasia may exhibit prominent verrucous architecture and be reported as verrucous hyperplasia
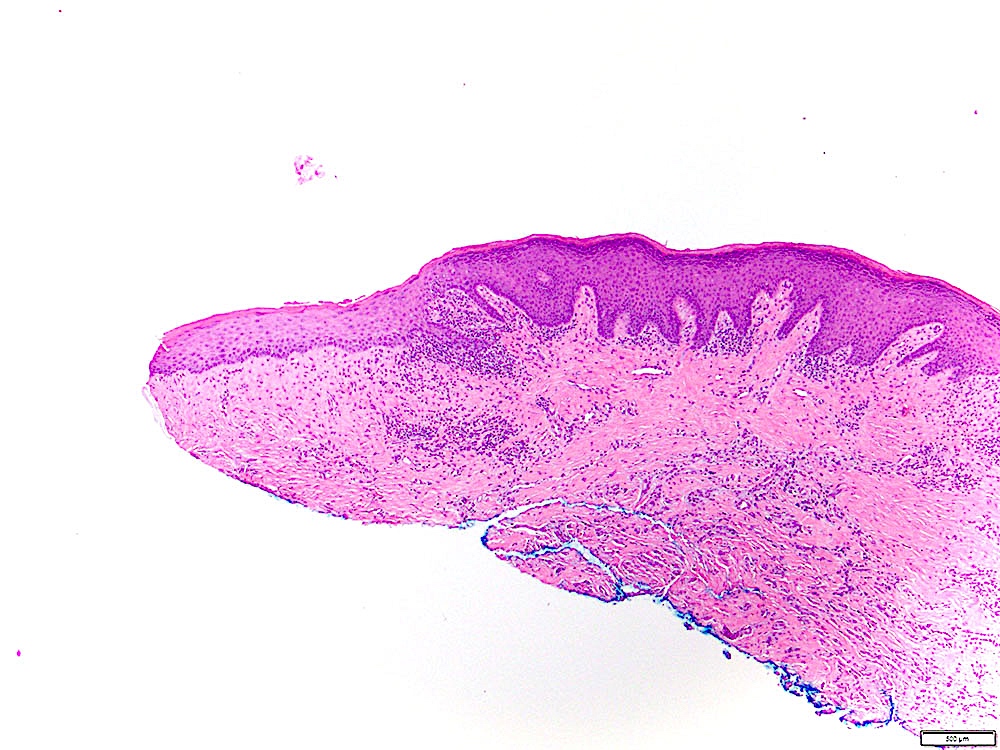
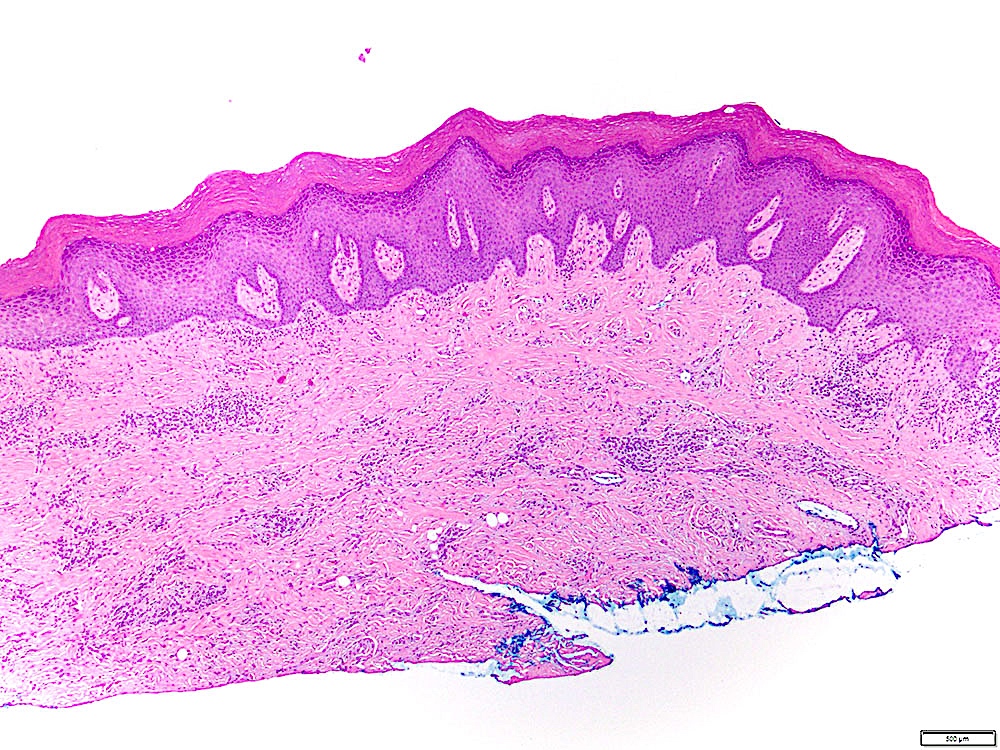
Microscopic (histologic) images
Contributed by Ivan J. Stojanov, D.M.D., M.M.Sc.
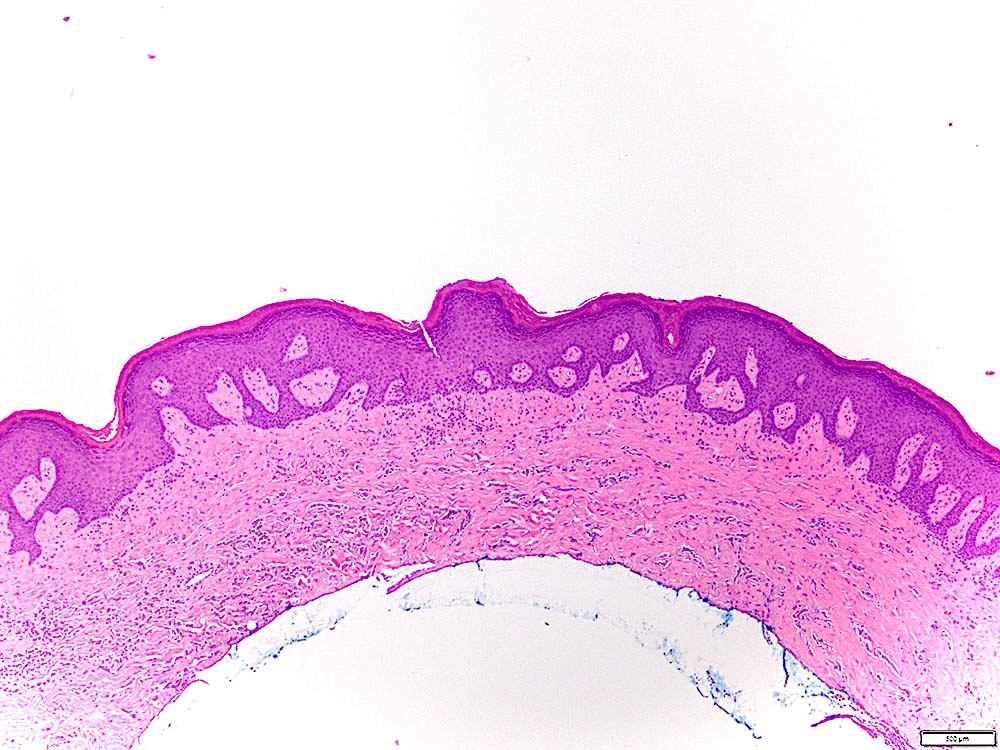
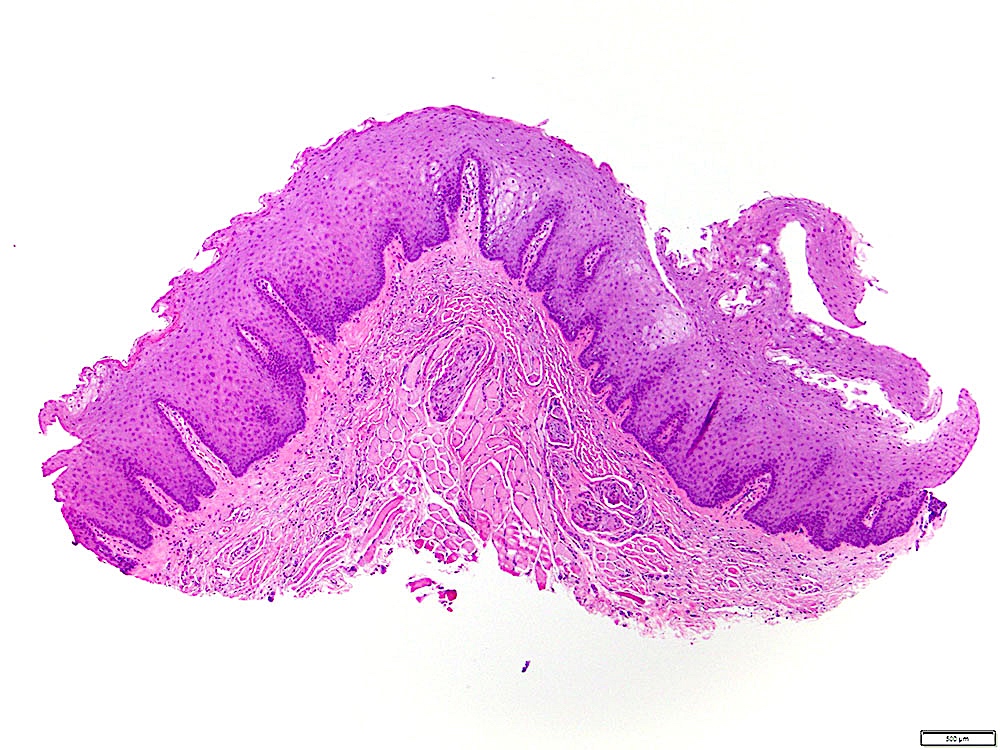
Undulating / verrucoid surface architecture
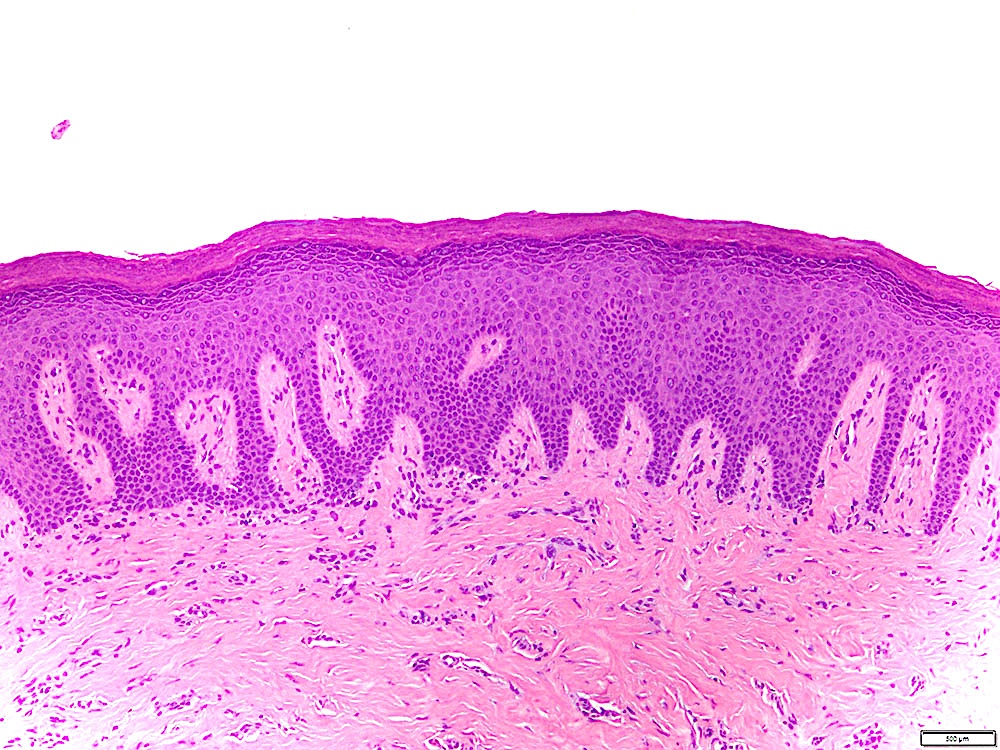
Absence of epithelial atypia
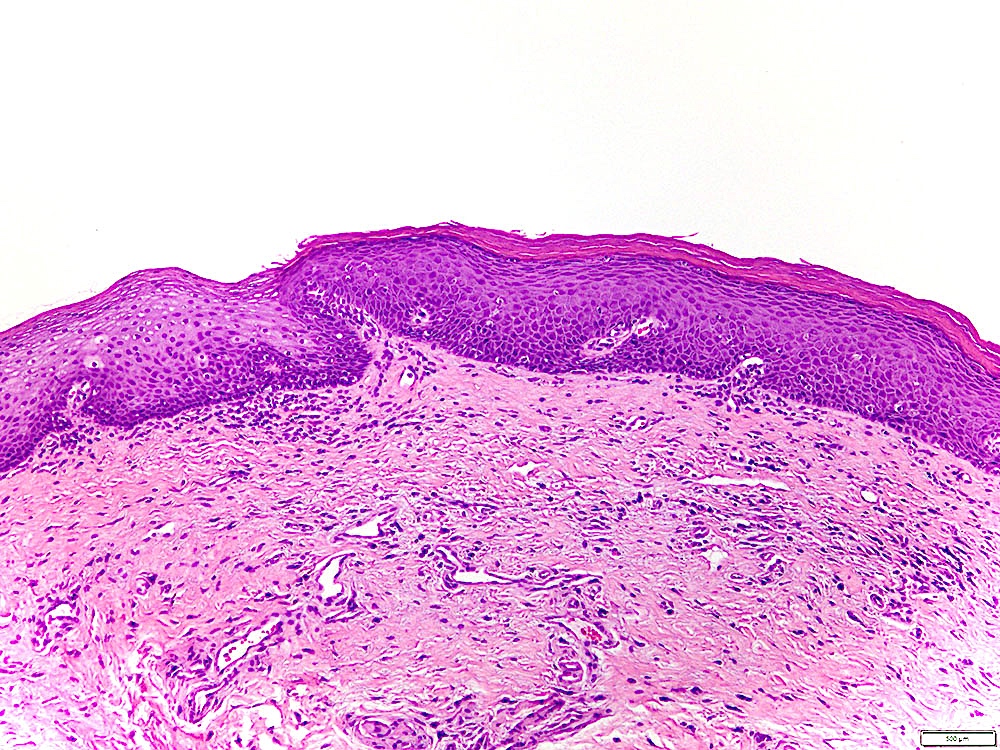
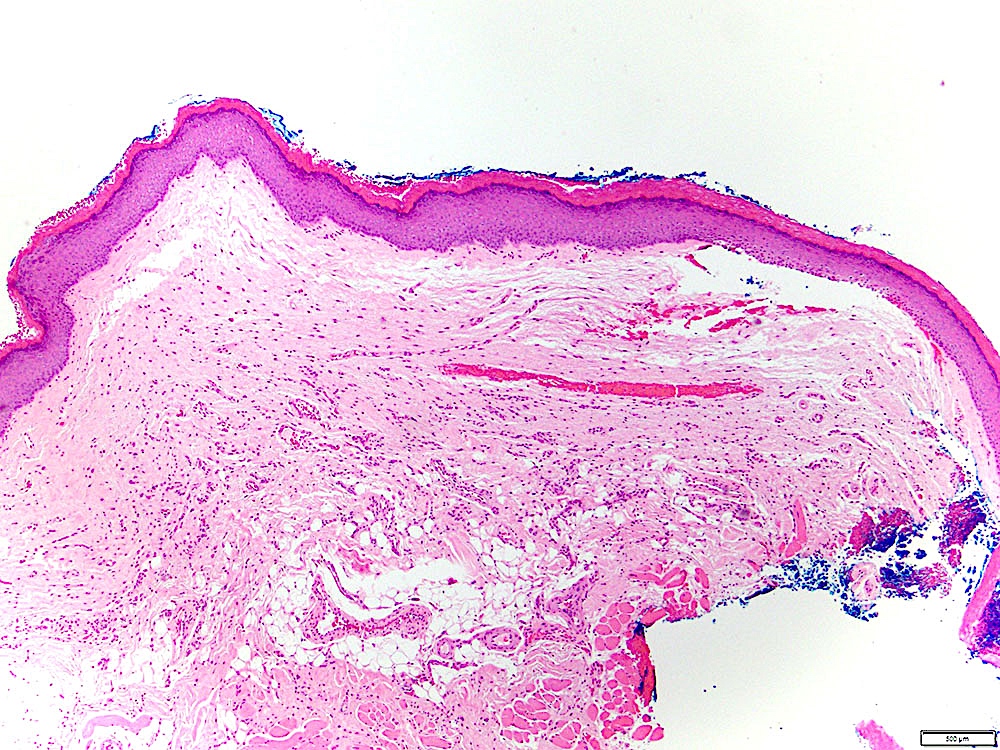
Sharply demarcated hyperkeratosis
Verrucous hyperplasia
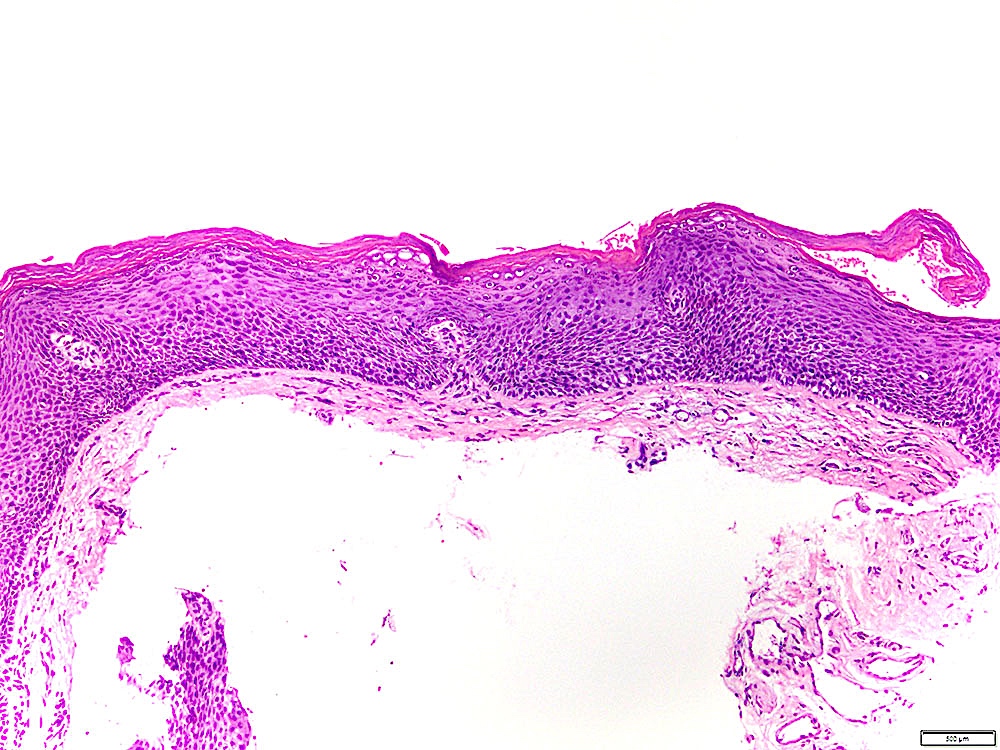
Leukoplakia periphery
Moderate dysplasia
Leukoplakia with no dysplasia
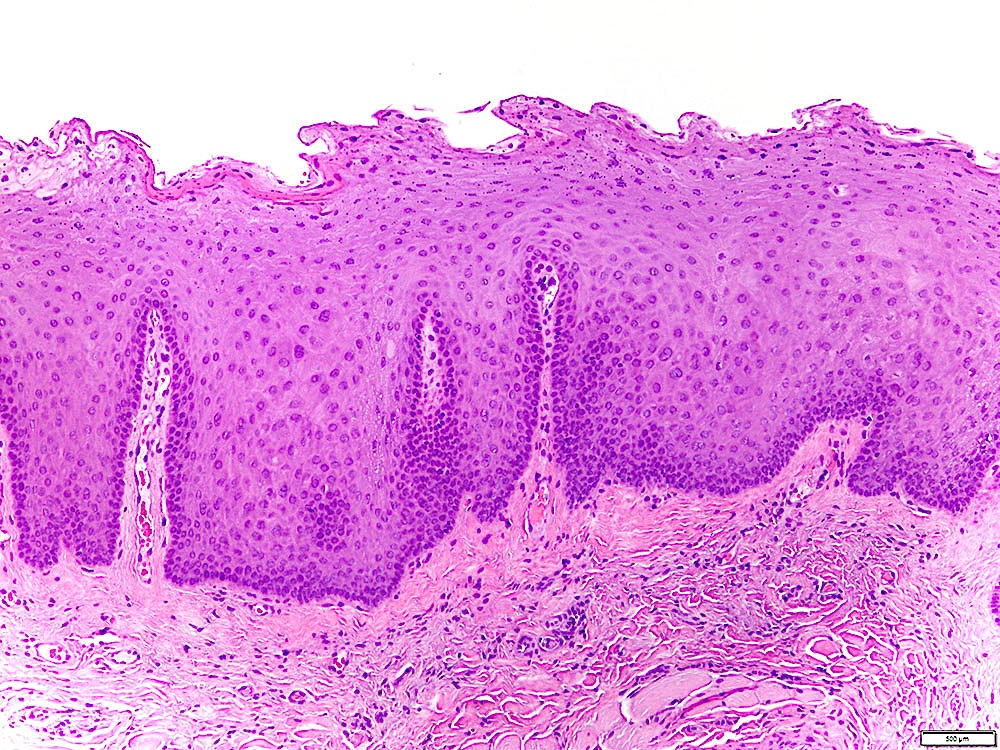
Parakeratosis and epithelial hyperplasia
Hyperkeratosis and epithelial atrophy
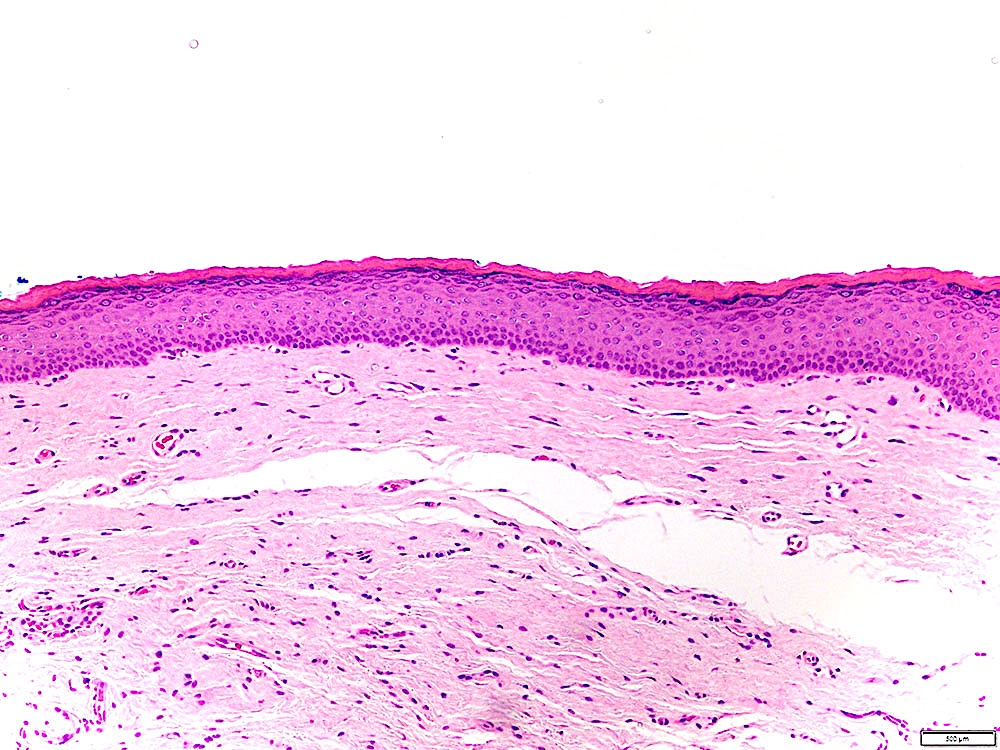
Minimal cytologic dysplastic features
Cytology description
- Currently limited role for cytology:
- Difficulty sampling adequate tissue in unanaesthetized patients
- Epithelial atypia, if present, difficult to classify as reactive or dysplastic in absence of architectural features
- Patterns of keratinization cannot be assessed
- Oral cavity sites readily amenable to incisional biopsy
Molecular / cytogenetics description
- See Pathophysiology
Molecular / cytogenetics images
Images hosted on other servers:

CGH leukoplakia versus SCC

Genes implicated in malignant transformation
Sample pathology report
- Mandible, gingiva, incisional biopsy:
- Hyperkeratosis, epithelial atrophy and mild chronic inflammation, not reactive (see comment)
- Comment: The hyperkeratosis exhibits no features of a frictional / reactive process and resembles the surface keratinization commonly seen in epithelial dysplasias. Cytologic atypia is minimal / absent in this specimen but leukoplakia without dysplasia (hyperkeratosis that is not reactive) has malignant transformation rates of approximately 5%, similar to that of leukoplakia with mild dysplasia. The findings are consistent with the clinically observed leukoplakia, which in approximately 60% of cases presents without dysplasia. If the clinical context is appropriate, proliferative (verrucous) leukoplakia may also be considered.
Differential diagnosis
- Benign alveolar ridge keratosis:
- Histologic features similar to lichen simplex chronicus
- Epithelial hyperplasia with verrucous / undulating surface and wedge shaped hypergranulosis
- Compact hyperkeratosis that tapers towards the edges and is not sharply demarcated
- Elongated rete ridges, occasionally confluent at tips
- No epithelial atypia
- Fibrosis and sparse chronic inflammation
- Chronic frictional / factitial keratosis:
- Shaggy / macerated parakeratosis with superficial bacterial colonization
- Epithelial hyperplasia with keratinocyte edema but no epithelial atypia
- Variable fibrosis, acute and chronic inflammation and leukocyte exocytosis
- Lichen planus / lichenoid mucositis:
- Squamatization / degeneration of the basal cell layer with Civatte bodies (dyskeratotic keratinocytes)
- Band-like lymphoplasmahistiocytic infiltrate in the superficial lamina propria with leukocyte exocytosis and spongiosis
- Proliferative (verrucous) leukoplakia:
- Characterized clinically by multifocal leukoplakia
- Gingival involvement common
- Predilection for middle aged / elderly females and with no / minimal tobacco or alcohol exposure
- Reason for this association is unclear
- Indistinguishable histologically from leukoplakia
- Verrucous epithelial architecture common but not necessarily present
- Characterized clinically by multifocal leukoplakia
Practice question #1
A 57 year old male smoker presents with a leukoplakia on the left ventral tongue. What is the most important predictor of malignant transformation?
- Duration
- Homogenous appearance
- Nonhomogenous appearance
- Presence of epithelial dysplasia on biopsy
- Size
Practice answer #1
Practice question #2
Which of the following is true regarding leukoplakia without dysplasia?
- It can be readily recognized by histologic features of a frictional / reactive process
- It can undergo malignant transformation
- It is usually associated with HPV infection
- It is diagnostic of proliferative (verrucous) leukoplakia
- It is rarely encountered in leukoplakia biopsies
Practice answer #2
